Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
27 Cards in this Set
- Front
- Back
|
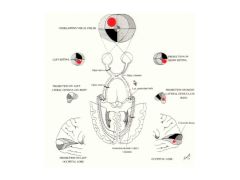
What system allows you to consciously look around and see things?
|
The Lateral Geniculo-Striate Nucleus (LGN) system
|
|
|
Describe the LGN path of the left temporal and right nasal retina nerves to the brain:
|
The start in separate eyes and travel through the optic nerve to the optic chiasm where now they begin to travel together in the optic tract. From there they synapse in the geniculo-striate nucleus of the thalamus. From there the project up through the Optic Radiations into the primary visual cortex located in the Calcarine Fissure of the occipital lobe.
|
|
|
What system is responsible for reflexive orienting your vision?
|
Retino-tectal system.
|
|
|
Describe the Retino-tectal system's path from the retinal nerves to the Extrastriate Cortex.
|
Same as major path except instead of synapsing at the Lateral Geniculate Nucleus, it continues to the superior colliculus to the pulvinar nucleus of the thalamus and finally to the extrastriate cortex.
|
|
|
Why might damage to the temporal lobe produce a restricted visual field defect? What treatment can cause this?
|
Bc it may also damage Myers' loop which are optic radiations that loop down into the temporal lobe. Lobectomies for temporal lobe epilepsy often cause this defect.
|
|
|
Describe the Pupillary Constrictor path:
|
1. Retina
2. Pregeniculate Body 3. Pretectal Area/Post Comm 4. Edinger-Westfal x-over 5. Pupillary Constrictor |
|
|
Why do both pupils constrict when only one eye receives light? What is the technical name for this?
|
Bc an axon from both eyes cross over at the Edinger-Westfal nucleus. This is called the Consensual Light Reflex
|
|
|
Describe the Pupillary Dilator path:
|
1. Retina
2. Pregeniculate Body 3. x-over to Midbrain Reticular Formation 4. Descends to thoracic cord 5. Thru sympathetic chain 6. To superior cervical ganglion 7. Pupillary dilator muscles. |
|
|
Which pupillary control system can be controlled by emotions?
Which is controlled by parasympathetic? Sympathetic? |
1. Pupillary dilator
2. Pupillary constrictor 3. Pupillary dilator |
|
|
Describe the path of for accommodation reflex:
|
1. Retina
2. Through LGN 3. Up through visual cortex 4. down to pretectum 5. x-over thru Edinger Westphal 6. ciliary ganglion |
|
|
Contraction of ciliary muscle causes increased or decreased depth of field? Why?
|
Increased. When muscles contract, the ciliary fibers relax and the lens gets fatter...increasing the magnification and depth of field.
|
|
|
What three things must happen to accommodate for looking at your far finger to looking at your near finger?
|
1. Convergence of the 2 eyes
2. Contraction of the ciliary muscle to thicken lense 3. Contraction of pupillary muscles - this increases the depth of field (like an F-stop on a camera) |
|
|
How is the accommondation reflex pathway unique compared to others? Why is this so?
|
It involves the cerebral cortex. This is necessary to determine if image is blurry or out of focus.
|
|
|
If an object is in the upper left part of the field, where does it show up on the retina?
|
The lower right. The image is upside down and background.
|
|
|
How are the retinal signals split up/distributed to the brain?
|
The right sides of each field/retina are distributed to the left side of the brain.
|
|
|
If an object is in the upper left part of the field, where does it ultimate project in the brain?
|
In the lower right part of the Calcarine Fissure.
|
|
|
What is cortical magnification?
|
Since the fovea contains more ganglion cells than the periphery, this means there are more fibers and cells which requires more cortical area to project neurons to.
|
|
|
Why is a small loss of vision in the center of gaze a serious concern?
|
Because it can indicate a large lesion in the visual cortex (ie calcarine fissure).
|
|
|
Remember to review the injuries and where they show up in a projection. Note that for the optic radiations, top projects to top.
|
Remember to review the injuries and where they show up in a projection. Note that for the optic radiations, top projects to top.
|
|

Name these types of retinotopies
|

1. Heteronymous
2. Hemianopia 3. Homonymous 4. Quadrantanopia |
|
|
Vision is wired into two parts basically termed the "what" and "where or how" is it. Name those respective regions of the brain.
|
What = Temporal lobe
Where = Parietal lobe |
|
|
All of the input from the retina and LGN goes where? From there where does it go (describe the next 2 steps...and then what happens)
|
V1 of the visual cortex. Then it goes to V2 and then V3 and after that it splits to different parts of the brain.
|
|
|
A defect in the hMT+ area of the brain would result in what type of symptoms?
|
Selective loss of motion perception. E.g. pts with this problem can see a car coming at them but then suddenly it's right next to them. Pouring tea into a cup is a problem bc she can see the movement of the filling of the cup.
|
|
|
What would a lesion of FFA cause? What is the technical term?
|
Prosopagnosia - inability to recognize familiar faces. (is this my Fa Fa Amily?)
|
|
|
What happens in V8 lesion? (technial name too)
|
Achromatopsia - loss of color vision due to brain injury.
|
|
|
Damage to V1 would cause what symptoms?
|
COMPLETE BLINDNESS!!!
|
|
|
What happens with lesion in PVA region?
|
Attentional neglect problem.
|