![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
61 Cards in this Set
- Front
- Back
|
Inheritance of CF |
AR |
|
|
Organ systems affected by CF |
-Pulmonary -Pancreas -Hepatic -Sweat glands -GI tract -Vas Deferens |
|
|
Lifespan of CF |
Median 41.6 years |
|
|
Racial prevalence of CF |
~85% Caucasian, 8.5% Hispanic, 4.6% African American |
|
|
CF gene and CFTR protein |
CF gene (chromosome 7) codes for CFTR (cystic fibrosis transmembrane conductance regulator) - membrane protein that regulates salt transport |
|
|
Diagnosis of CF |
-Positive sweat Cl- (>60 mM) and -Positive genetics and -Organ manifestations: GI tract/nutrition, sino-pulmonary, liver, male repro tract, sweat gland |
|
|
How does CF cause high salt in sweat? |
-Normally, most Na and Cl are transported out of sweat glands before they reach skin surface (low salt on skin surface) -With CFTR not functioning, all of the NaCl in the sweat glands are transported to the skin surface |
|
|
Source of mucus in the respiratory tract |
-Mucins in goblet cells (predominantly MUC5AC) -Mucins in submucosal glands (predominantly MUC5B) |
|
|
Abnormal CFTR in the airways leads to... |
cilia that are not able to effectively clear mucus out |
|
|
How does CFTR progress to CF disease? |
-Loss of CFTR leads to: decreased Cl- transport, decreased HCO3 transport, increased Na transport via ENac (overabsorption of sodium contributes to dehydration) -Mucus defects -Downstream effects: infection, inflammation, airway damage |
|
|
Na and Cl transport in normal and CF epithelium |
-Normal: normal chloride and sodium absorption, transcellular CFTR present, normal ASL (airway surface liquid) height (7 um) -CF condition: reduced height/volume of ASL (airway surface liquid) interrupts clearance, chloride absorbed between cells, too much Na reabsorption |
|
|
Findings in the mucus layer of CF airway |
-Extracellular DNA from neutrophils increases mucus viscosity -Increased osmotic pressure compresses PCL (brush border) -Tethering causes mucous buildup -Defective CFTR causes mucus dehydration |
|
|
Key pathology of CF lung disease? |
Bronchiectasis (obstructive disease) |
|
|
FVL appearance for CF? |
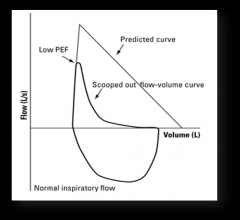
Obstructive pathway |
|
|
Targets for CF treatment |
-CFTR modulators - gene transfer, gene/RNA editing -Hydration of mucus -Anti-inflammatories -Antimicrobials |
|
|
Survival with CF? |
Pts born with CF later survive longer due to improved therapies However rate of decline of FEV1 is still the same regardless of longevity |
|
|
Age of death for CF patients? |
Mid-20s Bimodal component of survival |
|
|
Four components of pulmonary pathology in CF |
-Ion transport -Plugging -Infection -Inflammation All lead to progressive lung damage |
|
|
Evidence-based tx of CF lung disease |
-Airway clearance (hand, vest, autogenic) - usually at least 2x day -Mucus hydration -Mucolytics -Infection (antimicrobials) - prevent acquisition, chronic infection, acute exacerbation -Inflammation (anti-inflammation) |
|
|
RhDNase in CF |
-Mucolytic -First FDA approved drug for CF -Reduction in age-adjusted risk of pulmonary exacerbation -Increased lung fxn |
|
|
Hypertonic saline in CF |
-7% hypertonic saline (Compliance issues) -Hydration -Improved lung fxn and clinical stability |
|
|
Lung infections in CF with age |
-S. aureus most prevalent overall, especially in kids
-Pseudomonas prevalence increases with age -MRSA: peaks around young-adulthood -H. influenzae - in young children |
|
|
Infection with pseudomonas and progression of CF lung disease |
-Transient bacterial infection early in life - either eradication or progress to chronic bacterial infections -Inflammation starts with these transient bacterial infections and increases -Chronic bacterial infections lead to mucoid/biofilm, bacterial infection -- this leads to irreversible lung damage and increase in inflammation |
|
|
Age-specific prevalence of Pseudomonas from birth-age 16 |
-No PA: rapidly declines within first years of life -Non-mucoid PA only - majority of patients between ages 1-10 yrs old (transient colonization) -Mucoid PA +/- nonmucoid PA - increases with age (age 10+) |
|
|
Two terms to associate with pseudomonas? |
Mucoid + biofilm |
|
|
There is an association of mucoidy with ____ |
drop in FEV1% moreso than non-mucoid pseudomonas |
|
|
Additional mechanisms of virulence and antibacterial resistance in Pseudomonas besides mucoid and biofilm |
-Type III secretion system -Other secreted factors: Exotoxin A, Proteases, Phenazines -Efflux pump -Flagellum -B-lactamase, porins, increase of pumps to pump beta-lactams out (efflux) |
|
|
Oral antibiotics for Pseudomonas |
-Ciprofloxacin -Levofloxacin -Trimethoprim/sulfamethoxazole -Azithromycin -Minocycline |
|
|
Aerosolized antibiotics for Pseudomonas |
-Tobramycin -Colistin -Aztreonam lysine -Otherparenteral antibiotics |
|
|
Parenteral antibiotics for Pseudomonas |
-B-lactam related: ticarcillin, ticarcillin-clavulanate, ceftazidime, piperacillin/tazobactam, meropenem, imipenem, aztreonam arginine, cefepime -Aminoglycosides: amikacin, tobramcyin, gentamicin |
|
|
Tombramycin |
Aerosolized antibiotic for Pseudomonas -Improvement in lung function -Decrease in hospitalization -Decrease in IV antibiotics -Reductions in PsA density - declining effects over time vs placebo, independent of PsA resistance pattern |
|
|
Acute pulmonary exacerbations are ____ events |
sentinel events - 25% of pts fail to recover lung fxn |
|
|
Burkholderia cepacia |
-Complex organism -Inherently high resistance to antibiotics -Higher mortality compared with Bcc negative patients (~9yr shorter survival) -Transmissible |
|
|
Infection control in CF |
-Infectious risk is ubiquitous -CF bacteria: can be spread person to person -Methods of control: hand washing, care of equipment, masks, limited exposure, cohort patients, no sharing respiratory equipment |
|
|
Lung inflammation in CF |
-Early, dramatic, relentless -Multiple contributors in lower airways |
|
|
Sputum inflammation |
CF sputum enriched with inflammatory biomarkers Neutrophils, cytokoines, chemokines, elastase, bacterial load Sputum biomakers track with disease |
|
|
Azithromycin |
-Has unique anti-inflammatory properties -May kill Pseudomonas in stationary growth phase -Improvement in Lung fxn and Decrease in pulmonary exacerbations in patients with Pseudomonas -Even without Pseudomonas, reduction in lung exacerbations, increase in body weight, less cough and less productive cough |
|
|
Antibiotics can also work as ____ |
anti-inflammatories |
|
|
Nutrition in CF |
-Pancreatic insufficiency -High caloric needs -Diabetes -Use enzyme replacements, supplements, insulin |
|
|
Vitamin deficiencies in CF |
Fat soluble vitamins (ADEK) due to pancreatic insufficiency - supplements |
|
|
Liver disease in CF |
Cirrhosis - bile acid flow agents Only clinically relevant in 5-10% of pts |
|
|
Male infertility in CF |
Problem in vas deferens |
|
|
Other chronic conditions found in CF patients |
-CF-related diabetes (islet cell dysfunction) -Depression -Bone disease |
|
|
Lung transplantation in CF |
-Relatively common (1/3 of all lung transplants) -Outcomes not as good as other organs: 1) High exposure to cardiac output 2) Contact with the environment 3) Immunity reasons -CF survival better than other lung disease with lung transplants |
|
|
Newborn screening for CF |
Associated with... -Improved growth -Improved cognitive fxn -Reduced time to diagnosis -Reduced catastrophic hospitalization costs -Risks of early pseudomonas colonizaiton (clinic exposure) (concern, but no longer an issue) |
|
|
What is CFTR and how does it work? |
-Traffic ATPase -Two transmembrane domains, two nucleotide binding domains, one regulatory domain -Anion channel: Cl-, HCO3-, SCN-, GSH, others? |
|
|
CFTR modulators targerts |
-Potentiator: improves gating (opening of CFTR) -Corrector: improves trafficking/folding -Suppressor: suppresses stop codon, improves surface CFTR -Stabilizer: improve surface CFTR -Amplifier: increase RNA substrate |
|
|
What are the channel factors that influence CFTRs anion transport? |
-Number of channels at the plasma membrane (N) -How much time each channel spends open vs closed (Po) -Size of each chloride channel (G) N x Po x G = total Cl- transport |
|
|
Matching CFTR modulator strategies to mutations |
-Gating mutation - use potentiator -Folding mutation - use corrector -Stop codon mutation - use suppressor |
|
|
Where do modulators come from? |
-Agents in current clinical trials discovered via high throughput screening -Use of cell lines (stably expressing CFTR or reporter gene) |
|
|
G551D CFTR |
-3rd most common disease-causing mutation -Problem with open channel probability (gating) -Strategy - increase Probability of (Ivacaftor) |
|
|
Restoring airway epithelial cell functions with Ivacaftor |
-Improvement in reduced ASL (airway surface liquid) volume/height found with CFTR -Ciliary beat frequency is normalized |
|
|
Efficacy results of Ivacaftor |
-Risk of exacerbation decreased -QOL increase -FEV1 increase -Weight - gained (good) -Decrease in sweat chloride |
|
|
F508del CFTR activity |
-Most common mutation in CF -Mutation in NBD-1 -Destabilized protein folding - failure of later motifs to compact, driven by proximal/distal interactions -Failure to mature and acquire full glycosylation -ERAD and proteosomal degradation |
|
|
Two problems idenfitied that contribute to folding defect with F508del mutation |
1) Co-translational folding of NBD-1 2) Domain assembly (interactions between NBD-1 and ICL4) |
|
|
How to correct f508del CFTR? |
-Increase N (number of channels) -VX-809 (Lumacaftor) |
|
|
Correcting AND potentiating F508del |
-Increase N and Po (Lumacaftor + Ivacaftor) -See FEV1 improvement -See decrease in acute pulmonary exacerbations |
|
|
Two drugs approved for use in CFTR? |
-Ivacaftor -Lumacaftor -Gating mutations in CFTR treated with ivacaftor -F508del treated with ivacaftor + luvacaftor |
|
|
Adherence rates with CF treatments |
-Reported adherence rates typically 50-60% -Can be as low as 30% for inhaled medications and chest clearance -Unwitting adherence: mistakenly feel that they are adherent -Erratic adherence: patient understands/agrees with therapy but has difficulty maintaining adherence -Intelligent: patient deliberately alters/discontinues therapy |
|
|
Approaches to adherence based on etiology |
-Unwitting: re-educate, reinforce -Erratic: cues, problem solving, prioritize -Intelligent: deeper understanding of choices |
|
|
Components of Kalydeco and Orkambi |
Kalydeco = ivacaftor Orkambi = ivacaftor/lumacaftor combo |