Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
19 Cards in this Set
- Front
- Back
|
What is the mechanism of action of acetaminophen?
|
Inhibits COX-2 preventing PGE2 synthesis resulting in analgesia and antipyresis
|
|
|
How is acetaminophen metabolized?
|
In the liver it is:
-Conjugated with glucuronide (40-67%) -Conjugated with sulfate (20-46%) -Oxidized by cytochrome P450 2E1 to NAPQI and conjugated with glutathione |
|
|
When/how does acetaminophen toxicity occur?
|
When the amount of NAPQI produced outstrips glutatione stores NAPQI begins binding to cell proteins in the liver causing zone III (centrilobular) necrosis.
|
|
|
What is the antidote to acetaminophen and how does it work?
|
N-acetylcysteine (aka NAC, Mucomist) works through 4 mechanisms:
-glutathione precursor (easy to create more glutathione) -glutathione substitute (binds NAPQI) -enhances conjugation to sulfate -scavenges other free radicals |
|
|
What are the 4 stages of acetaminophen toxicity?
|
1 - Preinjury: 0-12h
2 - Injury: 8-36h 3 - Maximal injury: 2-4 day 4 - Recovery: >4 days |
|
|
How is the need for treatment determined in an acute ingestion?
|
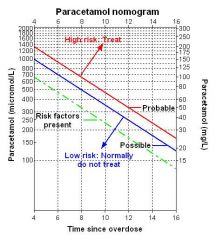
Using the Rumack-Mathew Nomogram
|
|
|
Approximately how many mg/kg of acetaminophen are required to produce a toxic level?
|
150mg/kg
|
|
|
How far post ingestion can the first value be plotted on the Rumack-Mathew nomogram in an acute overdose? When does treatment need to begin?
|
Values can be plotted at or after 4 hours when absorption should be nearly complete. Liver damage generally does not occur until 6-8 hours. NAC can usually be delayed until then with no adverse effect.
|
|
|
How does assessment of acetaminophen OD change in chronic ingestion?
|
The nomogram can not be used. Likelihood of toxicity is increased with larger total doses and longer durations. Assess for damage with AST/acetaminphen level. Treat if evidence of liver damage or high level.
|
|
|
Who is at increased risk of acetaminophen toxicity?
|
-patients using medications that use cytochrome P450 2E1 inducers such as isoniazid and ethanol
-malnourished patients |
|
|
How should assessment of acetaminophen overdoes change in pregnant patients?
|
It shouldn't. Follow the same guidelines. Perhaps have a lower threshold for observation.
|
|
|
Is activated charcoal indicated for isolated acetaminophen overdose?
|
No. There is an effective antidote. AC has no proven efficacy.
|
|
|
What are the pros/cons of PO vs IV N-acetylcystine?
|
PO - poor taste, causes emesis, delivered directly to the liver, 72 hour protocol
IV - can have anaphylactoid reaction, only route studied in confirmed liver failure, 21 hour protocol |
|
|
What symptoms can be present from an anaphylactoid reaction to NAC?
|
2-6% gett skin rashes and flushing
~1% get angioedema, bronchospasm and hypotension -Reactions are dose/rate dependant and are treated by pausing/slowing the infusion and giving fluids and antihistamines +/- steroids if needed |
|
|
What are the criteria for predicting death/transplant in acetaminophen toxicity?
|
The King's College Criteria
-Lactate >3.5 (4h post resuscitation) -pH <7.3 (12h post resuscitation) -Cr >300mmol/L -INR >6.5 -Grade III/IV encephalopathy (somnolence disorientation, asterixis) -Phosphorus >1.2mmol/L |
|
|
Describe the preinjury stage of acetaminophen toxicity
|
0-12h, N/V/anorexia/malaise; elevated acetaminophen
|
|
|
Describe the injury stage of acetaminophen toxicity
|
Injury; 8-36h, N/V/RUQ pain; transaminitis</div><div>
|
|
|
Describe the maximal injury stage of acetaminophen toxicity
|
2-4 days; encephalopathy, coagulopathy, hemorrhage, acidosis; ARDS, SIRS, MOSF, cerebral edema, hemorrhage
|
|
|
Describe therecovery stage of acetaminophen toxicity
|
>4 days; histologic hepatic recovery over weeks... or death
|