Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
31 Cards in this Set
- Front
- Back
|
Seizure vs Epilepsy
|
Seizure: clinical manifestation of abnormal and excessive excitation of a population of cortical neurons
Epilepsy: tendency toward recurrent spontaneous seizures unprovoked by systemic or neurologic insults |
|
|
What is epileptogenesis?
|
sequence of events that converts neuronal network into a hyperexcitable network
|
|
|
What is ictus?
Post-ictus? Inter-ictal? |
Ictus: period of a seizure
Post-ictus: period of abnormal behavior that follows ictus (confusion, paresis, lethargy) Inter-ictal: baseline phase in between seizures |
|
|
What is an aura?
|
Earliest experienced syx that predict an imminent larger seizure to follow (represents early ictal phase)
|
|
|
Focal vs Generalized Seizure
|
Focal: seizure arises from particular region of cortex at onset
Generalized: seizure arises diffusely (bilaterally synchronous) |
|
|
Primary Generalized vs Secondarily Generalized
|
Primary Gen: Starts out as Generalized
Secondarily Gen: Starts out focal and propagates |
|
|
Simple vs Complex Partial Seizures
|
Simple: Consciousness preserved (simple partial seizure)
Complex: Loss of Consciousness |
|
|
Describe an absence seizure.
|
Petit mal
Staring spell; non-convulsive seizure |
|
|
Describe a generalized tonic-clonic seizure.
|
grand mal seizure
Convulsive seizure: tonic (stiffening) phase followed by clonic (twitching) phase |
|
|
Describe a myoclonic seizure.
|
Convulsive seizure with brief twitches
|
|
|
Describe a tonic seizure.
|
Convulsive seizure with brief stiffening.
|
|
|
Describe an atonic seizure.
|
Convulsive seizure with sudden loss of tone (falls)
|
|
|
Symptomatic vs Idiopathic seizures
|
Symptomatic: seizure is secondary (symptomatic) of another problem (ex: head trauma)
Idiopathic: unknown cause, could be genetics |
|
|
What metabolic derangements can cause seizures?
What are other causes of seizure? |
Hypo/hyperglycemia
Hyponatremia Hypocalcemia Hypomagnesia Other causes: Toxins Withdrawal Fever CNS Trauma, infection, ischemia, hemorrhage Neurodegenerative Illnesses (AD) |
|
|
What is DFLE?
|
Autosomal Dominant Frontal Lobe Epilepsy
Genetic cause of epilepsy |
|
|
Effect of age on epilepsy's etiology?
|
First two decades: genetic, early life CNS insults (infection, vascular, CNS dysgenesis)
In the elderly: vascular (stroke), neoplasia, neurodegen, toxic-metabolite, drug/EtOH withdrawal |
|
|
Acute Symptomatic Seizures vs Delayed Seizure
|
Acute Symptomatic: post CNS insult, later epilepsy possible, but variable
Delayed Seizure: silent period of weeks, months, or years after injury |
|
|
What neuronal changes in epilepsy allow for hyperexcitability?
|
-excitatory axonal sprouting
-loss of inhibitory neurons -loss of excitatory neurons driving inhibitory neurons |
|
|
What does the kindling model of epileptogenesis state?
|
Repeated subconvulsive stimuli result in electrical afterdischarges which eventually:
lead to stimulation-induced clinical seizures lead to spontaneous seizures (epilepsy) (applicability to human epilepsy is uncertain) |
|
|
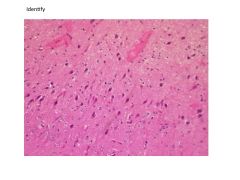
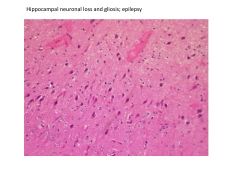
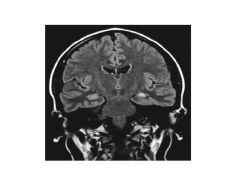
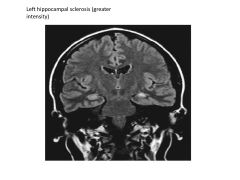
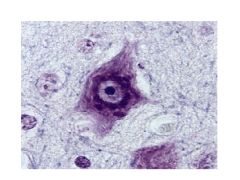
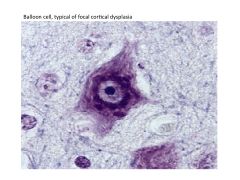
What are the pathological findings in epilepsy?
|
Hippocampal sclerosis (mesial temporal sclerosis)
Cortical dysplasia Gyral abnormalities (polymicrogyria) |
|
|
|
|
|
|
|
|
|
|
|
Distribution of epileptiform waves on EEG can help determine _________________
|
type of epilepsy (focal, generalized, lateralized)
|
|
|
What EEG abnormalities correlate with seizure?
|
Spikes, sharp waves, spike-wave complexes, polyspikes
|
|
|
Differential Diagnosis for Epilepsy
|
Syncope (esp convulsive--syncope = loss of consciousness)
Migraine Vertigo Non-epileptic seizures (Any transient spell associated with confusion) |
|
|
Spell vs Seizure
|
Spell: less specific of pathophysiologic mechanism; preferable if etiology (cause) is unknown
Seziure: disrupted cerebral physiology with hyperexcitable, hypersynchronous neuronal activity |
|
|
Seizure vs Syncope:
Setting Prodrome Ictus Confusion |
Seizure:
Setting: Random, non-situational Prodrome (premonitory syx): None or aura (GI, deja vu, sensorimotor) Ictus: Rigid fall, injuries, incontinence, clonus Confusion: Prominent, minutes to hours Syncope: Setting: Often situational (pain, emotion), upright Prodrome: nausea, pallor, clammy, visual graying Ictus: Flaccid fall, rare injury, brief & generalized jerking Confusion: Mild, fleeting, no paresis, "shaken up" |
|
|
What is status epilecticus?
|
Ongoing seizure activity lasting over 10-15 mins; recurrent seizures without interval recovery to neurologic baseline
|
|
|
Treatment of Status Epilecticus?
|
IV Benzos
1st Line AED: phenytoin 2nd Line AED: barbiturates Sedative agents to put pt in iatregenic coma |
|
|
If a third of patients with epilepsy are refractory to AEDs, what treatment options are available to them?
|
Surgery for well-localized cases to non-eloquent cortex (non-language area): lobectomy, lesion-ectomy
Palliative surgeries: callosotomy (CC: changes seizure to focal), hemispherectomy Vagal Nerve Stimulation Ketogenic diet (high fat, low carb, adequate protein) in kids |