![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
24 Cards in this Set
- Front
- Back
- 3rd side (hint)
|
Focal point |
Đầu mối |
|
|
|
Advocate |
Ủng hộ |
|
|
|
Unity |
Đoàn kết |
|
|
|
Advocacy |
Chủ trương |
|
|
|
Nociceptive |
Đau thụ thể There are 3 types of pain: nociceptive, neuropathic and nociplastic. Nociceptive pain is a normal response to an insult to the body, something that is perceived as dangerous, like a burn or appendicitis. Neuropathic pain is pain from an injury or disease to the peripheral or central nervous system. Nociplastic pain is when the pain is not nociceptive, it is not neuropathic, and it is a malfunction of the pain system, it's altered state of nociception. |

|
|
|
Acceptance and commitment therapy ACT |
This therapy emphasizes the importance of accepting pain, and focusing on goals that are important to that person. This is very goal-oriented and personalized. I don't have time to marinate in the misery anymore. |
|
|
|
SySADOA |
Symptomatic slow acting drugs of OA Only diacerein: benefit outweigh its risks.
Glucosamine sulfate Chondroitin sulfate
Glucosamine, chondroitin sulfate or the combination are marketed for supporting joint health. They have also been widely used for treating OA. The preponderance of evidence indicates little of no meaningful effect on pain and function. Doubt in efficacy... No meaningful effect. Recommend not using.
|

|
|
|
Meralgia paraesthetica |
Mơ rá gia, para es the địc. Đau đùi dị cảm. Lateral femoral cutaneous nerve. Dây thần kinh bì đùi ngoài (L2-3) bị chèn ép gây ra các triệu chứng đặc trưng như ngứa ran, đau châm chích (tingling, pins), tê bì đùi (numbness) và nóng rát (burning pain), or electrical shock ở mặt ngoài đùi. tight belts, tight underwear, who have fat adipose tissue... Light touch, pinprick, hot and cold sensations. Allodynia: loạn cảm đau. Có thể gởi bệnh nhân làm Nerve conduction study. Ko mặc quần bó sát. Ko đứng hoặc đạp xe trong tgian dài. Béo phì. Mang thai. Giảm đau, giảm cân. Quần áo thoải mái. Bài tập con mèo. Bird dog. Bài tập chùng chân (lunges) Bài tập bắt cầu. Bridge
|
|
|
|
Coccydynia |
Đau xương cụt. Injury to the tailbone after a fall. Or woman after she gives birth to a child. What can you do to alleviate coccydynia? Have function in holding mang muscles and ligaments in the pelvic floor. During childbirth, the coccyx is pushed backward to make space for the baby to pass. Person who spends too much time sitting on a hard surface, like concrete, or hard chair. It seems there is some advantage to having some fat around the coccys. Some people start having tailbone pain when they have Rapid weigh loss. (Losing the cushioning that protects the coccyx). Refered pain from another nerve root or internal pelvic organ. Infection or tumor of the coccyx. Most cases of coccydynia improve spontaneously without any medical intervention. It may take 2 to 3 months for the pain to get better. 90% Don't need xray or investigation if the pain is improving, without incontinence of bowel or bladder, fever, numbness. If the pain start interfering with your daily activities, like sitting for a prolonged period, defecation or sexual intercourse. Retal examination. Exam the coccyx. Mobile or not. Hypermobility, hypomobility. Normal 10-15 degree. Dynamic xray. Heat and cold. Nsaids. Topical cream. Proper sitting posture. . Coccygeal cushions. Changing the chair.Coccygeal cushions.TENS.Pelvic floor rehab. TENS. Pelvic floor rehab.
|
|
|
|
SASPC |
Somatic cơ thể ADL Social Psychological tâm lý Communication |
|
|
|
(Hyper) acute phase |
Giai đoạn tối cấp 0-24h Chẩn đoán/ điều trị / phòng biến chứng Hạn chế tổn thương tiến triển Phòng ngừa biến chứng thứ phát (viêm phổi do nuốt) Dịch chuyển sớm. |
|
|
|
Early rehabilitation phase
|
Phcn gđ sớm 24h-3 tháng.
Thiết lập lại chức năng nếu được. Nếu không: chiến lượt bù trừ. Phòng ngừa hoặc giảm các khiếm khuyết trong hoạt động và tham gia. Nếu cần: điều chỉnh môi trường và chăm sóc tại nhà. Cung cấp thông tin và giáo dục. |
|
|
|
Late rehabilitation phase |
Phcn muộn 3-6 tháng. Tiếp theo giai đoạn phcn sớm. Nhấn mạnh vào phòng ngừa và giảm khiếm khuyết trong các hạn chế về hoạt động và tham gia. Nếu cần điều chỉnh môi trường và chăm sóc nhà ở.
|
|
|
|
Chronic rehabilitation phase |
Phcn gđ mạn tính >6 tháng. Hỗ trợ: duy trì, phòng ngừa. Tối ưu hóa chức năng tham gia hoạt động xã hội. Học các thích nghi với tình trạng khuyết tật Duy trì sự khỏe mạnh thể chất. Đảm bảo chất lượng cuộc sống người bệnh. |
|
|
|
AVERT a very early rehabilitation trial |
Is a large multi-centre study on the importance of early timing in stroke rehabilitation is the AVERT trial. The AVERT trial consists of 3 phases: Phase I: gather data baseline on current practice (completed). Phase II: trial protocol tested for feasibility and safety (completed). Phase III: test for efficacy and cost-effectiveness (multi-centre, ongoing) Studies performed during phase II of the demonstrated that very early rehabilitation was feasible and safe. In addition, patients who underwent earlier and more intensive mobilization after stroke. Patients in the very early intensive mobilization group returned to walking significantly sooner than did standard stroke unit care controls. PHCN sớm an toàn và khả thi. |
|
|
|
Kết luận nghiên cứu AVERT |
Chương trình vận động sớm với cường độ thấp là tốt hơn so với vận động rất sớm với cường độ cao, thường xuyên. Người bệnh ko nên vận động quá sớm- tập thụ động trong vòng 24 giờ đầu là tốt nhất. Ko có sự khác biệt ở những người bệnh được tPA. PHCN sớm hơn, nhiều hơn có thể có hại có người bệnh chảy máu não và nhồi máu não nặng. Đặc biệt lưu ý đến những người bệnh đột quỵ nặng (NIHSS > 16 điểm). Very early mobilization was associated with a significant reduction in the odds of little or no disability at 3 months after stroke, with no evidence of accelerated walking recovery; however, the number of patients who died or had serious adverse events at 3 months after stroke did not differ significantly between groups. Our data show that an early, lower dose out-of-bed activity regiment is preferable to very early, frequent, higher dose intervention, but clinical recommendations should be informed by the future prespecified, detailed analysis of the dose-response association. |
|
|
|
4 R in osteoarthritis |
Relieve pain giảm đau Restore function bảo tồn chức năng khớp Reduce disability giảm tàn phế Rehabilitation PHCN. Non- pharmacological treatment: Education, exercises, prevention of injuries, weight loss, orthotic devices. Pharmacological treatment: Acetaminophen, NSAIDs and cox2 inhibitors, sysadoa, duloxetin, opiods. Topical: NSAIDs. Capssacin, lidocain patches. Intra-articular: corticosteroid, HA. Core set: education. Weight loss. Exercise. Ensure that positive behavioral changes, such as exercise, weight loss, use of suitable footwear and pacing, are appropriately targeted. For those who are overweight (BMI >25), a minimum weight loss target of 5-7.5% of body weight is recommended. Thermotherapy: the use of local hear or cold should be considered as an adjunct to core treatments. Electrothrapy: TENS as an adjunct to core treatment for pain relief. Water-based exercise: may be appropriate to offer aquatic exercises/ hydrotherapy for some people with knee and/or hip OA. This will depend upon personal preference and the availability of local facilities. |
|
|
|
ESCEO |
European society for clinical and economic aspects of osteoarthritis and osteoporosis |
|
|
|
Glucosamine |
Appear to be relatively safe and well tolerated when used in suggested doses over a 2-year period. May interact with wafarin. Risky for diabetes patients. Risky for patients with glaucoma. Risky for patients with HNT or kidney disease. Risky for patients who receive anti-coagulant. Risky for patients with shellfish allergy. Glucosamine acid clohydrid: xách tay Mỹ. Ko khuyến cáo. Sulfate kia mới được.
|
|
|
|
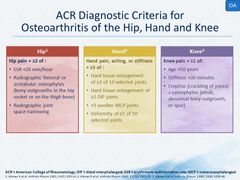
A mechanism-based approach to the management of osteoarthritis. 3 categories: 1. Those which inhibit peripheral mechanisms of pain and inflammation. 2. Those which treat central pain mechanisms. 3. Those which affect progression of joint destruction (peripheral pain generators) |
Uc che dau va viem ngoai bien Dieu tri dau trung uong. Tac dong den qua trinh huy khop (tao ra dau ngoai bien) |
|
|
|
Laboratory test results as a basis for misdiagnosis of OA- misinterpretation.
|
Factors to keep in mind include increases in: Erythrocyte sedimentation rate ESR with age (nữ thường cao hơn nam, tăng theo tuổi, lấy tuổi chia 2 là ra bt). Serum RF titer with age. Serum antinuclear anti-body ANA levels with age. Serum CRP levels with obesity. |
|
|
|
No diagnosis criteria for spinal OA |
|
|
|
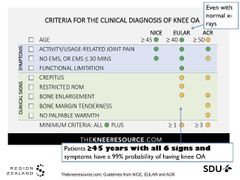
|
Diagnosis criteria of knee OA is different among Nice: national institute for health and care excellence, eular: EUropean ALiance of Association for Rheumatology and ACR: American college of rheumatology. |
|
|
|
|
DIP distal interphalangeal PIP proximal interphalangeal MCP MetaCarpoPhalangeal CMC CapoMetaCapal |
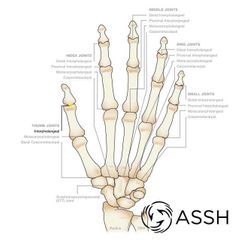
Dip Gian đốt xa Pip gian đốt gần MCP bàn ngón (RA) CMC cổ bàn |

|