![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
52 Cards in this Set
- Front
- Back
|
Suppurative (purulent) inflammation |
-Predominantly neutrophils -Pyogenic (pus forming) bacteria |
|
|
Mononuclear or granulomatous |
-Macrophages, lymphocytes, and/or plasma cells -Granulomas evoked by organisms that resist eradication and stimulate T cell mediated immunity -Granulomas comprised of activated epithelioid macrophages which fuse to form giant cells combined with lymphocytes +/- necrosis |
|
|
Cytopathic cytoproliferative reaciton |
Usually produced by viruses - intracellular, use host machinery + damage host cells |
|
|
Tissue necrosis |
-Gangrenous necrosis due to powerful toxins -Ex: C. perfringens |
|
|
Chronic inflammation and scarring |
caused by many infections |
|
|
Potential anatomic distributions of pulmonary infections |
Lobar vs lobular/bronchopneumonia |
|
|
Types of CAP |
Bacterial Atypical Viral |
|
|
Causes of healthcare associated pneumonia |
-S. aureus (methicillin resistant) -Pseudomonas aeruginosa |
|
|
Causes of aspiration pneumonia |
Anaerobic oral flora admixed with aerobic bacteria |
|
|
Characteristic of chronic pneumonia? |
Granulomatous |
|
|
Necrotizing pneumonia + lung abscess - causes |
-Anaerobic bacteria +/- aerobic infection -S. aureus, Klebsiella pneumoniae |
|
|
Causes of pneumonia in immunocompromised hosts |
-CMV -Invasive aspergillosis |
|
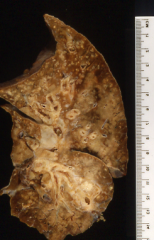
Anatomic distribution of pneumonia? |
Lobar |
|
|
With aspiration pneumonia, where do you find problems if pt is upright vs supine? |
Upright = R middle/lower lobe Supine = R upper lobe, posterior segment |
|
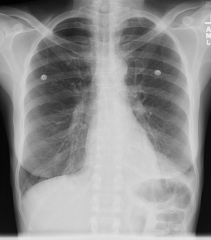
Anatomic distribution of pneumonia? |
L lower lobe pneumonia |
|
Anatomic distribution of pnuemonia? |
Bronchopneumonia (aka Lobular) |
|
|
Pulmonary defense mechanisms against bacteria |
Cough reflex Mucociliary escalator Secretions Macrophage function Immune system |
|
|
When is the cough reflex impaired? |
Coma, alcohol, NM disorders, drugs, pain |
|
|
What is the mucociliary escalator impaired? |
-Primary ciliary dyskinesia -Cigarette smoke -Gases -Viral infections |
|
|
When are secretions impaired? |
CF Obstruction (COPD) |
|
|
When is macrophage function impaired? |
Alcohol Tobacco smoke |
|
|
Features of an acute bacterial infection |
-Intra-alveolar -Acute inflammation -Fibrinopurulent debris (neutrophils) |
|
|
Features of subacute bacterial infection |
-Macrophage infiltrate (mononuclear) -Fibroblast proliferation -Advanced organizing pneumonia |
|
|
Abscess formation from bacterial infection - define + causes |
-Local suppurative process that produces necrosis of lung tissues -Mechanisms: aspiration of infective material, antecedent lung infection, septic embolism, neoplasm - post-obstructive pneumonia -Others: trauma, spread from neighboring organs, hematogenous seeding |
|
|
Complications from bacterial pulmonary infections |
-Abscess -Spread beyond lungs -Bronchopleural fistula -Empyema -Fibrosis -Bronchiectasis |
|
|
Non-viral cause of viral-like pneumonia |
-Mycoplasma pneumoniae -Chlamydia pneumoniae and C. psittaci (ornithosis) -Coxiella burnetti (Q fever) |
|
|
Opportunistic viral pathogens |
Varicella Herpes CMV |
|
|
Viral infections - upper respiratory tract findings |
-Mucosal hyperemia and swelling -Lymphocplasmacytic infiltrate (not neutrophils) -Overproduction of mucus secretions (due to damaged cells) -Predisposes to secondary bacterial infections |
|
|
Histology findings associated with viral pulmonary infections |
-Interstitial process -Chronic inflammation -Necrotizing bronchiolitis |
|
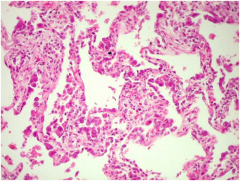
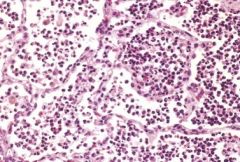
Viral or bacterial process? |
Viral - intersitial |
|
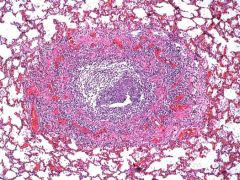
viral or bacterial process |
Viral - necrotizing bronchiolitis |
|
|
Cytopathic effects seen with viral infections? |
Multinucleated giant cells (formation of syncytium) |
|
|
Classic CMV cell findings? |
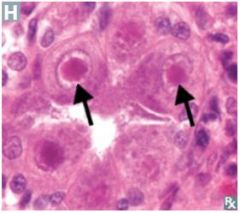
-Characteristic Cowdry Type A intranuclear inclusions (Herpesvirus) -"Owl eye" appearance of cells |
|
|
Viruses that cause multinucleated syncytia? |
RSV + HSV |
|
|
Morphology of bacterial vs viral infections (histo findings) |
-Bacterial: intra-alveolar, acute inflammation, +/- necrosis -Viral: chronic inflammation, necrotizing bronchiolitis, cytopathic effect |
|
|
Fungal infections - possibilities in healthy vs immunocompromised ppl |
Healthy: histoplasma, blastomyces, coccidioides, cryptococcus Immunocompromised: aspergillus, zygomycetes (mucormycosis), candida, pneumocystitis |
|
|
Common histo finding seen with fungal infections? |
Granulomas |
|
ID features of a granuloma |
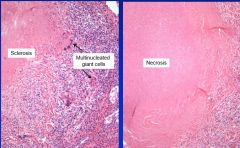
Don't confuse multinucleated cells here with those from cytopathic effect (virus) -- would NOT see granulomas with a virus |
|
|
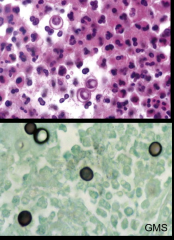
Morphologic features of histoplasmosis |
-3-5 um thin wall yeast forms -Narrow based budding yeast |
|
|
Distribution/acquisition of histoplasmosis |
Inhalation from soil contaminated with bird or bat droppings Ohio-Mississippi River Valleys |
|

Organism? |
Histoplasmosis - fungus |
|
|
Morphology of coccidioidomycosis? Clinical presentation? Distribution? |
-Thick walled non-budding 20-60 um spherules with endospores (big) -Granulomas +/- pyogenic reaction (neutrophils) -Develop delayed type hypersensitivity reaction -SW and W US |
|
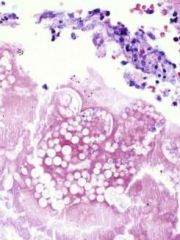
Organism? |
Coccidioidomycosis (see endospores + thick wall) |
|
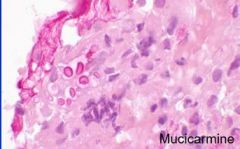
Organism? What is being stained? Symptoms you would see in infected patient? |
Cryptococcus - stain highlights mucin in the capsule; pt would have pneumonia + neuro symptoms and immunocompromised |
|
|
Morphology of blastomycosis |
-5-15 um thick wall yeast forms -Broad based budding (Bs) -Suppurative granulomas |
|
|
Reservoir + distribution of Blastomycosis |
-Soil inhabiting fungus -Central and SE US |
|
For a necrotizing, caseating granuloma, would not NOT be on the differential diagnosis? |
Mycoplasma pneumoniae - would resemble viral infection which does not have granulomas |
|
|
TB pathogenesis - before initiation of cell mediated immunity |
Mycobacterium is taken into phagosomes - see maturation arrest, lack of acid pH, ineffective phagolysosome formation Unchecked bacillary proliferation in the phagolysosome --> bacteremia with seeding of multiple sites |
|
|
Initiation and consequence of cell-mediated immunity - TB pathogenesis |
Alveolar macrophages send IL-12 to recuirt T cells T-cells release IFN-gamma to activate macrophages --> leads to phagolysosome maturation and activation, production of NO, production of reactive oxygen species, autophagy --> leads to monocyte recruitment and granuloma formation |
|
|
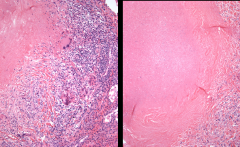
Primary tuberculosis |
-Inhalation -Formation of a Ghon complex: Ghon nodule/lesion in the periphery seeds the lymphatics, when lymph node is also involved called a complex -Minority progress (most are healed, scar) |
|
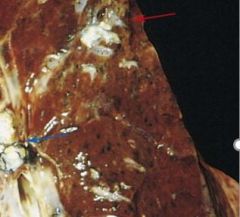
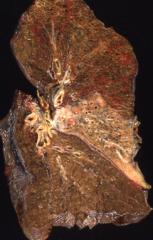
Primary or secondary TB? |
Primary TB - see Ghon lesion in the periphery (subpleural) |
|
|
Secondary tuberculosis |
-Reactivation (or huge second inoculum) -Lung apex involved (high O2 content) (different from primary) -Manifestations: fibrocalcific scar, cavitary TB (if you can't make a scar, for ex immunocompromised), fibrocaseous TB, miliary TB (small reaction around the blood vessels), TB pneumonia, pleural involvement, spead beyond the lungs |