Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
91 Cards in this Set
- Front
- Back

|
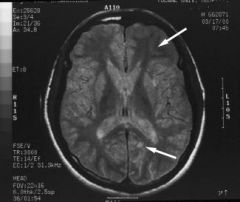
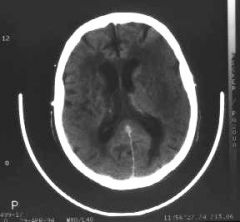
Diagnosis: Glioblastoma multiforme
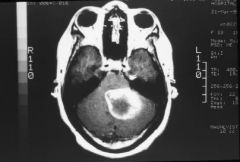
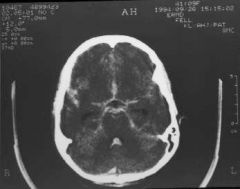
A contrast CT scan reveals a bizarrely and peripherally enhancing mass within the right cerebellar hemisphere with central low density consistent with either necrosis or cystic degeneration. The findings are consistent with either a metastatic lesion or a primary neoplasm such as a glioblastoma multiforme. The other consideration would be an abscess which usually has a more uniform wall. |
|
|
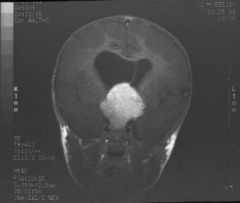
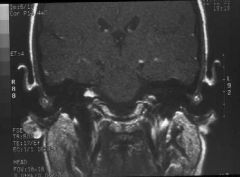
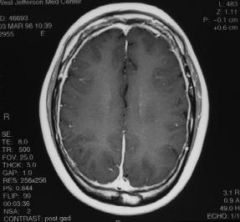
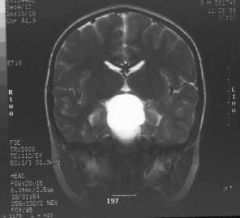
Hypothalamic Astrocytoma - Coronal T1 weighted MRI following the administration of contrast reveals a large hypothalamic mass which is somewhat lobulated but well-defined. The findings are typical for hypothalamic glioma in a child. The differential diagnosis would include other suprasellar lesions such as a solid craniopharyngioma.
|
|

|
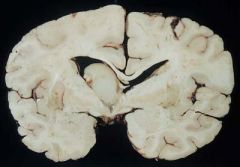
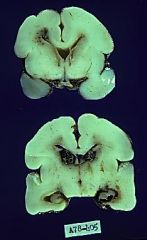
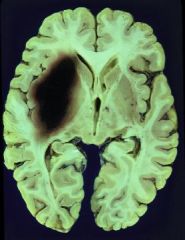
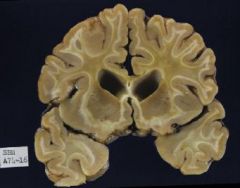
Glioblastoma multiforme - Left hemisphere basal ganglia and medial temporal variegated mass with indefinite borders, edema and shift of midline to the Right
|
|
|
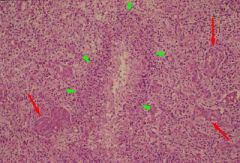
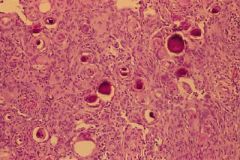
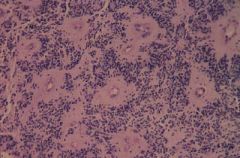
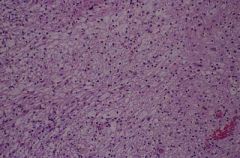
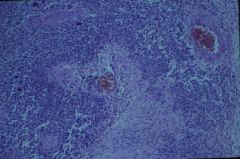
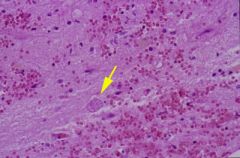
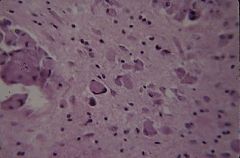
Cellular glial neoplasm with vascular endothelial proliferation (VEP)(red arrows), pseudopalisaded necroses (green arrow heads), cellular pleomorphism and mitoses; typical histologic features seen in high grade gliomas. The presence of necrosis qualifies this lesion as a glioblastoma multiforme.
|
|
|
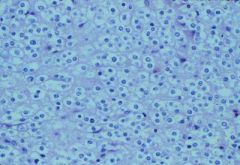
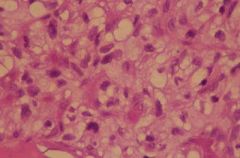
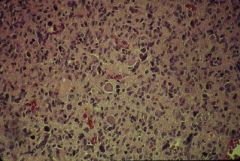
Oligodendroglioma - Glial neoplasm with round cells showing prominent perinuclear clearing, typically seen in oligodendrogliomas.
|
|
|
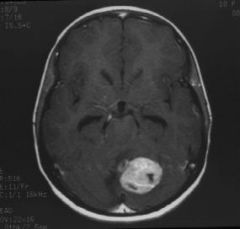
Medulloblastoma - Axial T1 weighted MRI with contrast reveals an enhancing cerebellar mass in the midline and slightly to the left of midline. A mass arising in this location would be consistent with a medulloblastoma versus a solid astrocytoma. Note the mild enlargement of the temporal horns of the lateral ventricle consistent with early hydrocephalus secondary to 4th ventricular compression by the mass.
|
|
|
Medulloblastoma - Cellular blue cell tumor with rosettes, may show neuronal and/or glial differentiation, may be desmoplastic
|
|
|
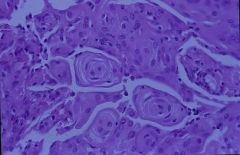
Tumor with cellular whorls and psammoma bodies (concentric calcifications), typically seen in meningiomas.
|
|
|
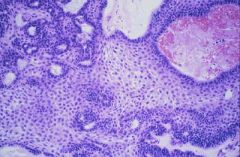
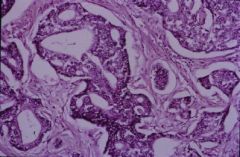
Craniopharyngioma - Epithelial lesion with peripheral palisading of basal squamous epithelium surrounding loosely arranged epithelial cells, the so-called "stellate reticulum" and nodules of keratin and variable calcification are typical histologic features of a craniopharyngioma.
|
|
|
Metastatic carcinoma - T1 weighted MRI with contrast shows a ring-enhancing left cerebellar mass with compression of the fourth ventricle. Central low signal intensity is consistent with either necrosis or cystic degeneration. The findings are typical for metastatic carcinoma versus primary neoplasm or abscess.
|
|

|
Ependymoma - Fleshy 4th ventricular mass arising from floor of the 4th ventricle and producing obstructive hydrocephalus. Diagnosis: Ependymoma
|
|
|
Ependymoma - Glial neoplasm with uniform cells and pronounced perivascular pseudorosettes are characteristic features of an ependymoma.
|
|
|
Colloid cyst - Cystic mass usually attached to 3rd ventricular roof and filled with jelly-like material; causes intermittent obstruction of foramen of Monro. Diagnosis: Colloid cyst.
|
|

|
Colloid cysts - Collapsed cyst wall lined by single layer of cuboidal-columnar mucin producing or ciliated cells, typically seen in colloid cysts.
|
|
|
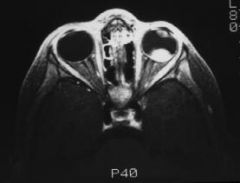
Retinoblastoma - MRI of the orbit with contrast reveal a well-defined mass in the posterior aspect of the globe adjacent to the retina. The appearance is typical of ocular retinoblastoma in a child.
|
|
|
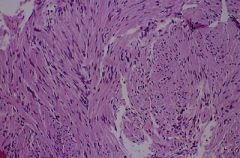
Schwannoma (Antoni A) - Neoplasm with fascicles of spindle cells with elongated wavy nuclei which are typically seen in Antoni A areas of a schwannoma.
|
|
|
Schwannoma (Antoni B) - Neoplasm with loose, disorderly cells as typically seen in Antoni B areas of a schwannoma.
|
|
|
Acoustic Schwannoma (Acoustic neuroma) - Axial and coronal T1 weighted MRI's demonstrate a slightly expansile enhancing mass within the right internal auditory canal consistent with an acoustic schwannoma (arrow). Note the normal MRI appearance of the contralateral left internal auditory canal.
|
|
|
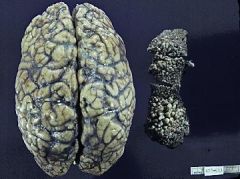
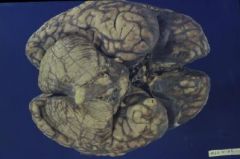
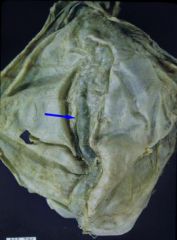
Angiofibromas (Tuberous sclerosis) - This is view of the brain from above and also a fragment of tissue removed from the face of the patient representing skin and angiofibromas. The skin shows multiple nodular structures. Brain shows irregular gyral pattern with some very firm and thick gyri, tubers. Diagnosis: #1 skin with angiofibromas (Adenoma sebaceum) . #2 Convexity of the brain with tubers.
|
|

|
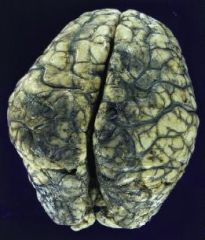
Tuberous sclerosis - Lateral view of the brain. It shows several large, thick and pale gyri in the frontal, parietal and temporal areas (Tubers). The gyri are irregular, thick, and have indentations. Diagnosis: Tuberous sclerosis
|
|

|
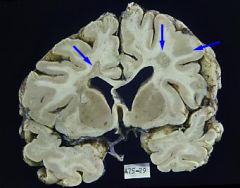
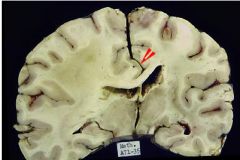
Tuberous sclerosis - Coronal sections of the cerebral hemispheres. One is through the head of caudate nuclei and tips of the temporal lobes. The second one is through the optic chiasm and the anterior portion of the third ventricle. The lower panel shows sections of the brainstem and mid-cerebellar peduncles and the medulla. The coronal sections show an irregular gyral pattern (white arrows) and the contrast with the normal cerebral cortex. On the side of the thickened gyri, the cortex and the white matter are not very well differentiated. The left lateral ventricle shows a nodule protuding from the head of the caudate nucleus (yellow arrow head). The section through the optic chiasm shows a thickened gyrus representing a tuber. Also, both lateral ventricles show nodules that are attached to the caudate nucleus and thalamus and protruding into the lateral ventricles. Section of the cerebellum shows cerebellar folial atrophy. Diagnosis: Tuberous sclerosis with, #1 Cortical tubers (white arrows), #2Periventricular candle gutterings (yellow arrow head) and #3 cerebellar atrophy (Blue arrow).
|
|
|
Hemangioblastoma (seen in Von Hippel-Lindau Dz) H&E stained section showing capillary vessels interspersed by foamy, stromal cells. Diagnosis: Hemangioblastoma.
|
|
|
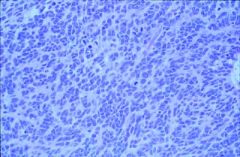
Glioblastoma mutiforme
|
|
|
Glioblastoma mutiforme
|
|
|
Meningioma - biopsy with Psammoma bodies
|
|
|
Metastatic adenocarcinoma
|
|
|
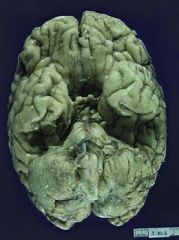
Basal view of a brain with abnormally opaque meninges. Diagnosis: Basal meningitis suggestive of Cryptococcal meningitis
|
|
|
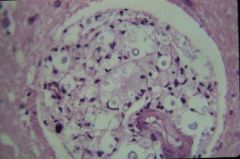
H&E stained microscopic section of brain showing macrophages clustered in the perivascular space, containing yeasts with a nonstaining capsule. Diagnosis: Cryptococcal meningitis
|
|
|
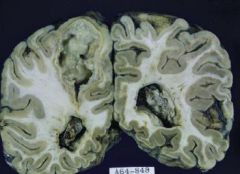
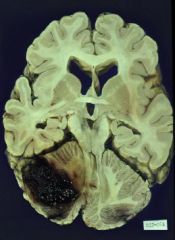
Coronal section through the occipital lobes. There is a big encapsulated lesion in the left hemisphere with a yellow well demarcated rim and green purulent material in the interior. There is also swelling of the left occipital lobe and presence of pus in the ventricles. Diagnosis: Abscess and pyocephalus
|
|

|
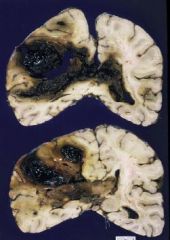
The left hemisphere is markedly enlarged and swollen. There is a big cavity containing pus. The lesion is well demarcated by a red-brown rim. The brain shows marked cyanosis due to tetralogy of Fallot. Diagnosis: Abscess associated with congenital heart disease.
|
|

|
Ventral surface of the brain with an opaque fibrinous exudate obscuring completely the basal structures. Diagnosis: Basal meningitis as seen in Tuberculosis
|
|
|
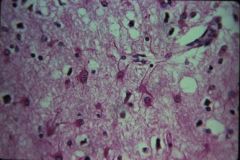
H&E stained microscopic section showing microvacuolation of the neuropil and reactive astrocytosis. Diagnosis: Spongiform encephalopathy of Creutzfeldt-Jakob disease
|
|

|
Axial CT scan without contrast reveals marked hypodensity representing edema within the frontal and temporal lobes with sparing of the basal ganglia and cerebellum. The findings are typical of herpes encephalitis versus an anoxic/or toxic insult. Diagnosis: herpes encephalitis.
|
|

|
Coronal section of the cerebral hemispheres through the caudate nuclei and corpus callosum. The cortical ribbon in of both insular areas shows petechiae.There are a few petechiae also in the orbital gyrus and gyrus rectus, bilaterally. Diagnosis: Herpes simplex virus encephalitis
|
|
|
post-contrast MRI's demonstrate non-specific abnormal meningeal enhancement. These findings are typical for menigitis. Diagnosis: meningitis.
|
|
|
H&E stained section showing a cyst (arrow). Diagnosis: Toxoplasma cyst.
-->Meningoencephalitis CT shows ring-enhancing lesions with surrounding edema. Positive Sabin-Feldman dye test. The causative agent is a protozoon The definitive hosts are cats Human infections are due to consumption of undercooked contaminated meat Transplacental infections can occur Symptomatic infection is associated with: AIDS, Immunosuppresive therapy, Malignant disease, Hodgkin’s lymphoma Congenital infection can produce: Encephalitis, Microcephaly, Chorioretinitis, Mental retardation |
|
|
Rabies
|
progressive malaise, headaches, fever , convulsions and hydrophobia.
eosinophilic cytoplasmic inclusions in pyramidal neurons of thr hippocampus peri-vascular lymphocytosis in the brain stem Negri bodies in Purkinje cells of the cerebellum |
|
|
Neurosyphilis
|
Tertiary syphilis --> Tabes dorsalis: axonal loss in dorsal columns (decreased vibratory sense, proprioception and touch)
obliterative endarteritis in leptomeninges cerebral gummas spirochetal invasion of cerebral cortex granular ependymitis Test with FTA-ABS (Treponema antibody test); but may be negative in 3* syphilis |
|

|
Parkinson’s disease - depigmentation of the substantia nigra in the midbrain (upper) and of the locus ceruleus in the pons (lower).
|
|

|
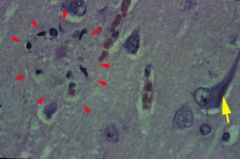
Lewy body of Parkinson’s disease - round eosinophilic inclusion surrounded by a halo and displacing the nucleus of the affected pigmented neuron.
|
|

|
Huntington’s Disease - There is global atrophy. The ventricles are dilated and the caudate nuclei appear flattened because of severe atrophy.
|
|

|
AML (Amyotrophic Lateral Sclerosis) - Picture of the anterior aspect of the spinal cord. The anterior spinal nerve roots appear thin and gray (atrophic) (blue arrows) as compared to the posterior roots with preserved normal thickness. This lesion can be seen in amyotrophic lateral sclerosis and spinal muscular atrophy (motor neuron diseases)
|
|

|
Midsagittal section showing wrinkled meninges and widened sulci due to diffuse atrophy. Diagnosis: Global atrophy as seen in Alzheimer’s disease
|
|
|
Alzheimer's Disease - neuritic plaques (red arrowheads) and neurofibrillary tangle (yellow arrow)
|
|

|
Global atrophy seen in Alzheimer's Disease - convexities of the brain showing diffuse marked cortical atrophy.
|
|

|
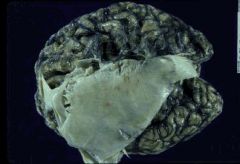
Pick's Disease - temporal lobe atrophy. Note the sulci of temporal lobe are deeper and gyri are smaller. Pick's disease may also involve the frontal lobe.
|
|
|
Multiple Sclerosis - The brain shows cortical atrophy with enlarged sulci. The white matter shows areas of gray, irregular discoloration (arrows). One is located on the left side of the slide in the periventricular area and another is located in the centrum semiovale in the right hemisphere.This gray discoloration of the white matter represents irregular demyelinating plaques.
|
|
|
Multiple Sclerosis - patchy areas of demyelination (arrows).
|
|
|
Periventricular hemorrhage in immature brain with intraventricular extension - Coronal sections of a newborn immature brain. Sections are made through the head of the caudate nucleus and midsection of the thalamus. The immature brain shows poor differentiation of the cortex and white matter and poor or early formation of sulci. The brain shows two focal areas of hemorrhage: in the periventricular area in the germinal matrix. The hemorrhage is larger on the left than on the right side and most likely ruptured on both sides into the ventricles.
|
|
|
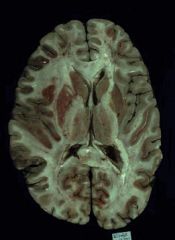
Recent cerebral infarction in left MCA distribution - This is an axial section of the brain through the mid portion of the cerebral hemispheres. The brain had been cut without complete fixation. However the left cerebral hemisphere shows swelling with compression of the lateral ventricle mainly in the frontal area. This swelling of the left hemisphere is due to recent necrosis in the Middle Cerebral Artery distribution. The brain in the MCA area shows discoloration of the cortex and also blurring between the cortex and white matter.
|
|

|
Recent infract of ACA - Coronal section shows the cerebral hemispheres through the anterior portion of third ventricle, anterior commissure, and the tip of the temporal lobes. This section is not quite symmetrical because it shows more of the anterior portion on the left side. The brain shows a recent area of necrosis in the right anterior cerebral artery distribution near the midline, with fragmentation of the tissue and poorly demarcated cortex and white matter. Corpus callosum is very thin and there is also an old slit-like lesion in the distribution of the left anterior cerebral artery. Diagnosis: Recent infarction in right anterior cerebral artery distribution, and old infarct, left anterior cerebral artery.
|
|

|
Old infarct of PCA - This is a view of the cerebral hemispheres after brainstem and cerebellum have been removed at the level of the midbrain. There is circular marked atherosclerosis of the left posterior cerebral artery. The left occipital lobe (right side of the photograph) shows a collapsed cystic and pigmented area in the distribution of the posterior cerebral artery
|
|

|
Transverse section of the cerebellum and medulla. The section shows blood vessels with atherosclerotic plaques. The left vertebral artery (seen on the right side of the photograph, green arrow) shows an occlusion in the region of posterior inferior cerebellar artery (PICA). The medulla shows a necrotic area in the lateral and posterior portion (behind the pyramids, yellow arrow). The ipsilateral cerebellar hemisphere in the lower and posterior portion shows necrosis and fragmentation of the tissue, red arrow . Diagnosis: #1 Occlusion of the left vertebral artery at the origin of PICA. #2Left posterolateral medullary infarct. #3 Infarction of the inferior posterior portion of the left cerebellar hemisphere.
|
|
|
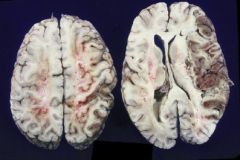
Hemorrhagic infarct of MCA - This is an axial view. The superior section is shown on the left side of the photograph and the inferior portion on the right side. The inferior portion is through the upper portion of the caudate nuclei and the thalami. The brain shows fragmentation, necrosis, and discoloration, predominantly of the cortex, in the right middle cerebral artery distribution. There is mass effect with compression of the ventricular system. Discoloration of the cortex within the lesion represents early hemorhagic transformation of the ischemic lesion
|
|

|
Old cystic infarct of MCA - Coronal sections of cerebral hemispheres . One is anterior and through the optic chiasm and the posterior section is through the thalami. The left hemisphere (on the left side of the photograph) is smaller than the right hemisphere. The small size of the left hemisphere is due to a large cystic lesion that includes the external portion of the putamen, internal capsule, inferior portion of the frontal lobe and parts of the temporal lobe.
|
|
|
Acute MCA territory infarct - Axial non-contrasted CT scan shows wedged-shaped low density in the left middle cerebral artery (MCA) territory representing acute edema. Note that the cerebral sulci are effaced compared to the right. The findings are pathognomonic of an acute MCA territory infarct
|
|
|
Acute subarachnoid hemorrhage (ACA aneurysm) - Ventral surface of a brain showing the frontal lobes, temporal lobes, brainstem and cerebellum. There is subarachnoid hemorrhage prominent in both Sylvian fissures and also around the chiasmatic area and interhemispheric fissure. There is also diffuse brain swelling which affects both cerebral hemispheres and cerebellum. The focal nature of the hemorrhage suggest a source in the anterior portion of the Circle of Willis, most likely anterior communicating cerebral artery aneurysm.
|
|

|
Ruptured ACA aneurysm - Coronal sections of the cerebral hemispheres through the frontal lobes and at the level of the genu of the corpus callosum. A hematoma has destroyed the area around the corpus callosum and inferior frontal gyri. Hematoma has ruptured into both lateral ventricles. The location of the hematoma is characteristic of a ruptured anterior communicating or anterior cerebral artery aneurysm.
|
|

|
Ruptured aneurysm of MCA - This is a close up of the ventral surface of the brain at the Sylvian fissure. Tip of the right temporal lobe has been amputated to show the blood vessels in the Sylvian fissure. The right carotid artery, posterior communicating and anterior cerebral artery are normal. The right middle cerebral artery at the distal bifurcation shows a ruptured sacular aneurysm, yellow arrow.
|
|
|
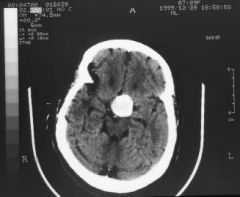
Axial CT scan without contrast demonstrates a large calcified suprasellar mass. Diagnosis: suprasellar aneurysm.
|
|
|
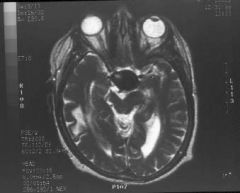
An axial T2 weighted MRI shows a large hypointense suprasellar mass with signal characteristics consistent with a large vascular structure. Diagnosis: suprasellar aneurysm.
|
|

|
The MR angiogram confirms a suprasellar aneurysm that appears to be originating from the anterior communicating artery. Diagnosis: suprasellar aneurysm.
|
|
|
Subarachnoid hemorrhage - Axial CT scans at the level of the perimescencephalic and the suprasellar cisterns reveal subarachnoid hemorrhage within the CSF cisterns, seen as high density. These are typical findings of subarachnoid hemorrhage where blood is seen as hyperdensity, whereas normal CSF is usually low density.
|
|
|
Spontaneous hypertensive aneurysm of Putamen - Axial section of the brain through the level of the putamen and the upper portion of the thalami. The left hemisphere shows a localized hematoma that involves the putamen and part of the anterior limb of the internal capsule. The hematoma has not ruptured into the ventricle and has spared the insular cortex.
|
|

|
Spontaneous hypertensive thalamic hemorrhage with intraventricular extension - Coronal section of the cerebral hemispheres through the pulvinar and quadrigeminal plate. The section shows a hematoma that has destroyed part of the thalamus on the left side. The hematoma has ruptured into the lateral ventricle and has compressed the quadrigeminal plate on the left side.
|
|

|
Spontaneous hypertensive pontine hemorrhage - This is a transverse section of the pons and cerebellum. The pons is almost completely destroyed by a hematoma that has replaced the tegmentum and most of the basis pontis . The hematoma has ruptured into the fourth ventricle which is obscured by this lesion. The cerebellum is normal
|
|
|
Spontaneous hypertensive right cerebellar hemisphere hemorrhage. #2 Acute hydrocephalus - This is an axial section of the brain, brainstem and cerebellum. The section goes through the caudate nuclei, part of the anterior commissure, the midbrain and the upper portion of the fourth ventricle and cerebellar hemispheres. The brain shows hydrocephalus with dilatation of both anterior portions of the lateral ventricles and the temporal horns. The right cerebellar hemisphere is enlarged by a hematoma that has originated near the dentate nucleus and has destroyed part of the white matter of the cerebellar hemisphere and the folia.The fourth ventricle is compressed to the left side anteriorly.
|
|

|
Old hypertensive spontaneous hemorrhage left putamen - An axial section of the cerebral hemispheres. Shows a pigmented slit- like lesion in the left putamen. This pigmentation is rusty brown and within the cavity there is some old blood. The sulci in the insula are prominent.
|
|
|
Multiple Hematomas - Coronal section of the cerebral hemispheres through the parietal area and splenium of the corpus callosum.The section shows enlargement of the left cerebral hemisphere. The enlargement is due to multiple hematomas The hematomas are irregular where they had ruptured into the ventricle. There is subfalcine herniation and there is dilatation of the left ventricle.
|
|

|
Amyloid angiopathy (congophilic angiopathy) - Microscopic section of the brain cortex, section has been stained with Congo Red for amyloid viewed with polarized light. The section shows relatively preserved cortical neurons and the blood vessels shows birefringence with polarized light. In some areas the walls of the blood vessels are yellow-green (arrow).
|
|
|
Superior sagittal sinus thrombosis - Dura mater seen from the external surface and including the superior sagittal sinus. The sinus is dilated and has a sausage like appearance due to thrombosis.
|
|
|
This is a brain viewed from above, showing both convexities of the hemispheres. There is dilatation and thrombosis of the cortical veins, more striking in the parasagittal areas. There is also hemorrhagic necrosis of the parasagittal gyri (outlined by arrows). Diagnosis: Cortical venous thrombosis with hemorrhagic infarction of the parasagittal brain tissue.
|
|

|
Vascular malformation (probably AVM) - Coronal section of the cerebral hemispheres through the midthalamus, subthalamic nucleus and midbrain. The right cerebral hemisphere shows abnormally dilated blood vessels; some of them seem to be arteries, some of them are dilated veins. These abnormal, dilated vessels occupy most of the medial portion of the right hemisphere and the tissue around this area is atrophic and pigmented.
|
|
|
Subdural hemorrhage
|
|

|
Chronic right subdural hematoma - There is semi-lunar left subdural hematoma with flattening of the subjacent left convexity. Note: there is no swelling or midline shift.
|
|

|
The slide shows the calvarium removed from above and showing bilateral epidural hematomas. The hematomas are outside the dura which has been left on the surface of the brain. Diagnosis: Bilateral epidural hematoma
|
|

|
This slide shows a sagittal section of the brain and spinal cord. The brain shows multiple deformities of the brainstem and cerebellum including #1tonsillar herniation, #2 elongation of the 4th ventricle, #3 beaking of the quadrigeminal plate and #4 elongation of the pons and medulla.There is an indentation of the brainstem and the cerebellum in the location of the foramen magnum . The lower portion of the spinal cord is attached to the sacral bone and shows also a piece of skin attached to a sac that contains meninges and roots of the lumbosacral cord. Diagnosis #1-3: Chiari malformation. #4 Sacral meningomyelocele.
|
|

|
Lumbar meningomyelocele - A sagittal view of a meningomyelocele that shows section of sacral vertebral bodies and spinal contents that include meninges, meningocele, herniated spinal nerve roots and part of the spinal cord.
Ante-natal diagnosis may be made with elevated maternal alpha-fetoprotein levels. frequently associated with the Chiari 2 malformation |
|

|
Chiari malformation Type 2 - This is a sagittal section of the brainstem and cerebellum. The slide shows herniation of the cerebellar tonsils, elongation of the pons and medulla and buckling of the lower part of the medulla. There is also elongation of the fourth ventricle.
|
|

|
Slide shows immature baby brain in axial section. It shows an immature brain with early differentiation of the cortex and the white matter. The brain shows also severe hydrocephalus and staining of the ventricular system and the ventricular walls with hemosiderin. There is an area of destruction of the germinal matrix, mainly in the right hemisphere and evidence of subarachnoid hemorrhage. Diagnosis: Old peri and intraventricular hemorrhage in an immature brain with #1 hemocephalus #2 hydrocephalus.
|
|

|
holoprosencephaly - This is a front view of a baby’s brain showing the brainstem, cerebellum and cerebrum. Abnormalities include #1 size of the cerebrum and the posterior fossa structures (including brainstem and cerebellum) are equal. #2 There is absence of the sagittal fissure. #3 There is absence of the rhinencephalic structures including absence of both olfactory nerves. #4 Absence of sulci in the brain with the primitive gyral formation.
|
|

|
Cerebellar tonsillar herniation - Shows brainstem and cerebellum from below showing very clearly both cerebellar hemispheres. There is indentation around the cerebellar tonsils this represents cerebellar tonsillar herniation. There is subarachnoid hemorrhage in this area and around the brainstem.
|
|
|
This is a coronal section of the brain through the midportion of the thalamus.The brain shows diffuse cerebral swelling and effacement of the sulci. There is also right displacement of the cingulate gyrus of the left hemisphere. This displacement represents subfalcine herniation.
|
|

|
Bilateral uncal herniation - This slide represents a view of the ventral part of both cerebral hemispheres. The brain stem has been removed at the mid brain level. The occipital lobes shows the dura representing the tentorium of the cerebellum. There is bilateral herniation of the hippocampal gyri (arrows). The right hippocampus (seen on the left side of the photograph) shows the larger herniation.
|
|

|
This is a transverse section of the brainstem and cerebellum at the level of the upper pons. Section shows area of hemorrhage in the posterior tectal portion of the pons. The hemorrhage is irregular and is in continuity with the upper portion of the fourth ventricle and the lower portion of the aqueduct. The area of hemorrhage is also in the midline of the pons. Cerebellar folia are swollen and the sulci are effaced by swelling. Diagnosis: Secondary pontine (herniation) hemorrhage (Duret hemorrhage).
|
|
|
Leukodystrophy (Krabbe's Disease) - Coronal section of the cerebral hemispheres through the caudate nuclei and tips of the temporal lobes. The photograph shows dilated lateral ventricles and diffuse demyelination involving almost all the white matter, more strikingly around the ventricles, but sparing the subcortical U fibers.
|
|
|
Leukodystrophy (Krabbe's Disease) - H&E stained microscopic section showing numerous "globoid cells" as seen in Krabbe’s disease
|
|

|
Lissencephaly - smooth surfaced brain with total absence of gyri. (Agyria).
|
|

|
Polymicrogyria - gyri are small, numerous and irregularly formed.
|
|

|
Agenesis of Corpus Callosum:
May be found in patients with mental retardation or in patients who are clinically normal. Radiologic imaging studies reveal a "bat-wing" deformity. A lipoma sometimes occupies the defect. May be associated with seizures |
|
|
Craniopharygioma - T2 weighted MRI reveals a suprasellar cystic lesion with peripheral enhancement.
|