Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
37 Cards in this Set
- Front
- Back
|
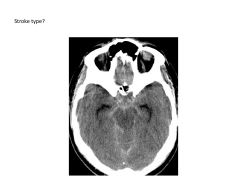
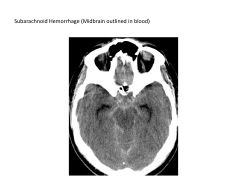
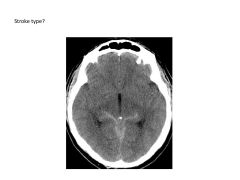
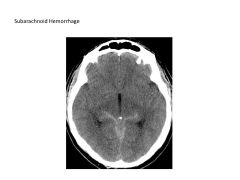
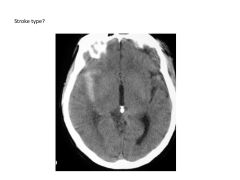
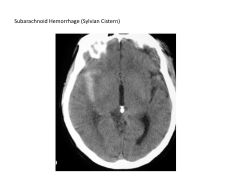
What is the main cause of subarachnoid hemorrhage?
Where do these bleeds occur? Complications? |
Subarachnoids caused by aneurysm 95% of the time (can be due to trauma as well)
Bleeds occur in cisterns (basal), sulci, within ventricles Complications: Hydrocephalus, vasospasm (secondary ischemia) |
|
|
What is a saccular aneurysm? Where do they tend to occur?
|
Saccular aneurysm: arterial outpouching at vessel bifurcation in Circle of Willia (90% Anterior comm, Pcomm; MCA)
Risk rupture if >7mm |
|
|
Who should be screened for a saccular aneurysm?
|
Fam Hx of 2 immediate relatives of aneurysm, those with Autosomal Dominant Polycystic Kidney Disease
|
|
|
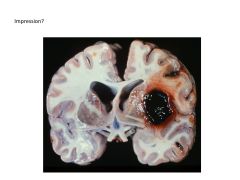
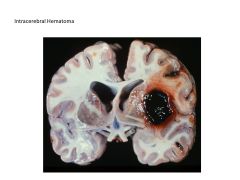
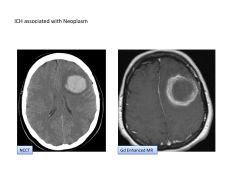
What are the most common causes of intracerebral hematoma?
|
Hypertension
Amyloid Angiopathy Less common: vasular malformation, neoplasm, venous infarct, toxin (cocaine), coagulopathy |
|
|
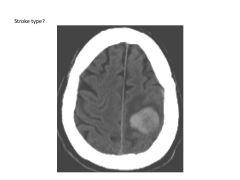
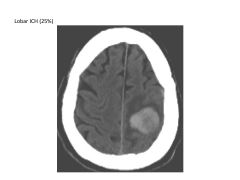
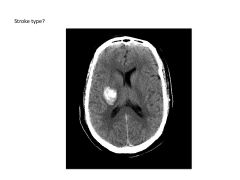
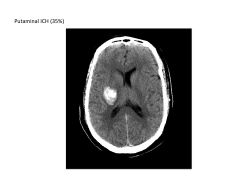
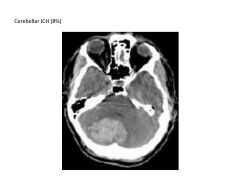
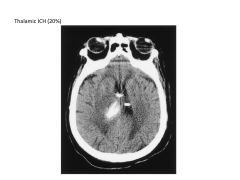
Where are hypertensive intracerebral hematomas most likely to occur?
|
Putamen (35%)
Lobe (25%) Thalamus (20%) Cerebellum (8%) Pons (7%) |
|
|
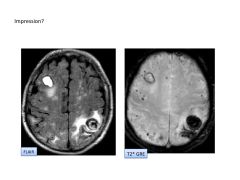
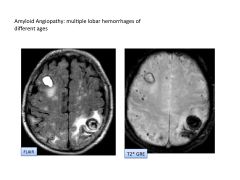
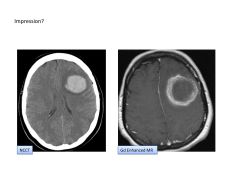
What is the most common cause of ICH? Appearance on imaging?
|
Amyloid Angiopathy
Appears as multiple lobar hemorrhages of different ages; microhemorrhages; small vessel ischemic WM dz |
|
|
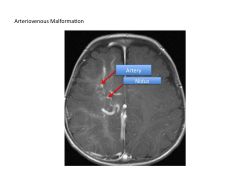
What is an arteriovenous malformation?
|
Tangle of abnormal vessels (nidus) that directly connects artery to vein; no normal capillary bed formed
Accounts for 45% ICH, 25% seizures |
|
|
What are the most common causes of an ischemic stroke?
|
(Thromboembolic)
Large Artery Atherosclerosis (25%) Cardiogenic Embolism (30%) Small Artery Occlusive Dz (20%) Intracranial Atherosclerosis (10%) Uncommon: Vasculopathy/vasculitis Dissection Venous Thrombosis Hypoperfusion |
|
|
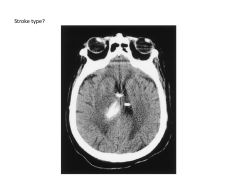
What are the three P's of CT stroke investigation?
|
check Parenchyma for hemorrhage/infarction (NCCT)
check Pipes for patency (lack of occlusions)--CT Arteriography Perfusion for tissue viability (look at tissue around stroke site that's ischemic but still viable--at risk tissue): CT Perfusion Imaging |
|
|
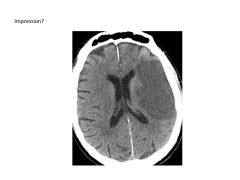
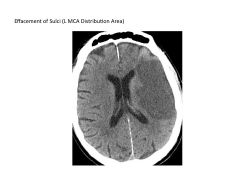
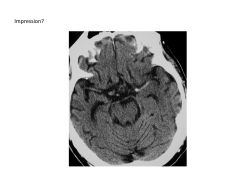
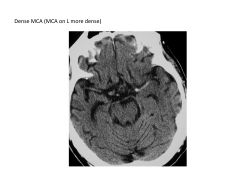
What are CT signs of early ischemic infarction?
|
Loss of grey-white differentiation
Swelling of Gyri-Sulci Effacement (cytotoxic edema) Dense MCA sign (MCA on one side more dense than on other side bc of thrombus) |
|
|
When is intravenous thrombolysis most effective?
|
Within 4.5 hours of stroke onset (IV TPA)
|
|
|
Infarct Core vs Ischemic Penumbra
|
Infarct Core: Irreversibly infarcted tissue at increased risk for hemorrhage with thrombolysis
Ischemic but VIABLE Penumbra: at risk for infarction if not re-perfused; salvageable with intra-arterial thrombolysis |
|
|
When is intra-arterial/mechanical thrombolysis warranted?
|
If there's a small infarct core and a large viable penumbra, benefit of IA-thrombolysis outweighs risk of hemorrhage
|
|
|
What are causes of cardioembolism?
|
Atrial fibrillation
Ventricular Thrombus Endocartitis Right to Left Shunt |
|
|
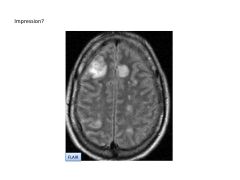
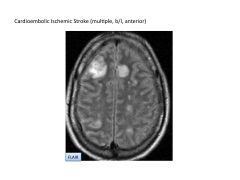
What are signs of a cardioembolic stroke on a CT?
|
Signs:
Multiple, bilateral infarct sites More likely to be cortical than WM In ANTERIOR circulation with/without hemorrhage |
|
|
When is intravenous thrombolysis most effective?
|
Within 4.5 hours of stroke onset (IV TPA)
|
|
|
Infarct Core vs Ischemic Penumbra
|
Infarct Core: Irreversibly infarcted tissue at increased risk for hemorrhage with thrombolysis
Ischemic but VIABLE Penumbra: at risk for infarction if not re-perfused; salvageable with intra-arterial thrombolysis |
|
|
When is intra-arterial/mechanical thrombolysis warranted?
|
If there's a small infarct core and a large viable penumbra, benefit of IA-thrombolysis outweighs risk of hemorrhage
|
|
|
What are causes of cardioembolism?
|
Atrial fibrillation
Ventricular Thrombus Endocartitis Right to Left Shunt |
|
|
What are signs of a cardioembolic stroke on a CT?
|
Signs:
Multiple, bilateral infarct sites More likely to be cortical than WM In ANTERIOR circulation with/without hemorrhage |
|
|
|
|
|
|
|
|
|
|

|

|
|
|
|
|
|
|
|
|
|
|

|
|
|

|

|
|
|
|
|
|
|
|
|
|
|
|

|
|
|
|
|
|
|
|
|
|
|
|
|