![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
191 Cards in this Set
- Front
- Back
|
CNS
|
-Controls and regulates all mental and physical functions -Dysfunction of the neurons in an area of the brain can disrupt the complex organization of firing, resulting in abnormal perception of the environment, uncoordinated movement, loss of force production, and decrease in cognition |
|
|
Cellular Dysfunction |
Cell death is common in nervous system disorders • Necrosis – death of a tissue -Cellular swelling, fragmentation and cell disintegration • Apoptosis – programmed cell death - Do not cellular swelling - Necessary to prevent overproduction of one type of cell o Damage to the CNS can cause excessive apoptosis |
|
|
Cellular Dysfunction |
Glial cells - Nerve cells - Neurotransmission - Amino acids - Amines - Neuropeptides - Gaseous neurotransmitters and others |
|
|
Cellular Dysfunction |
|
|
|
Glial Cells |
Provide support and structure for the CNS similar to connective tissue in other areas of the body - Do not signal information - Macroglia and microglia – two primary cell types located throughout the CNS - Macroglia - Astrocytes - Oligodendrocytes - Schwann cells - Macroglia support and maintain neuroplasticity in the CNS - Often effected by disease processes that affect brain tissue |
|
|
Macroglia |
Astrocytes remove neuronal debris - Astrocytes are seen early in a CNS injury – astrocyte swelling - Oligodendrocytes and Schwann cells – produce the myelin sheath - Demylinated disorders (MS) are often due to disruption in the function of oligodendrocytes |
|
|
Glial Cells |
Microglia – immune cells of the brain - Respond to an insult in the CNS by proliferating and infiltration of the CNS tissue - Act like macrophages for the benefit of CNS tissue |
|
|
Nerve Cells |
Communicators for biochemical events, regulate structure and function Nucleus of the cell contains genetic material and directs manufacturing of proteins to determine structure, function and regulation of neural circuits When mutation or a change in the structure of the DNA occurs, abnormal proteins can be produced and increase chance of neurological disease Cell body inclusions – growths that occur within the cell body due to age or because of disease Result in loss of function of the cell |
|
|
Nerve Cell Communication - Neurotransmission |
Communication occurs in response to electrical, mechanical and chemical signals Nerve cells generate the following signals Input signal, trigger signal, conducting signal, and output signal Dendrite receives incoming signals from other neurons Action potential is fired through the axon Axon also serves as entry route for pathogens and toxins |
|
|
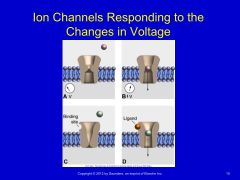
Ion Channels Responding to the Changes in Voltage |
|
|
|
Neurotransmission |
Synapse – release of neurotransmitter from the presynaptic terminal and up take of that substance in the postsynaptic receptor Changes in the neurotransmitter substances is often the cause for neurological disease processes Figure 18-6 |
|
|
Neurotransmitters and Associated Responses |
Amines Acetylcholine – active in the peripheral nervous system (PNS), released at neuromuscular junctions and ANS, regulates general activity Catecholamines – working memory, decrease with age and especially with Alzheimer’s Dopamine – decreased in patients with Parkinson’s and attention disorders of the frontal lobe Norepinephrine – also associated with attending |
|
|
Neurotransmitters and Associated Responses |
Amino acids GABA – synthesized by glutamate, provides brief inhibitory responses, found in basal ganglia Glutamate – involved in cell metabolism, found in afferent nerve endings, cerebellum, dentate gyrus, important in basal ganglia function • Excess glutamate seen in stroke, TBI and SCI • May also lead to degenerative processes in ALS, Alzheimer’s, and Parkinson’s Glycine – overlaps with GABA but is found primarily in the spinal cord |
|
|
Neurotransmitters and Associated Responses (continued) |
Neuroactive peptides Enkephalins and β-endorphins: pain control achieved by use of drugs (opiates) that bind to endorphin and enkephalin receptors Substance P: involved in pain pathways |
|
|
Clinical Manifestations |
Sensory disturbances Brainstem dysfunction Movement disorders Disorders of coordinated movement Deficits of higher brain function Altered states of consciousness Memory problems Autonomic nervous system Aging and the central nervous system |
|
|
Sensory Disturbances |
Includes damage to afferent nerves, dorsal columns of the spinal cord and brainstem Symptoms – loss of cutaneous sensation, numbness, tingling, paresthesias or dysthesia Loss of proprioception – position in space, postural control |
|
|
Brainstem Dysfunction |
Controls the lower motor neurons for the muscles of the head Initial processing of afferent information involving the head Cranial nerve entry Serves as a conduit for ascending sensory and descending motor tracts of the spinal cord 3 parts – medulla, pons (including the vestibular nuclei), and the midbrain Also houses the reticular formation which influences movement |
|
|
Movement Disorders |
Movement is coordinated by many parts of the brain Parietal and premotor areas of the cerebral cortex identify targets in space, determine course of action, and create the motor program The cortex determines strategies for movement Brainstem and spinal cord execute the task |
|
|
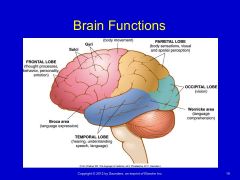
Brain Functions |
|
|
|
Disorders of Coordinated Movement |
Often involves the cerebellum Ataxia – lack of coordinated movement Usually seen in cerebellar dysfunction Hypotonicity – decreased muscle tone Usually seen in proximal muscle groups Asthenia – generalized weakness, can be seen in cerebellar lesions Dysmetria – over- or underestimation of movement toward a target, also seen in cerebellar lesions Intention tremor – over or undershooting during movement Dysdiadochokinesia – inability to perform rapidly alternating movements |
|
|
Disorders of Coordinated Movement |
Gaze-evoked nystagmus – nonvoluntary rhythmic oscillation of the eye Ocular dysmetria – similar to dysmetria of the extremities but involves the eyes’ ability to move from one target to another Gait disturbance Cerebellum has many other functions – motor learning, anticipatory/feedforward activity, cognitive and emotional processing |
|
|
Deficits of Higher Brain Function |
Cortex is responsible for language, abstract thinking, perception, movement, and adaptive response Frontal lobe – highest level of cognitive processing, control of emotion, behavior, personality Damage to frontal lobe – will see slow processing of incoming information, lack of judgement, withdrawal, irritability, lack of inhibition and apathy, lack of insight into deficits that are present Right hemisphere syndrome – inability to orient the body within external space (ie. Hemineglect |
|
|
Deficits of Higher Brain Function |
Dysarthria – disturbance in articulation (speech) Anarthria – inability to produce speech Aphasia – deficit of speech production or language output Apraxia – disorder of skilled purposeful movement and NOT a result of paresis, akinesia, ataxia, sensory loss, or comprehension Agnosia – inability to recognize an object |
|
|
Memory Problems |
Working memory – ability to hold information in short-term storage while permitting other cognitive operations to take place (depends of prefrontal cortex) Amnesia – loss of recent memory (common after TBI) Declarative memory – retention of facts and events of a prior experience or the memory of what has occurred |
|
|
Memory Problems |
|
|
|
Autonomic Nervous System |
Controls unstriated tissue, cardiac muscle, and glandular tissue Efferent autonomic pathways – divided into sympathetic and parasympathetic Also includes the enteric nervous system of in the walls of the gut Neurons in the cerebral cortex, basal forebrain, hypothalamus, midbrain, pons and medulla contribute to autonomic control Hypothalamus – integrates ANS and endocrine responses for homeostasis Medulla – control of cardiovascular, respiratory and gastrointestinal function |
|
|
Aging and the CNS |
Each of the following changes are seen with aging: Loss of cells, atrophy, decreased nerve conduction velocity, wear and tear similar to that seen in musculoskeletal tissues, decreased blood supply Mood-related and depressive symptoms Loss of sensory inputs for balance, mobility, vision and somatosensation |
|
|
Diagnosis
|
Clinical localization Computed tomography Magnetic resonance imaging Functional magnetic resonance imaging Positron emission tomography Electroencephalography Brainstem auditory evoked potentials Transcranial Doppler ultraso |
|
|
Types of Central Nervous System Neoplasms |
Primary tumors: Develop in the brain, spinal cord, or surrounding structures Secondary (metastatic) tumors: May spread to the CNS from another site, such as a lung Paraneoplastic syndromes: May occur as a result of remote or indirect effects on the CNS from cancer elsewhere in the body Leptomeningeal carcinomatosis: Metastasized carcinoma throughout CNS with multiple lesions to the meninges and CSF pathways of the brain and/or spinal cord |
|
|
Types of Central Nervous System Neoplasms (Continued) |
Malignant Astrocytomas Benign–slow growth rate and relatively non-invasive Meningiomas Neurinomas Hemagioblastomas -Because of space-occupying properties in vital tissue with a resultant high threat of functional limitation, the use of the term benign is somewhat misleading. Some authors insist that because of location, even a very slow growing CNS tumor should be considered basically malignant. |
|
|
Signs and Symptoms of Brain Tumors |
Headache Visual changes (double vision, blurred vision) Nausea Vomiting Cognitive changes — impairment of memory, judgment, personality Lethargy Behavioral changes Seizures Syncope Weakness Hemiparesis, hemiplegia Apraxia Cortical sensory deficits (graphesthesia, stereognosis difficulties) Sensory impairments (tingling, spatial orientation changes) Cranial nerve palsies Aphasia Facial numbness Hearing disturbances Anosmia Swallowing difficulties Paralysis of outward gaze (sixth cranial nerve) Papilledema Incoordination Ataxia In children, diastases of cranial sutures and enlarging head size |
|
|
EPILEPSY
|
Overview and definition Epilepsy is defined as a chronic disorder characterized by recurrent seizures. Although a diagnosis of epilepsy requires the presence of seizures, not all seizures imply epilepsy. Epilepsy comes from the Greek word meaning attack and has been recognized since ancient Babylonian times when people believed seizures were caused by demons. Incidence The overall prevalence of epilepsy is approximately 5 to 8 per 1000 individuals. Incidence is highest among young children and the elderly, with men slightly more affected than women (1.5:1). Epilepsy is the third most common serious neurologic disease of old age after dementia and stroke. |
|
|
EPILEPSY (Continued) |
Etiologic and risk factors • Epilepsy may result as abnormalities in the “wiring” of the brain or imbalance of neurotransmitters, or a combination of both. • Forms that are more heritable than others are termed idiopathic or primary epilepsies. Adult-onset seizure disorder • Epilepsy can be caused by virtually any major category of serious disease or human disorder. It can result from congenital malformations, infections, tumors, vascular disease, degenerative diseases, or injury. Infantile seizure • The age-dependent appearance of spontaneous seizures in the primary epilepsies appears to depend on critical periods in cerebral maturation. • The other important cause of seizures arising in the early neonatal period is hypoglycemia. |
|
|
EPILEPSY (Continued) |
Etiologic and risk factors • Epilepsy may result as abnormalities in the “wiring” of the brain or imbalance of neurotransmitters, or a combination of both. • Forms that are more heritable than others are termed idiopathic or primary epilepsies. Adult-onset seizure disorder • Epilepsy can be caused by virtually any major category of serious disease or human disorder. It can result from congenital malformations, infections, tumors, vascular disease, degenerative diseases, or injury. Infantile seizure • The age-dependent appearance of spontaneous seizures in the primary epilepsies appears to depend on critical periods in cerebral maturation. • The other important cause of seizures arising in the early neonatal period is hypoglycemia. |
|
|
EPILEPSY (Continued) |
Pathogenesis All seizure activity is a result of chaotic, excessive electrical discharge in the central nervous system (CNS). Susceptibility to these seizures most likely results from inherited biochemical, membrane, or neurotransmitter defects that result in abnormal excitability within the involved circuits. Events that may trigger a seizure: • Stress • Poor nutrition • Missed medication • Skipping meals • Flickering lights • Illness • Fever and allergies • Lack of sleep • Emotions such as anger, worry, or fear • Heat and humidity |
|
|
EPILEPSY (Continued) |
Clinical manifestations Signs and symptoms • In most individuals, seizures occur unpredictably at any time and without any relationship to posture or ongoing activities. Tonic-clonic seizures • In the tonic phase of a tonic-clonic seizure, the body becomes rigid and the person is at risk of falling • The clonic phase begins with rhythmic, jerky contractions especially in the extremities and ends with relaxation of all body muscles |
|
|
EPILEPSY (Continued) |
Prognosis Persons with epilepsy have increased mortality rates compared with the general population. Much of this increased risk occurs in individuals with symptomatic epilepsy in whom mortality relates to the underlying condition. Death from asphyxia is the greatest concern in instances when the individual has a seizure during eating or when the airway is compromised during the seizure or in the postepileptic phase. |
|
|
EPILEPSY (Continued) |
Classification of seizures Partial seizures • Simple partial seizures • Complex partial seizures • Partial seizure evolving to secondarily generalized seizures Generalized seizures • Absence seizures • Myoclonic seizures • Atonic seizures Tonic-clonic seizures Status epilepticus |
|
|
EPILEPSY (Continued) |
Common misconceptions about epilepsy Myth: You can swallow your tongue during a seizure. Fact: It’s physically impossible to swallow your tongue. Myth: You should restrain someone during a seizure. Fact: Do not use restraint; the seizure will run its course and stop. Myth: People with epilepsy should not be in jobs of responsibility and stress. Fact: People with epilepsy hold many types of jobs; they often do not inform others of the disorder. Myth: You can’t tell what a person may do during a seizure. Fact: The characteristic form of seizure is consistent during each episode. Behavior may be inappropriate for the time and place but will most likely not cause harm. Myth: You can’t die from epilepsy. Fact: Status epilepticus can cause death. It should be treated as a medical emergency |
|
|
PRIMARY HEADACHES |
Migraine • “A familial disorder characterized by recurrent attacks of headache widely variable in intensity, frequency and duration.” Migraine without aura Migraine with aura Typical aura without headache Sporadic and familial hemiplegic migraine Basilar-type migraine Vestibular migraine Ophthalmoplegic migraine Retinal migraine Status migrainosus Chronic migraine |
|
|
PRIMARY HEADACHES |
Cluster headaches • Rare, but are the most painful of the primary headaches Episodal cluster headache • Defined by periods of susceptibility to headache, called cluster periods, alternating with periods of remission • The most common type, constituting 80% of all cases Chronic cluster headache • A term used when the headaches have gone on for at least 12 months and remissions last less than 14 days • Evolves from episodal CH Other classifications • Paroxysmal hemicrania • Short-lasting unilateral neuralgiform headache attacks with conjunctival injection and tearing • Probable trigeminal autonomic cephalalgia |
|
|
SECONDARY HEADACHES |
Cervicogenic headaches Pain is localized to the neck and occipital regions and may project to the forehead, orbital region, temples, vertex, or ears Pain is precipitated or aggravated by special neck movements or sustained neck posture Posttraumatic headache syndromes Not a single pathology but a group of traumatically induced disorders with overlapping symptoms When the headache develops within 7 days of the trauma and resolves within 3 months, it is considered acute The headache can begin weeks or months after the trauma and can persist for years; this considered chronic |
|
|
SECONDARY HEADACHES |
Classifications of headache attributed to head or neck trauma Acute posttraumatic headache Chronic posttraumatic headache Acute headache attributed to whiplash injury Chronic headache attributed to whiplash injury Headache attributed to traumatic intracranial hematoma Headache attributed to other head and/or neck trauma Postcraniotomy headache |
|
|
SECONDARY HEADACHES |
Medication overuse headaches Frequent intake of medications used for headache can lead to chronic headache. It appears that all drugs used for the treatment of headache may lead to chronic headache. Migraineurs are most susceptible to headache related to excessive medication. Overuse of analgesic medications resulting in analgesic rebound phenomenon is common when the headache type has not been identified appropriately. |
|
|
SECONDARY HEADACHES |
Headaches in the elderly New-onset headaches in the elderly that are related to another disorder are more common than in the young. Such headaches can be caused by: • Increased use of nitrates for control of angina • Hypertension and atherosclerotic and hemorrhagic cerebrovascular disease • Diseases of the aged such as chronic obstructive lung disease • The hypercalcemia related to malignancy and chronic renal failure • Parkinson’s disease • Intracranial disease, tumors, and subdural hematomas • Cervical spondylosis and TMJ • Depression |
|
|
SECONDARY HEADACHE |
Temporal arteritis The headache of temporal arteritis classically is located over a branch of the superficial temporal artery and is described as a dull ache that persists throughout the day. Headache is the most common symptom in temporal arteritis, and this diagnosis should be considered in all adults older than 50 years who have headache or facial pain. Temporal arteritis may be related to widespread rheumatologic involvement such as polymyalgia rheumatica. Symptoms may include easy fatigability, weight loss, anorexia, and unexplained fevers, as well as proximal myalgias |
|
|
SECONDARY HEADACHE |
Sinus headaches The pain is usually localized to the frontal or maxillary area, and there is tenderness to tapping over the affected sinus. The pain is of low to moderate intensity and is present on a daily basis. Postdural puncture headaches Can occur after lumbar puncture or with epidural anesthesia The headache is due to leakage of cerebrospinal fluid and changes in the pressure within the skull. The headache is usually self-limiting but can last 3 to 5 days |
|
|
VESTIBULAR DISORDERS |
Because the vestibular system provides information about orientation in space, disorders of the vestibular system can cause a devastating abnormal sense of movement, visual instability, and loss of balance. Damage to the peripheral vestibular nerve can arise from a neurologic pathology, mechanical deformation from a nonneurologic pathologic condition, or trauma to the structures surrounding the nerve. |
|
|
COMMON CAUSES |
Benign positional vertigo Episodic, intense vertigo related to head position; is most often a benign disorder called benign paroxysmal positional vertigo Infection Viral infection is common and usually affects the vestibular nerve unilaterally The use of antibiotics in general has decreased the incidence of bacterial infections affecting the vestibular system; however, infections still do arise and can be introduced into the vestibular apparatus. |
|
|
COMMON CAUSES (continued) |
Endolymphatic hydrops and Meniere’s syndrome A disorder relating to the membranous inner ear as a consequence of the overaccumulation of endolymph compromising the perilymphatic space Perilymphatic fistula An abnormal communication of the inner and middle ear spaces, can cause vertigo |
|
|
COMMON CAUSES (continued) |
Ototoxicity Ototoxicity is usually seen in individuals who are given multiple doses of antibiotics over time or one large dose, usually aimed at managing a threatening infection. Damage to the hair cells in the inner ear can result in complete loss of vestibular function within 2 to 4 weeks after these drugs have been given. Mal de Debarquement A syndrome that is named essentially for the symptoms related to “getting off the boat.” It is usually triggered after a long time spent on a ship, such as during a cruise, or by an extended train ride. |
|
|
COMMON CAUSES (continued) |
√ Autoimmune ear disease Rapidly progressive bilateral sensorineural hearing loss, typically characterized by symptoms of pressure and tinnitus in the ears with or without dizziness. Neoplasia Primary carcinoma can directly involve the end organ, the middle ear, or the mastoid. Glomus tumors arethe most common tumor of the middle ear. |
|
|
COMMON CAUSES (continued) |
Traumatic brain injury Complaints of dizziness and imbalance are common after traumatic brain injury (TBI) and may affect as many as 50% of the individuals who experience TBI. Psychologic disorders and somatoform dizziness Forty percent of dizzy individuals have psychologic disorders and, in general, individuals with psychiatric disorders report more disability from dizziness than do individuals without psychiatric involvement. |
|
|
Cerebral Palsy (CP) |
CP • Permanent, nonprogressive neurologic disorder of motor function • Impairment in postural control and movement • Due to – Faulty development – Injury – Damage to motor cortex in the brain • Symptoms usually appear before the age of 2 |
|
|
Typical Signs of CP |
• Spas;city • Muscle weakness • Ataxia • Rigidity • Atypical movement patterns • Slow to reach developmental milestones • Musclesof speech, swallowing and breathing may be involved • Intellectual disabilities and seizures may also occur • Incidence: 500,000 in 2002: cost for care $8.2 billion |
|
|
Pathology |
• Permanent brain insult during pregnancy (prenatal), delivery (perinatal), or shortly after birth (postnatal). • Premature birth: increased risk of CP • Prior to 1980, thought result of birth trauma: only a small fraction due to birth trauma • 2 types 1. Congenital (present at birth) 2. Acquired (after birth within the first few years of life) |
|
|
Congenital CP
|
• Brain damage during pregnancy or around the time of birth • High risk: very low birth weight, premature, multiple pregnancy • Causes 1. Infection during pregnancy 2. Jaundice untreated: athetoid CP 3. Rh incompatibility: mother’s immune cells attack the fetus 4. Oxygen shortage: hypoxic-.‐ischemic encephalopathy 5. Stroke: coagula;on disorder 6. Toxicity: drug or alcohol use during pregnancy 7. Bleeding in the infant’s brain 8. Kidney and UTI |
|
|
Acquired CP |
• Brain damage in the first few months or years of life • Causes 1. Brain infection: encephalitis, meningitis 2. Head trauma or injury: falls, MVA, child abuse |
|
|
CP |
• No cure • Early diagnosis and treatment can improve the child’s chances of independence • Display a wide range of capabilities and level of involvement |
|
|
Classification of CP |
• Muscle tone: the amount of resistance to movement • Tone must be balanced to move smoothly • Types of tone 1. Spas;c: hypertonic 2. Hypotonic 3. Ataxic 4. Athetoid: dyskinetic
• Use Modified Ashworth Scale |
|
|
Spastic CP |
• Most common • Muscles stiff, tight • Increased resistance to passive movement • Abnormal reflexes:clonus: hyperactive • Hypersensitivity to sensory stimuli •Joint movement may be limited: joint deformities |
|
|
Hypotonic CP |
• Decreased tone throughout • Poorly defined muscles • Decreased responses to DTR • Hypermobile joints |
|
|
Athetoid CP |
• Fluctuating tone • Writhing movements |
|
|
Ataxic CP |
• Poor balance & coordination • Gait requires a wide base of support |
|
|
Classification of CP cont… |
• Patternern of motor development 1. Hemiparesis 2. Quadraparesis: tetraparesis 3. Diplegia: involvement primarily in legs 4. Triplegia • May be combined with first classifica;on: spastic quadraparesis |
|
|
Classification of CP cont…. |
• Gross Motor Functional Classification •Categorizes children by degree of severity or functional capacity •Qualita;ve, objective measure of prognosis for gross motor skills |
|
|
Level 1
|
• Infant 1. Can move in & out of sitting 2. Floor sit independently 3. Manipulate objects with their hands before 18 months • Child 1. Ambulate independently before 2.By4 can get up from floor into standing without assistance 3. By 6 can climb stairs • Adolescence 1. Able to ambulate on all surfaces without assistance 2. Can run & jump with reduced speed, balance |
|
|
Level II
|
• Infant 1. Able to maintain floor sitting but must use hands to maintain balance 2. Commando or belly crawling 3. Pulling to stand using furniture • Child 1. Beginning to cruise before age 2
2. By age 4, requires 1-2 hands to floor sit • Transition in & out of sit independently • Pull to stand on stable surface • Crawling reciprocal pattern • Ambulation with assistive device
3. At age 6, can sit on floor with both hands free • Ambulate short distances without assistive devices • Require assistive device when walking in community until age 12 • Climb stairs using rail • Cannot run or jump
• Adolescent 1.By age 12, uneven surfaces, inclines, crowds still difficult 2. Can ambulate without device for most conditions
|
|
|
Level III |
• Infants 1.Can maintain floor sitting when lower back is supported 2. Can roll & creep forward in prone
• Child 1. Between 2 & 4: “W” sit •Creep on stomach or crawl on hands & knees (often without reciprocal leg movement) • May pull to stand on stable surface • Cruise short distances •Walk short distance indoors using assistive device: need assistance for steering 2.Age 6: independent in chair, walk with assistive device, climb stairs with assistance • Adolescence 1.Age 12: can independently ambulate in community with assistive device, climb steps using rail, use wheelchair for longer distances |
|
|
True or False:
A degenerative disease can affect both the gray and white matter of the brain. |
TRUE :) |
|
|
The neuropathic findings observed in a degenerative disease can reflect changes in what components? |
-intracellular abnormalities, cerebral cortex, and subcortical regions MAY be involved. |
|
|
What is the major component of neurodegenerative disease? |
Cellular stress |
|
|
What is the most devastating of any neurodegenerative disease? |
Amyotrophic Lateral Sclerosis (ALS)
*Generally recognized as adult-onset progressive motor neuron disease but is also a complex disease process underlying a multisystem illness
**Also known as Lou Gehrig's disease. |
|
|
What happens (neurologically speaking) with ALS? |
-Degeneration and scarring (sclerosis) of motor neurons in the lateral spinal cord, brainstem, and cerebral cortex
-Both upper CNS and lower PNS motor neurons are eventually involved
-Most patients die within 2-5 years of diagnosis usually from respiratory failure or pneumonia
-Often managed with multiple medications |
|
|
What are the presentations of ALS? |
-Deficits in visual attention, working memory, problem solving -Dysarthria (disturbance in articulation) -Initially present with asymmetric weakness distally moving proximally -Difficulty chewing and swallowing -Muscle wasting and atrophy -Muscle cramping and fasciculations -Lack of dexterity -Spasticity |
|
|
What are some different diagnostic findings in ALS? |
-Clinical features of weakness, atrophy, and fatigue -Electromyography -Unstable motor units -Increased duration/amplitudes -Low amplitude polyphasic motor unit potentials -Muscle enzymes, such as creatine phosphokinase -Cerebrospinal fluid normal -No changes on myelogram |
|
|
Are Alzheimer's Disease (AD) and Dementia the same thing? |
Negative, ghost rider! |
|
|
What is dementia? |
Decline in intellectual functioning which interferes with a person's relationships and ADL abilities. |
|
|
What is Lewy Body Dementia? |
Overlaps with AD with mental decline and Parkinson's with physical decline
((Lewy bodies are plaques that are seen in the brain, also found in Parkinson's patients)) |
|
|
What is Alzheimer's Disease (AD)? |
-Disruption of multiple neurotransmitters - chiefly ACETYLCHOLINE!
-Multiple drug therapies available that slow the effects on symptoms, but nothing to affect the pathology itself
-Regular physical activity is good for patients |
|
|
What are different presentations of AD? |
-Visuaospatial defecits make it difficult to navigate the environment -Personality changes - indifference, irritability, impulsivity, and egocentricity -Inability to recall current events -Difficult to find words -> inability to remember names -> diminished comprehension -Social situations are difficult |
|
|
What is Dystonia? |
-Neurologic syndrome dominated by involuntary, sustained muscle contractions causing twisting and repetitive movements |
|
|
What is Huntington's Disease? |
-Progressive hereditary disorder characterized by abnormalities of movement, personality disturbances, and dementia |
|
|
What is Multiple Sclerosis (MS)? |
-Typically occurs in ages 25-40 -Major cause of disability in young adults -MS is a disease of temperate climates -Characterized by sclerotic plaques throughout the CNS: plaques block neural transmission causing weakness, sensory loss, and visual dysfunction, also demyelinating or progressive loss of myelin sheath that insulates the nerve and improves conductivity of neural impulse -Genetic component |
|
|
What are the 4 types of MS? |
1. Relapsing-remitting - most common: periods of dysfunction followed by complete resolution 2. Secondary progressive: initial relapse and remission that steadily becomes progressive 3. Primary progressive: steady decline in neurologic function 4. Progressive-relapsing: progressive from onset with clear exacerbations |
|
|
What are the clinical presentations of MS? |
-Optic neuritis - painful decrease or loss of vision -Parasthesia or hyposthesia in an extremity and ascending over time -Fatigue - most common and disabling symptom -Upper motor neuron symptoms -Weakness secondary to decreased neuromuscular impulses -> heat sensitivity cauess greater weakness -Cranial nerve lesions -Speech problems -Ataxia -Depression -Bladder urgency, frequency, and incontinence -Pain from spasticity, neuropathy |
|
|
Medical Management of MS: |
-Diagnosed with MRI of brain and spinal cord -Pharmaceutical mgmt: for spasticity, immune modulation, urological issues, meds to reduce episodes of relapsing
-usually not fatal; largest factor that impacts quality of life and health is pts ability to amb (if they have to be in a WC) |
|
|
What causes Parkinson's Disease (PD) and Parkinsonism? |
-Atrophy of the brain leading to degeneration of neurons in the basal ganglia -a chronic progressive disease of the motor component of the CNS
|
|
|
What are thought to be causal relationships of PD? |
-toxin and infectious exposures, smoking, increased formal education -exercise is thought to be protective |
|
|
What is the "classic triad of symptoms" of PD? |
-Tremor, rigidity, and akinesia |
|
|
What are other symptoms of PD? |
-Difficulty with movement activation and loss of automatic and reflexive movements -Bradykinesia - slowing of movement -> extremity movement and mouth movements; can even have freezing of movements -weakness and fatigue -Depression due to lack of Dopamine (replaced with Levadopa) -Dementia is found in 50% of pts with PD |
|
|
True or False:
Dementia is found in 25% of patients who have Parkinson's Disease. |
FALSE! Dementia is found in 50% of patients who have PD |
|
|
What are presentations of Parkinson's gait and posture? |
-Decreased ROM in LE, trunk, and pelvis -Decreased step length -Absence of recriprocal arm swing -Narrow based gait -Shuffling and decreased speed -Flexion of neck, trunk, hips, and knees -Forward head and trunk pulls weight bearing anterior |
|
|
What are causes of balance impairment in PD? |
-Loss of postural reflexes -Visuospatial Deficits -Retropulsion -Start hesitation -Freezing -Festinating gait -Orthostatic hypotension -True vertigo |
|
|
What is another term for a stroke and what causes this to happen? |
Cerebral Vascular Accident (CVA)
-An interruption of blood supply to the brain, either through hemorrhage or ischemia.
-This is the third most common cause of death in the US
-Cerebral vascular disease is the primary cause of stroke |
|
|
Review the humonculus (picture that shows what functions and parts of the body are affected when a stroke happens to different cerebral arteries)!! |
:) |
|
|
What is the highest vascular risk factor for stroke? |
Hypertension |
|
|
What are some other vascular risks factors for stroke? |
-Smoking -Diabetes -Obesity |
|
|
What are some other factors that can set a person up for a certain stroke mechanism? |
-Artherosclerosis (clogged or blocked arteries) -Cardioembolism (cardiac disease) -Small vessel disease -Maternal or paternal family history of stroke -Cardiac diseases -Diseases involving increased fibrin: **Rheumatic heart disease, endocarditis, artherosclerosis, thrombocytosis |
|
|
What are the warning signs of stroke? |
-Sudden weakness or numbness of the face, arm, or leg -Sudden dimness or loss of vision particularly in one eye -Sudden difficulty speaking or understanding speech -Sudden severe headache with no known cause -Unexplained dizziness, unsteadiness, or sudden falls |
|
|
What is FAST (in terms of warning signs for stroke)? |
F: Face - changes in facial expression; one side drooping A: Arm - one arm doesn't go as high as the other when lifted S: Speech - non-audible speech T: Time - the quicker the patient gets to the hospital, the better the chance of treatment |
|
|
What can cause an ischemic stroke? |
-Occlusion of major arteries due to thrombosis (blood clot within vein) or embolism (traveling clot in the artery); this is often due to other cardiac conditions |
|
|
What can take place after an ischemic stroke happens? |
-Second vascular responses: a cumulative effect of small occlusions happening elsewhere in the artery that increase in number and progressively impair blood flow
-Secondary neuronal damage: injury to neurons due to hypoxia (lack of oxygen) and ischemia (lack of blood) -Can be mild if blood flow is quickly restored
**Stroke-loss of blood and oxygen to an area of the brain -> Vascular response-neural damage** |
|
|
What are the 5 ischemic stroke syndromes and what do they consist of? |
-Anterior cerebral artery syndrome -Middle cerebral artery syndrome -Posterior cerebral artery syndrome -Vertebral and posterior inferior cerebellar artery syndrome -Superior cerebellar artery syndrome |
|
|
What is affected by an anterior cerebral artery syndrome? |
-Minimal dysfunction, hemiparesis and LE involvement; not quite as severe |
|
|
What is affected by a middle cerebral artery syndrome? |
-Middle cerebral artery is most common site of emboli -contralateral (meaning that if the stroke happens on the left side of brain, the right side of the body is affected and vice versa) hemiplegia and hemianesthesia -speech and oral-motor problems -motor weakness |
|
|
What is affected by a posterior artery syndrome? |
-Subthalamus, medial thalamus, ipsilateral cerebral peduncle and midbrain -Abnormal sensations of pain, temperature, proprioception, and touch - often exaggerated -Perseveration, disinhibition, personality changes -Hemiplegia, ataxia -Coma and decerebrate rigidity -visual deficits -Memory disturbance |
|
|
What is affected by vertebral and posterior inferior cerebellar artery syndrome? |
-Brainstem, medulla, and cerebellum -Wallenburg syndrome - vertigo, nausea -Ipsilateral ataxia -Sensory impairment to ipsilateral face and contralateral trunk and extremities -Edema can cause respiratory distress from raised ICP |
|
|
What are ways to prevent and treat ischemic stroke? |
Prevent: manage blood pressure, control edema and ICP, Antithrombotic agents ( clot dissolvers - 3 hour window to treat and prevent stroke)
Treatment: long term meds - anticoagulants and lipid lowering drugs, meds for spasticity, urinary incontinence and depression
*Recovery is most rapid in first 3 weeks but can continue for up to 5 years. Prognosis is better for ischemic stroke than hemorrhagic stroke |
|
|
What is an intracerebral hemorrhage (ICH)? |
-Bleeding from an arterial source into brain parenchyma.
-Two types: Primary ICH - spontaneous and usually attributed to vascular weakness due to HTN or aging, and Secondary ICH - due to trauma, impaired coagulation, toxin exposure, or anatomic lesion
**Most deadly stroke of subtypes** -More frequent among men -Can be an effect of using thrombolytics for ischemic strokes |
|
|
What are the risk factors for ICH? |
**Hypertension (HTN) is most important and modifiable risk factor
-Thrombolytic use for ischemic stroke -Long term use of coagulants
|
|
|
What causes an ICH? |
-Changes in vascular structure: smooth muscle replaced by collagen -> changes permeability -> accumulation of fat deposits and vessel walls become prone to leakage -> necrosis of the endothelium
-Hemorrhagic transformation - conversion of an ischemic infarct into a hemmorhage due to secondary bleeding |
|
|
What are syndromes of ICH? |
-Symptoms usually occur gradually vs. rapidly as with ischemic stroke -As the hematoma enlarges, the focal symptoms increase -If ICP rises, you see headache, vomiting, and decreased alertness -**Headache is most common sign of superficial and large hemorrhages -Table 21-1 |
|
|
How is an ICH medically managed and what is the prognosis ? |
Management: reduce elevated BP, control edema/ICP, Vitamin K may reduce prothrombin time, airway management depending on area of bleed
Prognosis: High mortality rate but also high functional recovery, the larger the bleed the greater the chance of mortality, severe neurologic deficits |
|
|
What is a subarachnoid hemmorhage (SAH) and what can cause it? |
--Can begin with the sudden onset of a headache with searing pain, sometimes the headache begins with exertion -results in frank blood in the subarachnoid space between the arachnoid and the pia matter
**Aneurysm and vascular malformations are responsible for most SAHs -can also be caused by trauma, developmental defects, neoplasm or infection |
|
|
What are the risk factors for an SAH? |
-Smoking, alcohol use, and HTN |
|
|
Presentation and medical management for SAH: |
Presentation: *headache in 40% - nausea, vomiting, syncope, confusion, lethargy, coma, and seizures
medical management: -often misdiagnosed - increased mortality -CT scan is scan of choice when diagnosing but the longer the scan is done from onset of symptoms, the less sensitive and ten may need a lumbar puncture to diagnose -neurological consult for prevention of management of secondary complications |
|
|
What is a traumatic brain injury (TBI) and how does it occur? |
-A TBI results from external force with the potential to cause mild to complex alterations of brain function. ((-Initially present with altered or diminished state of consciousness -Results can effect behavior, emotion, psychological function or cause disability))
*Falls are the leading cause of TBI and MVAs (motor vehicle accident) are second leading cause
-Greatest medical challenge: balancing cerebral perfusion and ICP |
|
|
What are the two types of TBIs? |
-Open head injury - skull has been penetrated and the brain is exposed
-Closed head injury - soft brain tissue comes in contact with the hard skull ->Coup injury - the initial time the brain contacts the skull -> Contacoup injury - deceleration of the brain against the opposite side of the skull (OFTEN WORSE) |
|
|
Pathogenesis for TBI: Vascular changes |
-cerebral contustions (bruise) -vascular damage causes infarction in grey matter -can also see subarachnoid hemorrhage, subdural hematoma and hydrocephalus -all can result in increased blood volume which can affect ICP -Fluid flow can be blocked compounding the issue -Result - the body cannot regulate homeostasis |
|
|
Pathogenesis for TBI: Parenchymal changes |
-Diffuse axonal injury - shear and tensile forces tear axons
|
|
|
Pathogenesis for TBI: compressive damage |
-intracranial HTN can produce herniation no longer making the brain symmetrical
-with closed head injury, herniation occurs through the foramen magnum
|
|
|
Pathogenesis for TBI: hypoxia |
-HTN can initially occur in severe TBI
-Caused decreased blood flow to the brain or decreased oxygen in the blood due to pulmonary insult
|
|
|
Pathogenesis for TBI: HTN |
-Alters regulation of blood and fluid volume in the brain leading to greater secondary damage |
|
|
What are the 3 levels of TBI? |
Mild TBI: concussion
Moderate TBI: structural damage, death is uncommon
Severe TBI: cognitive, physical damage and perhaps death |
|
|
What is typical presentation of a concussion? |
-May or may not have loss of consciousness -Postconcussion syndrome - can last 7 days to 3 months; includes dizziness, disorientation, nausea, and headache; irritability, difficulty reading, and with memory -Have lower level changes in neurons, axons, and neurotransmitter metabolism
**-Second impact syndrome - cumulative result of multiple concussions - can lead to long term brain damage and disability |
|
|
What are the grades of concussion? |
Grade 1: transient confusion or no loss of consciousness with resolution of symptoms within less than 15 min; may return to play that day if sideline neuro exam is normal
Grade 2: same as above, but last longer than 15 min; should not return to play same day
Grade 3: loss of consciousness; should not return to play on same day |
|
|
What are the two levels of consciousness listed in the PowerPoint and how are they measured? |
Coma - lowest level of consciousness; unable to obey commands, utter words, open eyes; unresponsive
Persistent vegetative state - continued reduced level of consciousness
*Levels of consciousness are measured with the Glasgow Coma Scale - one of the greatest predictors of outcome following a TBI |
|
|
What are the clinical manifestations TBI? |
Respiratory impairments: -Cheyne-strokes breathing (altered rapid breathing and stopping of breathing) - occurs with lesions to the hemispheres or diencephalon -Hyperventilation - irregular inhale without equal exhale
Pain: -head and neck is common -can affect attention span/distract pt -can also see neuropathic pain and myofascial pain |
|
|
Cognitive impairments of TBI: |
-Measured with the Ranchos Los Amigos scale - assesses cognitive recovery
-Retrograde amnesia - unable to recall events that occurred immediately before the injury
-Posttraumatic amnesia - period between injury and when memory returns; indicator of severity of the TBI
-Can also have anterograde memory loss - inability to form a new memory |
|
|
Other clinical manifestations that may occur with TBI: |
-Cranial nerve damage: changes in the function of the senses; pupillary response, blindness, eye movement, smell, taste, hearing, vestibular
-Motor deficits: varying levels of plegia/motor function -> tone, spasticity, and rigidity
-Decorticate posturing: loss of cortical control: flexor tone in UE and extensor tone in LE
-Decerebrate posturing: loss of cerebral control: extensor tone in UE and LE
-Balance, motor control, cerebellar dysfunction
-Heterotrophic ossification: abnormal bone growth around a joint, possibly due to elevated levels of alkaline phosphates, leads to loss of motion, tenderness, erythema, edema and pain
-Other medical complications: cardiovascular - dysrythmias, pulmonary - edema, aspiration, and emboli |
|
|
Medical management for TBI: |
-Diagnosis starts at level of consciousness -Pupillary responsiveness -Conduct MRI and CT but these do not necessarily quantify the extent of injury -Assessment of cognitive deficits -Can also have spine and spinal cord injury |
|
|
3 types of treatment for TBI: |
Acute: resuscitation if necessary, obtain airway to minimize hypoxia -control hypoxia and hypotension and secondary brain damage from edema and increased ICP -surgery -decompression of the skull -control blood pressure and any cardiac issues
Subacute: pharmacological treatment of spasticity and seizures
Rehab: restore mobility and function, community re-entry, cognitive rehab |
|
|
Prognosis for TBI patients: |
-Greatest predictors of outcome: duration of altered consciousness and posttraumatic amnesia
-Acute hemispheric swelling with extra cerebral hematoma, unilateral brain contusion and DAI carry poor prognosis
-Epilepsy occurring within first 7 days of injruy
-Dementia |
|
|
What is a leading cause of death among children? |
TBI
-Nonaccidental injury is a common cause of head injury in infants and toddlers and is often the result of battered child syndrome |
|
|
How does a spinal cord injury (SCI) occur? |
-A catastrophic event of low incidence -Occurs most often in active persons -Rarely occurs in isolation, with more than 75% of these individuals having some other systemic injruy
Primary cause: MVAs (also falls, acts of violence and sporting injuries)
Classified as concussion (caused by a blow or violent shaking), contusion (glial tissue and spinal cord remain intact but loss of central gray and white matter), or laceration (glia interrupted and spinal cord may be torn, knife wound and punctures).
-Hemorrhage is common -Often due to excessive flexion |
|
|
What is a Hangman's Fx? |
-A fx of C2, typically caused by forced flexion, can cut into or sever spinal cord |
|
|
Primary injury of spinal cord: |
-Structural damage occurring immediately after injury; destruction of neurons, hemorrhage and vascular damage |
|
|
Secondary injury of spinal sord: |
-Occur as a result of the primary injury; death of axons, ischemia, hypoxia, edema |
|
|
Other pathologies involved with SCI: |
-Blood flow changes: decreased oxygen to grey (processing function of CNS) and white matter ("doing" function of the CNS) for cell survival and function, increased edema causes increased pressure on the spinal cord, occurs more often in grey matter because blood supply is more superfluous here.
-Edema: forms at immediate injury site and spreads
-Demyelination: decreased nerve signal firing
-Dural scarring: scarring can decrease free cord movement and restrict motion - limits regeneration and recovery
-Neural function: injured CNS undergoes premature aging including abnormal cell production and impairments in cell repair |
|
|
What does ASIA stand for? |
American Spinal Cord Association |
|
|
What are the levels of SCI injuries? |
*Generally, SCI in cervical spine will result in tetraplegia which is the paralysis of all limbs and trunk
-Thoracic or lumbar SCI: paraplegia
-Complete SCI: complete loss of motor and sensory function below level of injury
-Incomplete SCI: partial loss of motor and sensory function below level of injury |
|
|
What are the 5 SCI syndromes? |
Brown-Sequard syndrome: damage to one side of the spinal cord - usually due to GSW or stab, deficits are ipsilateral to the lesion
Anterior cord syndrome: loss of blood supple by the anterior spinal artery - due to flexion injury, results in loss of bilateral function
Central cord syndrome:damage to the central spinal cord - due to extension injuries in the cervical spine - more severe injuries in UE than LE
Posterior cord syndrome: loss of proprioception below the lesion - very rare, pt will have wide based stepping gait
Conus medullaris syndrome and Cauda equina syndrome: damage at base of spinal cord - causes LE paralysis and bowel/bladder issues |
|
|
True or False:
A SCI in the cervical spine will result in tetraplegia, or paralysis of all limbs and trunk. |
TRUE |
|
|
What SCI syndrome includes damage to only one side of the spinal cord? |
Brown-sequard syndrome |
|
|
What SCI syndrome results in the loss of bilateral motor function? |
Anterior cord syndrome |
|
|
Damage at the base of the spinal cord can cause what? |
LE paralysis and bowel/bladder issues |
|
|
What are some other clinical manifestations present with SCI? |
-Changes in muscle tone: loss of sensory, motor, and autonomic control (sweating and reflex incontinence), spasticity
-Autonomic nervous system changes: Autonomic dysreflexia - impaired function of the ANS causing simultaneous sympathetic and parasympathetic activity, can occur in SCI at T5 and above
-Skeletal changes: heterotrophic ossification and changes in bony alignment
-Respiratory complications: Lesions above C4 require artificial ventilation; C5-T12 - loss of innervation of muscles of respiration, decreased ability to cough, pneumonia can result
Cardiovascular conditions: Hyperinsulinemia or insulin resistance, osteoporosis
-Pressure ulcers
-Bowel and bladder control: Conus medullaris - spinal center for urination; reflex neurologic bladder-spasticity, difficulty voiding, urethral refuls (lesions above conus medullaris); nonreflex bladder-decreased tone (lesions at conus medullaris); increased risk for UTI
-Bowels follow same pattern |
|
|
Medical management for SCI |
-Focus to prevent further neurological deterioration -Correct stabilization and handling -Meds given to prevent edema -Halo for cervical injuries -Steroids -Ventilation for cervical injuries -Manage cardiovascular system with ANS involvement -Spasticity managed with meds -Promote regeneration to improve function; stem cell transplant |
|
|
What is Cerebral Palsy (CP)? |
A permanent, nonprogressive neurologic disorder of motor function
-Impairment in postural control and movement -Due to: ->faulty development, injury, damage to motor cortex in the brain
-Symptoms usually appear before the age of 2 |
|
|
What are the typical signs of CP? |
-Spasticity -Muscle weakness -Ataxia -Rigidity -Atypical movement patterns -Slow to reach developmental milestones -Muscles of speech, swallowing, and breathing may be involved -Intellectual disabilities and seizures may also occur |
|
|
What causes CP? (Pathology) |
-Permanent brain insult during pregnancy (prenatal), delivery (perinatal), or postnatal -Premature birth can bring an increased risk of CP -Before 1980, birth trauma was thought to be main cause when actually only a small fraction due to birth trauma |
|
|
What are the two types of CP? |
1. Congenital (present at birth) 2. Acquired (after birth within the first few years of life) |
|
|
What causes of congenital CP? |
-Brain damage during pregnancy or around the time of birth -HIGH RISK: very low birth weight, premature, multiple pregnancy
-Causes: 1. infection during pregnancy 2. Jaundice untreated 3. Rh incompatibility: mother's immune cells attack the fetus 4. Oxygen shortage: hypoxic-ischemic encephalopathy 5. Stroke: coagulation disorder 6. Toxicity: drug or alcohol use during pregnancy 7. Bleeding in the infant's brain 8. Kidney and UTI |
|
|
What can cause acquired CP? |
-Brain damage in the first few months or years
Causes: 1. Brain infection: encephalitis, meningitis 2. Head trauma or injury: falls, MVA, child abuse |
|
|
Is there a cure for CP? |
No. -Early diagnosis and treatment can improve the child's chances of independence -Display a wide range of capabilities and level of involvement |
|
|
How is CP classified and what are the different types? |
-Muscle tone: the amount of resistance to movement -Tone must be balanced to move smoothly -Types of tone: 1. Spastic: hypertonic 2. Hypotonic 3. Ataxic 4. Athetoid: dyskinetic *Modified Ashworth scale is used to assess, grade, and quantify |
|
|
What is the most common type of CP? |
*Spastic CP* |
|
|
What are the presentations of spastic CP? |
-Muscle stiffness; causes poor ROM -Increased resistance to passive movement -Abnormal reflexes: clonus (test for upper motor neurom involvement): hyperactive -Hypersensitivity to sensory stimuli -Joint movement may be limited: joint deformities |
|
|
What type of CP presents with decreased tone throughout, and hypermobile joints? |
Hypotonic CP
-other presentations: -poorly defined muscles -decreased response to DTR (deep tendon reflex; decreased or absence of reflex) |
|
|
Type of CP that presents with fluctuating tone and writhing movements: |
Athetoid CP |
|
|
What are the presentations of Ataxic CP? |
-Poor balance and coordination -Gait requires a wide base of support ((affects cerebellum; poor balance=poor coordination)) |
|
|
What are the 4 different patterns of motor development? |
(paresis = weakness)
1. Hemiparesis 2. Quadraparesis: tetraparesis 3. Diplegia: primarily in legs 4. Triplegia: legs and one arm usually --May be combined with first classification: spastic quadriparesis |
|
|
What is the gross motor functional classification? |
-Categorizes children by degree of severity or functional capacity -Qualitative, objective measure of prognosis for gross motor skills |
|
|
Level 1:
Least severe |
->Infant: can move in and our of sitting, floor sit independently, and can manipulate objects with their hands before 18 months ->Child: can ambulate independently before 2, by 4 can get up from floor into standing without assistance, by 6 can climb stairs ->Adolescence: able to ambulate all surfaces without assistance |
|
|
Level 2: |
->Infant: able to make floor sitting but must use hands to maintain balance, commando or belly crawling, pulling to stand using furniture ->Child: begins to cruise before age 2, by age 4 requires 1-2 hands to floor sit, ambulate with assistive device -> at age 6 can sit on floor with both hands free, ambulate short distances without assistive devices but must use devices while in community, cannot run or jump |
|
|
Level 3: |
->Infants: can maintain floor sitting when low back is supported, can roll and creep forward in prone ->Child: between 2-4 can "W"sit, crawl, pull to stand, cruise short distances, walk short distance indoors with assistive device, by age 6 can sit in chair independently, climb stairs with assistance ->Adolescent: can independently ambulate in community with assistive device |
|
|
Level 4: |
->Infant: have head control, trunk support is needed for sitting ->Child: age 2 rolling independently, age 4 can sit when placed with both hands on floor for balance, need adaptive devices for sitting and standing, roll and creep, age 6 can sit independently in chair with trunk stabilization for balance and use of hands, transfers require assistance, ambulate short distance with assistive device ->Adolescence: by age 12, may still rely on wheeled mobility system |
|
|
Level 5:
mots severe |
->Infant: before age 2, limited voluntary control of movement, unable to hold head or trunk against gravity, require assistance to roll ->Adolescent: cannot sit, stand, or walk, adaptive equipment used extensively, some use power mobility systems |
|
|
What are some clinical signs of CP? |
-Difficulty with motor control and movement -Difficulty maintaining normal posture -Affected tone -Affected speech -Rounded posture |
|
|
What are common warning signs? |
*Over 2 months*: 1. head lag with pull to sit 2. muscles feel stiff 3. overextended back and neck 4. acts as if pushing away when cradled 5. legs get stiff and scissor when picked up
*Over 6 months* 1. continues to have asymmetric tonic neck reflex 2. reaches out with only one hand, other hand stays fisted
*Over 10 months* 1. crawls in lopsided manner 2. pushes off with one hand and leg, drags the others 3. scoots around on butt or hops on knees; does not crawl on all 4s |
|
|
What are the pharmaceutical interventions for spasticity?
(unsure if we need to know these, but good for review) |
1. Balcofen: oral or into cerebrospinal canal through a pump; pumps don't result with side affects of drowsiness, dizziness, weakness, confusion; rarely used for children under 4 2. Botox injections into the muscle 3. Phenol injections into the nerve: strips myelin form the nerve sheath thus reduces muscle tone 4. Diazepam 5. Dantrolene |
|
|
What are the pharmaceutical interventions for seizure?
(unsure if we need to know these, but good for review) |
1. First visited with phenobarbital, phenytoin (dilantin), carbamazepine (tegretol) or sodium valproate (depakote) 2. Newer medicines include: Lamictal and Neurontin |
|
|
What is the Peripheral Nervous System (PNS) include? |
-somatic motor and sensory components of cranial and spinal nerves arising from neurons with cell bodies located within the brainstem and spinal cord or in dorsal root ganglia
-signs and symptoms of PNS involvement relate to motor and sensory systems as well as the ANS - affects myelin, axon, cell body |
|
|
What are potential sites of involvement in the PNS? |
-Lower motor neuron involvement:
->cell body of alpha motor neuron ->axons ->motor end plate ->muscle fibers |
|
|
True or False:
Disorders of the PNS can be due to neuropathies or myopathies. |
True |
|
|
Damage to the PNS can be due to.... |
-Hereditary -trauma -infections -toxins -metabolism
-Nerve fibers demyelinate or degenerate -Usually. the longer nerve fibers are affected first then progress proximally |
|
|
What is neuropraxia? |
Segmental demyelination, usually due to compression causing ischemia
**Regeneration is possible |
|
|
What is axontmesis? |
The axon is damaged, compression causes infarction and necrosis |
|
|
What is neurotmesis? |
Severance of axon and disruption of supporting structures
-stab wounds, avulsions -causes distal axons to degenerate, muscle atrophy -requires surgery to regenerate |
|
|
Signs and symptoms of PNS dysfunction: |
-sensory s/s follow a dermatomal pattern -muscle paresis or paralysis in muscles distal to lesion of peripheral nerve -if spinal nerve root, all muscles receiving axons from that level are affected (myotomal pattern) -tingling, prickling, burning -glove-like presentation when multiple nerves are involved -can see changes in muscle tone and reflexes -myopathy - weakness tends to be proximal -neuropathy - sensory s/s and motor s/s occur first distally |
|
|
What is Charcot-Marie-Tooth disease (CMT)? |
-also known as hereditary motor and sensory neuropathy or peroneal muscular atrophy -rare; 1:2500
--progresses to the muscles of the forearms and hands
|
|
|
What causes CMT and what are some signs and symptoms of it? |
-pathology: protein mutations cause demyelination
-Clinical signs: distal muscle weakness (dorsiflexors and evertors), atrophy, diminished reflexes, pes cavus, foot drop with high steppage gait, wasting on intrinsic muscles in hands (between metacarpals) |
|
|
What is idiopathic facial paralysis? |
*Bell's Palsy*
-Common condition in which the facial nerve is unilaterally affected -People with DM and pregnant women have an increased chance of Bell's Palsy - affects 20:100,000 per year -Develops rapidly, sometimes overnight
-Asymmetrical facial expression; mouth droops, eyelid does not close, nasolabial fold is flattened; sensory loss - taste, salivation -Treated with steroids and antivirals |
|
|
What is Thoracic Outlet Syndrome (TOS)? |
An entrapment syndrome caused by pressure form the structures in the thoracic outlet on fibers of the brachial plexus at some point between the interscalene triangle and the inferior border of the axilla
*Involves branches of the brachial plexus and/or subclavian artery |
|
|
What causes TOS? |
*Poor posture is a risk factor -Compression causes edema and ischemia in the nerves leading to neurapraxia ->will often see parasthesias and pain in the arm, often at night ->vascular symptoms: coldness, edema in hand or arm, Raynaud's (cold sensitivity), fatigue in hand and arm |
|
|
What is diabetic neuropathy? |
-Occurs in conjunction with DM with or without other causes for peripheral neuropathy -Can be focal or diffuse -Distal, symmetrical pattern (diabetic polyneuropathy) -Thought to be due to metabolism disturbances -Loss of myelinated and unmyelinated axons -Vascular changes may also affect peripheral nerves in patients with DM |
|
|
What is Guillain-Barre syndrome? |
-Immune-mediated disorder - bacterial, viral, infections, surgery, and VACCINATIONS (recently found that pts who have received chemotherapy then a flu shot shortly after acquire this) -Lesions throughout the PNS from the spinal nerve roots to the distal termination of motor and sensory fibers -Rapidly ascending symmetrical motor weakness and sensory impairments -Can affect cardiac function due to ANS involvement and respiratory function due to ascending nature of pathology |
|
|
Is recovery typical for Guillain-Barre syndrome? |
Yes, but can have reoccurring episodes |
|
|
What is post-polio syndrome? |
-Occurs decades after a patient has polio -Neuromuscular s/s -thought to be due to widespread reinnervation - nerves responsible for a greater area -cannot maintain proper innervation
Presentation: decreased muscle strength, pain, atrophy, loss of function |
|
|
What is Myasthenia Gravis? |
-Fluctuating weakness and fatigability of skeletal muscles -Autoimmune disorder that affects the neuromuscular junction and motor endplate -Decreased number of ACH receptors which affects nerve impulse -Broad spectrum of muscle weakness and fatigability
Presentation: Facial weakness, unable to open jaw and eyelids |