![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
12 Cards in this Set
- Front
- Back
|
primary phys functions of respiratory system |
gas exchange
protective function: for pollutions (don't want that in blood that goes everywhere!)- defensive reflexes and filtering and conditioning
metabolic function |
|
|
spirometer: |
deal pt breathes into and it goes up and down with the metal ball to show volume |
|
|
normal breathing maximum inspiration and max expiration difference when exhale max |
tidal volume
vital capacity
expiratory reserve volume |
|
|
total lung capacity
residual volume
functional residual capacity |
volume in lung after a max inspiration
the lung volume when you've max exhaled: can't go down anymore
volume left after normal exhalation |
|
|
what factors affect lung volumes |
age declines height gender: females less
posture: standing vs supine (ERV decreases, IRV increases, TV no change, so FRC decreases while IC increases for healthy pt) effect exaggerated in obese pt
dz: restrictive and obstructive |
|
|
what are restrictive and obstructive dz like |
restrictive: sarcoidosis and other stuff. These lessen all the volumes, so both FRC and IC are lower than normal
obstructive like emphysema or asthma, see overall increased TLC with increased FRC from RV increase. ERV, TV, IRV thus IC and VC are all decreased |
|
|
in obstructive dz the residual volume is important but not easily measured with spirometry. what do they use? |
helium dilution method- it's inert and not soluble. Pt breathes in mouth piece and turn on He during end of normal exhalation (it's closed circuit now) and let He distribute to his lungs. The He concentration will reflect how much volume in the lung- it'll be diluted now.
initial [He] x volume machine = after [He] x (volume machine x FRC)
or they fancy with body plethysmograph |
|
|
what is plethysmograph
when the pt is instructed to exhale against closed shutter at mouthpiece, the pressure in his lung will _____ and the pressure in the box will ____. |
like a phone booth. uses Boyle's law. PV = constant (RT held constant)
increase, decrease the person's body volume goes down from lung, so increases pressure in lung, decreases pressure in box |
|
|
how do He and plethysmograph compare? |
in obstructive like COPD, it won't be measured with He. The obstructed regions are part of the FRC. So plethysmograph it will be detected because even though the area is obstructed, the whole lung is compressed since you're breathing against shutter. The volume in the obstructed regions still compresses just the same because compressibility.
so if He and plethysmograph give different FRC's, suspect certain dz and that they are considerable |
|
|
what's the first clue that pt has obstructive or restrictive lung dz |
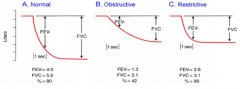
Obstructive: forced expiratory volume is decreased, going slowly into FVC
Restrictive: FEV immediately reaches FVC
FEV is within first second. FEV/FVC ratio should be 80% rather than 40 or 90. |
|
|
three major factors when doing FEV |
effort from muscles- they may be sad and defeated- make them try very hard
airway resistance- trying to tell if resistance from constriction or something- is it edema, constriction, gross cancer growth
elastic recoil of the lung- if lung is stiffer from fibrosis, when you let it go, there is more recoil to put out so the ratio will look higher since air shoots out but that pt doesn't breath well since too stiff to open up very far |
|
|
which volume/capacity measures change with age |
vital capacity goes down
residual volume and functional residual capacity increase. The total lung capacity stays the same. |