Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
95 Cards in this Set
- Front
- Back
|
Opacities on x-ray on both sides of carina
|
B/l hilar adenopathy-->Sarcoidosis
|
|
|
Dermatitis
Diarrhea Dementia |
B3 (niacin) deficiency-->Pellagra
|
|
|
Hyperphagia
Hypersexuality Hyperorality Hyperdocility |
Kluver-Bucy Syndrome (b/l amygdala lesion)
|
|
|
Nystagmus
Intention tremor Scanning speech |
Multiple Sclerosis
|
|
|
Lower extremity purpura
Arthralgias Renal Disease |
Henoch-Schönlein Purpura (vasculitis)
|
|
|
AMA Abs
|
Primary Biliary Cirrhosis
|
|
|
Anti-Platelet Abs
|
Idiopathic Thrombocytopenic Purpura
|
|
|
New born
Chronic diarrhea Failure to thrive Chronic candida |
SCID: Severe combined immunodeficiency
|
|
|
Child
Eczema Coarse facial features Cold abscesses |
Job Syndrome--Hyper-IgE
|
|
|
Child
Partial albinism Peripheral neuropathy Recurrent infections |
Chediak-Higashi Syndrome
|
|
|
Alpha-adrenergic antagonists used in treatment of pheochromocytoma
|
Phenoxybenzamine
Phentolamine |
|
|
Ipratropium:
Use |
COPD
Asthma |
|
|
Atropine:
Use |
Induce mydriasis; cause cycloplegia (paralysis of ciliary mm)
|
|
|
Tropicamide:
Use |
Induce mydriasis; cause cycloplegia (paralysis of ciliary mm)
|
|
|
Which bacteria are obligate intracellular?
Why? |
Rickettsia
Chlamydia Both lack ability to make ATP (Stay inside when it's Really Cold) |
|
|
Which bacteria form spores?
|
Bacillus
Clostridium Coxiella burnetti |
|
|
Case-control study
|
Compres group of people with dz to group without
Looks for prior exposure or risk factor Asks "What happened?"--retrospective |
|
|
Cohort study
|
Compres group with given exposure or risk factor to a group without
Looks to see if exposure increases likelihood of disease Asks "What will happen?" (Confirm risk factors, risk factor reduction)--prospective |
|
|
Cross-sectional study
|
Collects data from group of people to assess frequency of disease (and risk factors) at a particular point in time
"What is happening?" |
|
|
Twin concordance study
|
Compares frequency with which both monozygotic and dizygotic twins develop dz (measures heritability)
|
|
|
Adoption study
|
Compares siblings raised by biologic vs adoptive parents; measures heritability and influence of environmental factors
|
|
|
Meta-analysis
|
Pools data from several studies to come to an overall conclusion
Achieves greater statistical power and integrates results of similar studies. May be limited by quality of individual studies or bias in study selection |
|
|
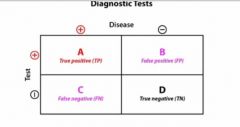
Draw disease x test table.
Label each box with relevant values. |
|
|
|
What is sensitivity?
General and equation |
TP/(Everyone w/Dz)
Probability that person with a dz will test positive for that disease Rules OUT dz 100% sensitivity means no false poz |
|
|
What is specificity?
General and equation |
TN/(People w/o dz)
Proportion of people without disease who test negative |
|
|
What is positive predictive value?
General and equation |
TP/(TP+FP)
Probability that person with positive test result actually actually has dz |
|
|
What is negative predictive value?
General and equation |
TN/(FN+TN)
Probability that person actually is disease free given a negative test result. |
|
|
Increased prevalence will increase _____.
|
PPV
|
|
|
Effect of prevalence on false negatives.
|
High prevalence-->inc'd false negatives
|
|
|
A test is positive for 800 of the 900 people who have disease X.
A test is negative for 1400 of 1600 people that do not have disease X. Determine: Sensitivity Specificity PPV NPV |
Sensitivity = TP/(Total w/Dz) = 800/900 = 0.89
Specificity = 1400/1600 = 0.88 PPV = TP/(TP+FP) = 800/(800+200) = 0.8 NPV = TN/(TN+FN) = 1400/(100+1400) = 0.93 |
|
|
What is prevalence?
|
(Total cases in population at a given time)/(Total population at a given time)
|
|
|
What is incidence?
|
(New cases in a population over a given time period)/(total population at risk during that time period)
Do not include people who had disease before given period! |
|
|
Prevalence = incidence for _______.
|
Acute diseases (common cold)
|
|
|
Relative risk:
Study type used for What is it? Equation |
Cohort study
Relative probability of getting disease in exposed group compared to unexposed group %Disease in exposed group/%Disease in unexposed group Don't forget percent!!! In decimal form, duh. |
|
|
Attributable risk:
What is it? Equation |
Difference in risk between exposed and unexposed group, or proportion of dz occurrences attributable to the exposure
%dz in exposure group - %dz in non-exposure group |
|
|
Odds ratio:
Study type used for What is it? Equation |
Used for case-control studies
Odds of having dz in exposed group divided by odds of having disease in unexposed group Approximates relative risk if prevalence is low ad/bc = (exposed with disease * unexposed without dz)/(exposed no dz * unexposed with dz) |
|
|
What is absolute risk reduction?
|
Reduction in risk assocd w/treatment as compared to placebo
Formula is same as attributable risk (except your exposure is something that should reduce risk of dz, e.g., abx): %dz in exposure group - %dz in non-exposure group |
|
|
What is number needed to treat?
|
1/absolute risk reduction=
1/(%dz in exposure group - %dz in non-exposure group) How many ppl you need to treat to save 1 life |
|
|
What is number needed to harm?
|
1/attributable risk=
1/(%dz in exposure group - %dz in non-exposure group) |
|
|
100 patients receive medication Z to prevent DM
200 patients did not receive medication Z 10 patients in experimental group developed DM 40 patients in control group developed DM Calculate absolute risk reduction and number needed to treat. |
Absolute risk reduction:
10/100 - 40/200 = -0.1-->reduce risk by 10% NNT = 1/-.1 = 10-->need to treat 10 pts to save 1 life |
|
|
A physician is looking for risk factors for a disease. He interviews 100 hospitalized patients with the disease and 100 hospitalized patients without the disease.
What type of study is this? |
Case-control study (retrospective)
|
|
|
A new glucose test arrives.
There is a standard substance provided that has 90 mg/dL of glucose. Your repeated measurements of substance reveals the following values: 54, 56, 55, 54, 53, 56, 55, and 54. What can you say about the precision and accuracy of your new glucose test? |
Precise (staying within a narrow range)
Not accurate (not close to 90) |
|
|
A group of people that smoke and a group that does not smoke are followed over 20 years. Every 2 years, it is determined who develops cancer and who does not.
What type of study is this? |
Prospective study, determining risk factors-->Cohort study
|
|
|
A certain screening test has a 1% false-negative rate.
What is the sensitivity of the test? |
Sensitivity = TP/(total w/dz)
False-negative rate = 1% False-negative = Poz Dz, Neg Test Take 100 people: 99 test positive 1 tests negative Sensitivity = 99/100 = .99 Note: sensitivity = 1-FN rate |
|
|
The prevalence of varicella in a population A is 2 times the prevalence of varicella in population B.
The incidence is the same in populations A and B. What can be assumed about disease duration in population A versus population B? |
Duration is 2x longer in populn A than it is in populn B.
|
|
|
What does it mean if the relative risk is <1?
|
Disease is less likely to occur in exposed group
|
|
|
What does it mean if the relative risk is >1?
|
Dz more likely to occur in exposed group
|
|
|
What does it mean if the relative risk is =1?
|
No different in risk of dz between exposure groups
|
|
|
Precision vs Accuracy
|
Precision = reproducibility of test result
Accuracy = validity (trueness of test measurements) |
|
|
What is a crossover study and how does it reduce bias?
|
Crossover study is when you start with two groups:
1 with placebo 1 with drug Then 6 months later placebo group gets drug, and drug group gets placebo Reduces bias bc each subject acts as own control |
|
|
Identify bias:
In a drug trial, only patients with end-stage disease are selected to receive drug. |
Selection bias
|
|
|
Identify bias:
Studies performed on patients that have been hospitalized. |
Berkson's bias--bias of syx, severity of dz, access to care, popularity of institution, etc.
|
|
|
Identify bias:
Ask parents of autism patients what happened 3 days before child developed autism. |
Recall bias
|
|
|
Identify bias:
A questionnaire of risk factors for MI is sent out to survivors of MI. |
Selection bias (what about those who did no survive MI?)
|
|
|
Identify bias:
Study performed in China may not be generalizable to US population. |
Sampling bias--subjects not generalizable to population
|
|
|
Identify bias:
Benefit of new drug during study may have been due to study requiring participants to attend clinic monthly and therefore receive better healthcare. |
Procedure bias--subjects in different groups not treated to same
|
|
|
Identify bias:
Asbestos miners may be more likely to have cancer because they mine asbestos because they're more likely to smoke. |
Confounding bias--related variables
|
|
|
Identify bias:
A test detects disease before it's detected by traditional diagnostics, but early detection does not increase survival. |
Lead-time bias
|
|
|
Identify bias:
An orthopedic surgeon performs a study on arthroscopic knee surgery. |
Pygmalion effect: researcher's belief in efficacy of tx changes outcome of tx
|
|
|
Identify bias:
In studying effects of MVI on longevitiy, study group not only takes daily MVI, but also consumers multiple other vitamins on daily basis. |
Hawthorn effect: group being studied changes its behavior owing to knowledge of being studied
|
|
|
What is positive skew?
|
Mean > median > mode (Asymmetry with tail on right)
Tail, not hump!! |
|
|
What is negative skew?
|
Mean<median<mode (asymmetry with tail on left)
Tail, not hump!! |
|
|
What is a null hypothesis?
|
Hypothesis of no difference (no association between dz and risk factor in populn)
H0 |
|
|
What is an alternative hypothesis?
|
Hypothesis that there is some difference (there is association between disease and risk factor in populn)
H1 |
|
|
Type I error (alpha)
|
Stating there is an effect/difference when none exists (mistakenly accept experimental hypothesis and reject null)
Remember p value = probability of making type I error |
|
|
Type II error (beta)
|
Stating there is NOT an effect or difference when one exists (fail to reject null hypothesis when in fact H0 is false).
Note: beta = probability of making a type II error |
|
|
What is a p value?
|
Probability of making a type I (alpha) error
If p<0.05, less than 5% chance that have rejected H0 when H0 is true. |
|
|
What is power?
How is it calculated? How can it be increased? |
Power = 1-beta
Power is probability of rejecting null hypothesis when it is in fact false, or likelihood of finding a difference if one exists. Depends on total number of end points experienced by populn Difference in compliance between groups Size of expected effect Inc sample size-->inc power |
|
|
How much of a population do the following SDs contain:
±1SD ±2SD ±3SD |
±1SD: 68%
±2SD: 95% ±3SD: 99.7% |
|
|
±____SD contains 90% of population.
|
±1.645 SD
|
|
|
What is a confidence interval?
How is it determined for: 90% CI 95% CI |
Range of values in which you'd expect if repeated the study
CI = range from [mean-Z(SEM)] to [mean +Z(SEM)] Note: for 95% CI (correlates to p=0.05), Z = 1.96 (can use 2) for 90% CI, Z = 1.645 SEM = SD/(sqrt of N) |
|
|
If mean heart rate for a sample is 74 bmp and SEM is 2, you can be 95% certain that the true mean lies within ________.
|
CI = range from [mean-Z(SEM)] to [mean +Z(SEM)]
=74 +/- (1.96 x 2) |
|
|
Using confidence intervals, when can H0 be accepted?
|
If CI range of means contains 0.
|
|
|
Using relative risk or _______, when can H0 be accepted?
|
If RR or Odds Ratio = 1, H0 cannot be rejected.
|
|
|
In a study of USMLE scores at a particular school, the mean is 230 and the SD is 20.
N=100 What is the 95% CI? |
CI = range from [mean-Z(SEM)] to [mean +Z(SEM)]
CI = 230 ± (230 - 2*20/√100) to (230 + 2*20/√100) 226-234 |
|
|
In a study of USMLE scores at a particular school, the mean is 230 and the SD is 20.
N=16 What is the 95% CI? |
CI = range from [mean-Z(SEM)] to [mean +Z(SEM)]
CI = 230 ± (230 - 2*20/√16) to (230 + 2*20/√16) 220-240 |
|
|
What does a t-test examine?
|
compares means of two groups
|
|
|
What does an ANOVA examine?
|
compares means of multiple groups
|
|
|
What does a chi-square examine?
|
looks at differences in percentages/proportions of groups, NOT MEANS
|
|
|
Correlation coefficient
|
between -1 and plus 1, closer to 1-->stronger correlation between variables
Closer to -1-->inverse relation |
|
|
Disease prevention:
Primary vs Secondary vs Tertiary |
Primary: prevent dz occurrence (HPV vaccine)
Secondary: early detection of dz (Pap smear) Tertiary: reduce disability from dz (chemotx) |
|
|
What diseases are reportable?
|
STDs: AIDS, gonorrhea, syphilis
Hep A, B, C Kid immunizations: Measles/Mumps/Rubella, Chickenpox Diarrhea: Salmonella, Shigella Tb |
|
|
Leading causes of death in:
Infants |
Congenital anomalies
Short Gestation Sudden infant death syndrome Respiratory distress syndrome |
|
|
Leading causes of death in:
Age 1-14 |
Injuries
Cancer Congenital anomalies |
|
|
Leading causes of death in:
Age 15-24 |
Injuries
Homicide Suicide |
|
|
Leading causes of death in:
Age 25-64 |
Cancer
Heart Dz Injuries |
|
|
Leading causes of death in:
Age 65+ |
Heart dz
Cancer Stroke COPD |
|
|
Premium vs Co-Pay
|
Premium = amt insured person pay insurance company (usually monthly)
Co-pay: amt insured person pays at time of service (e.g., $30 for clinic visit/drug, etc) |
|
|
HMO v PPO
|
HMO: health maintenance organization
PCP is gatekeeper to specialist In order for medical expenses to be covered, provider has to be in network PPO: preferred provider organization No gatekeeper to specialist Patient can see whomever they want; cost is higher for out of network care |
|
|
What is utilization management?
|
Someone that evaluates appropriateness, necessity, and efficiency of health care services
|
|
|
What is the resource-based relative value scale?
|
Scale that determines what a physician should be paid for a very specific procedure (CPT code) or service in a specific region of the country based on physician work, regional expense, and regional malpractice expenses
|
|
|
Medicare vs Medicaid
|
MedicarE for Elderly; >65 or <65 with certain disabilities and those with end stage renal dz
MedicaiD is for Destitute--federal and state health assistance for people with very low income |
|
|
Medicare:
Parts A vs B vs C vs D |
A: inpatient care in hospitals, hospice, home health care
B: outpt care, dosctors' services, PT/OT C: combination of A and B ("Medicare Advantage") D: stand-alone prescription drug coverage |
|
|
What is capitation?
|
Fixed payment for a period of time or number of patients.
Ex: ER shift Concierge practice (give me $3K and i'll take care of you and your children for a year) HMO |
|
|
When is pay for performance utilized?
|
Inc'd pay by health care organization for meeting preventive medicine targets (vaccines, colonoscopy, HgA1C)
|