Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
7 Cards in this Set
- Front
- Back
|
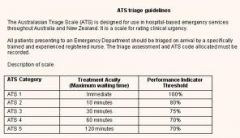
What is the maximum waiting period of the 5 categories of the ATS? What is the performance indicator threshold (% to be seen in time as suggested by ACEM)
|
|
|
|
Regarding the australian triage scale which is incorrect
1 triage categories are a measure of severity 2 triage is an ongoing process 3 the principles of triage include equity and efficiency 4 more in hospital deaths occur in category four (ATS4) patients than any other category 5 the death rate of category 1 patients is 16% |
1 INCORRECT - they measure urgency, NOT severity, complexity or prognosis
2 e.g should not just occur 'at the door' but be repeated as required 4, 5 ATS4 has 37% of total deaths, but a death rate of only 0.9%. ATS1 has 14% total deaths, rate of 16% |
|
|
Regarding triage, how do the principles of equity and efficiency apply?
|
Equity (justice) - the distribution of resources for treatment is fair, including treating the most urgent before those who arrived first
Efficiency - best use is made of available resources Overall philosophy is doing greatest good for greatest number |
|
|
Regarding the ATS, which is incorrect
1 answers the question of the maximum wait a patient should have for medical assessment and Rx 2 triage inconsistencies may occur in categorising mental health and pregnancy related problems 3 triage category correlates well with use of resources in the ED 4 triage category strongly predicts ED outcome 5 outcome at hospital discharge is predictable by triage category |
5 INCORRECT - poor predictor
|
|
|
What is the appropriate category for the following patients?
1 stable neonate 2 immediate threat of violence 3 mental health patient with social crisis, otherwise stable 4 behavioural problem without risk to others 5 suspected NAI 6 BSL>16 7 severe pain 8 chest pain, not likely cardiac 9 eye problem normal vision 10 mild haemorrhage |
1 - 3
2 - 1 3 - 5 4 - 4 5 - 3 6 - 3 7 - 2 8 - 3 9 - 4 10 - 4 |
|
|
List some of the problems and limitations of triage
|
1 inter-observer variability
2 institutional variability (e.g. Smaller hospitals may allocate higher priority to same cases than larger hospitals) 3 regional variability 4 limited information at time evaluation 5 lack of privacy 6 lack of time 7 different perceptions of staff and patients re urgency 8 lack of evidence to support impact on patient outcomes Triage variations can result in inequitable funding and difficulties in performance comparisons |
|
|
How do ATS4&5 patients differ from general practice patients?
|
Admission rates 10-20x higher
More complex evaluation and treatment, which may preclude GP care e.g. Observation period, IV therapy, wound care or plaster Ambulatory (e.g. pt able to be discharged) care does not equate to GP care Improving GP access may result in modest reduction in this category however as they are inexpensive patients to treat this may not be a cost effective alternative |