![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
62 Cards in this Set
- Front
- Back
|
homeobox, or Hox genes
|
|
|
majority of rotation occurs where in the C-spine?
|
C1/C2-atlas & axis
|
|
|
majority of flex/ext occurs where in the C-spine?
|
occiput/atlas
|
|
|
majority of later bending occurs where in the C-spine?
|
c3-c7
|
|
|
which cervical vertebra does NOT have the vertebral artery?
|
C7-Vertibal artery
|
|
|
which cervical vertebra does NOT have a bifid spinous process?
|
C1 & C7
|
|
|
-17mm=nl -<13mm =compression |
|
|
where is the C8 nerve root
|
at the C7 level
|
|
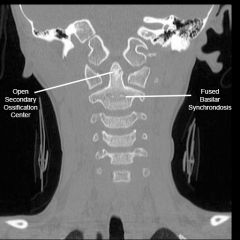
the secondary ossification center fuses to the dens at ~ age ___?
|
age 12
|
|
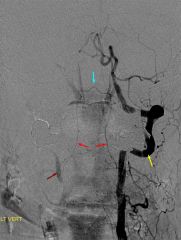
What does this image demonstrate? -why is it significant? -
|
-a vascular watershed exists between the apex and the base of the odontoid - watershed area is thought to affect healing of type II odontoid fractures-apex- internal carorid A base-vertebral A |
|
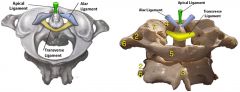
Occipital-C1-C2 Ligamentous Complex -which ligament limits anterior translation of the atlas |
transverse ligament
|
|
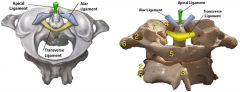
Occipital-C1-C2 Ligamentous Complex -which ligament limit rotation of the upper cervical spine
|
apical ligaments
|
|
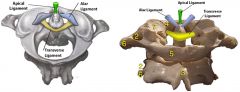
Occipital-C1-C2 Ligamentous Complex -which ligament limit rotation of the upper cervical spine
|
alar ligaments
|
|
|
C1 to C6
|
|
|
C6
|
|
|
C2-C6
|
|
|
which have a transverse foramen
|
C1-c7
|
|
|
C7
|
|
|
superior articular facets of the subaxial cervical spine (C3-C7) are oriented in a ___ direction at C3 and ___ direction at C7
|
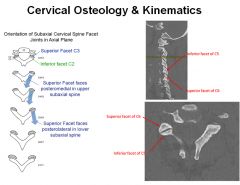
-posteromedial -posterolateral |
|
|
Range of motion is greatest at more ___, owing to the orientation of the ___
|
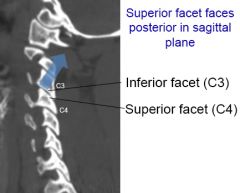
cephalad levels -facet joints. |
|
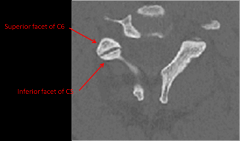
When viewed on axial imaging, the superior articular process is ___to the inferior articular process
|

-anterior
|
|
|
A 3-year old male falls from a table and is brought to the emergency room with neck pain, but no neurologic deficits. Cervical spine radiographs show a synchondrosis separating the odontoid process from the body of the axis. Which of the following best describes this radiographic finding?
|
-synchondrosis separating the odontoid process from the body of the axis is a normal radiographic finding in a 3 year old. - tip of the dens is not ossified at birth but appears at age 3 years and fuses to the dens by age 12 years |
|
|
-5 root test for sensory & reflex? - 6 nerve off of C5? what do these 6 nerve innervate? |
S-Lateral arm below deltoid R-Biceps
|
|
|
C5 root -primary motion & muscles tested? |
c5-Shoulder abduction -Deltoid |
|
|
What is a potential complication of an amputation at the level of the distal interphalangeal joint? |
A lumbrical plus finger is descibed as paradoxical extension of the IP joints while attempting to flex the fingers. In the case a lumbrical plus finger secondary to a DIP amputation, the PIP will extend upon attempted finger flexion. |
|
|
Carpal tunnel what is the most radial structure? what is the CT? |
most radial FPL - 1 consists of nine flexor tendons 2-one nerve (median nerve) 3-FPL |
|
|
which nerve lies between PL and FCR at level of the wrist flexion crease |
palmar cutaneous branch of median |
|
|
Carpal tunnel is narrowest at the level of the ___? |
hook of the hamate |
|
|
the most specific test (76%) for carpal tunnel syndrome? |
self administered hand diagram |
|
|
is the most sensitive test to diagnose carpal tunnels syndrome? |
carpal tunnel compression test (Durkan's test) |
|
|
demyelination leads to what effect to NCV ? (faster slower, increase decrease) NCV distal sensory latency of= CTS? NCV motor latencies= CTS? |
-increase latencies (slowing) of NCV -distal sensory latency of > 3.2 ms -motor latencies > 4.3 ms |
|
|
EMG test the electrical activity of ___&____? |
individual muscle fibers and motor units |
|
|
potential pathologic findings of emg with CTS suggestive of demylination? 5 |
|
|
|
nerve histology characterized by what in CTS? 5 |
|
|
|
-CTS first line of treatment? -nocturnal symptoms only? -___is a good prognostic factor that the patient will have a good result with surgery? -failure to improve following primary surgery most common reason? |
|
|
|
CTS pinch strength return in ___ weeks? grip strength is expected to return to 100% preoperative levels by ___ weeks postop |
pinch strength = 6 week grip strength =12 weeks postop |
|
|
prophylactic antibiotics, systemic or local, are____ for patients undergoing a clean, elective carpal tunnel release |
NOT indicated |
|
|
A 45-year-old man presents with a three-month history of unilateral symptoms in his right wrist and hand. He first noticed a palpable nodule over the volar aspect of his wrist about three months ago. The nodule would become painful after weekends of heavy drinking at which time he noticed tingling sensation in his index and middle fingers. He notes that ibuprofen has helped improve the pain in the past. On clinical examination, he has a palpable, painless, solid nodule over the volar aspect of his wrist. He has no motor or sensory deficits and negative carpal tunnel provocative tests. An axial CT and MRI image show atypical space occupying lesion - What would be the most appropriate next step in the management of his symptoms? |
gout. The most appropriate next step in the management of his symptoms would be referral to a rheumatologist where medical therapy, such as prophylaxis with colchicine, could be initiated. |
|
|
This guideline was subsequently endorsed by the American Association of Neurological Surgeons and the Congress of Neurological Surgeons. The guideline makes 9 specific recommendations:
|
|
|
|
carpal tunnel relationship of the FDS tendons & contains 10? Not the? |
|
|
|
EMG's detect the electrical potential generated by ____ when these cells are electrically activated. They give information about the ____ |
muscle cells -muscle motor unit |
|
|
The nerve conduction (NCV) portion of the electrodiagnostic study measures the speed at which the _____ travels down the axon. Large, ____ conduct impulses the fastest - only ____ fibers are evaluated in the nerve conduction portion of the electrodiagnostic study. |
nerve impulse myelinated nerve fibers myelinated nerve fibers |
|
|
General parameters for NCV diagnosis of carpal tunnel syndrome include ___ of >4.5 msec, a ____ of >3.5msec, or a ____ of < 52 m/sec. |
a distal motor latency distal sensory latency -conduction velocity |
|
|
___&___ are measured with NCV's. EMG's detect the ___ generated by muscle cells when these cells are ___. |
Distal latencies and conduction velocities -electrical potential -electrically activated |
|
|
A 45-year-old carpenter complains of difficult gripping a hammer, which worsens with repeated use. On physical exam, he is able to passively flex the proximal interphalangeal (PIP) joint when the metacarpophalangeal (MCP) joint is flexed but not when the MCP joint is extended. What is the most likely explanation? |
patient exhibits a positive Bunnell test, indicative of intrinsic tightness, which commonly affects those who use objects that require repetitive grip. |
|
|
positive test when PIP flexion is less with MCP extension than with MCP flexion =what test? |
Bunnell test (intrinsic tightness test |
|
|
___ is characterized by an active flexion lag in fingers adjacent to a digit with a previously injured or repaired flexor digitorum profundus tendon. |
Quadrigia effect |
|
|
____ is limited MCP flexion secondary extensor tendon adhesion to bone. |
Extrinsic tightness |
|
|
____ would result in a Boutonniere deformity. |
Central slip rupture |
|
|
_____is paradoxical PIP extension during active finger flexion. |
Lumbrical plus |
|
|
Chronic injury to what anatomic structure can lead to a boutonnière deformity of the finger? |
central slip of the extensor tendon |
|
|
A 54-year-old female presents with a hand deformity. A surgical procedure is being considered that relocates the lateral bands dorsally to counteract the pathophysiology of the deformity. Which of the following deformities does this patient most likely have? |
Boutonniere deformity is characterized with the PIP in flexion and the DIP in hyperextension |
|
|
Primary lesion is lax volar plate that allows hyperextension of PIP? |
Swan Neck Deformity |
|
|
A finger deformity caused by disruption of the terminal extensor tendon distal to DIP jointthe disruption may be bony or tendinous? |
Mallet Finger |
|
|
A 16-year-old football player sustains an injury to his ring finger after making a tackle. A clinical photograph is shown demonstrates the inability to flex the ring finger DIP What is the most likely diagnosis |
"rugby jersey finger", which is an avulsion of the flexor digitorum profundus (FDP) tendon. |
|
|
A butcher sustains a traumatic amputation of the ring finger through the distal interphalangeal joint. He is brought to the operating room where the flexor digitorum tendon is retrieved and advanced to the distal stump. Three months after surgery the patient notes that when he makes a fist, only his ring finger tip reaches the palm. What is this patient's clinical problem? |
Quadrigia syndrome occurs when a flexor digitorum profundus (FDP) tendon is shortened and advanced. |
|
|
A 34-year-old seamstress was diagnosed with Parsonage-Turner brachial neuritis in the right upper extremity 1 month ago. She has weak forearm pronation with the elbow in the flexed position. She denies any current sensory changes. A clinical image of her hands attempting to make a clenched fist Which of the following most likely represents her diagnosis and treatment |
This patient presents with anterior interosseous nerve (AIN) syndrome and is often seen in conjunction with brachial neuritis (Parsonage-Turner Syndrome). -Anterior interosseous nerve syndrome treated with observation |
|
|
sx: aching pain over proximal volar forearm sensory disturbances over the distribution of palmar cutaneous branch of the median nerve (palm of hand) which arises 4 to 5 cm proximal to carpal tunnellack of night symptoms xray=supracondylar process dx? define? |
Pronator Syndrome -A compressive neuropathy of the median nerve at the level of the elbow |
|
|
Cubital tunnel syndrome is caused by compression of the ulnar nerve between what two structures as it passes posterior to the medial epicondyle? |
- Osborne's ligament and the MCL ulnar nerve passes posterior to the medial epicondyle and medial to the olecranon, then enters the cubital tunnel. The roof of the cubital tunnel is primarily made up of Osborne's ligament, and the floor consists of the medial collateral ligament. |
|
|
is not a possible sites of compression for the ulnar nerve? |
ligament of Struthers |
|
|
A 50-year-old man complains of numbness and tingling along his right small finger. Physical exam is notable for the finding demonstrated compensatory IP hyperflexion of FPL (innervation?) to compensate for the loss of adductor pollicis (innervation?) during key pinch. Elbow flexion reproduces the numbness and tingling. Physical therapy and splinting have failed to relieve the symptoms. Which of the following is the most appropriate surgical intervention to alleviate the symptoms while minimizing complications? |
- FPL (AIN) - adductor pollicis (ulnar nerve) Simple ulnar nerve decompression at the cubital tunnel |
|
|
A 72-year-old female complains of progressive weakness with grasp and key pinch in her left hand. Physical exam of the hand is significant for decreased sensation on the volar aspect of the fourth and fifth digits. Dorsal sensation throughout the hand is normal. A clinical photo displaying bilateral key pinch FPL is used to substitute for the weakened adductor pollicis resulting in flexion of the thumb at the interphalangeal joint, and MCP joint hyperextension.. What is the most likely cause of compression? |
Ganglion within Guyon's canal |