Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
5 Cards in this Set
- Front
- Back

Hx:14yo M child c/o increasing foot deformity Fig A. PE=unable to walk on his heels, < Achilles reflexes b/l. Coleman block testing reveals correctable hindfoot deformity. Which procedure is has improved clinical outcomes in pts w/ the above described condition? 1-Transfer of PB-> PL
2-Split ATT ->to lateral column; -Triple arthrodesis 4-PTT ->through the interosseous membrane to dorsum of the foot; 5-Lateral column lengthening calcaneal osteotomy |

The physical exam and clinical photo are consistent with a cavovarus foot deformity associated with Charcot-Marie-Tooth (CMT) disease. The Coleman block test reveals a flexible hindfoot deformity, which suggests that soft-tissue transfers and not osteotomies can correct the deformity. The posterior tibial tendon retains its strength in CMT and can aid in decreasing hindfoot varus while providing ankle dorsiflexion when transferred to the dorsum of the foot, Answer 1: Peroneal longus to brevis transfer can be utilized due to the fact that PL is typically preserved while PB is weakened in CMT.
Answer 2: The anterior tibial muscle is weakened and therefore transfer provides no benefit and can actually worsen the deformity. Answer 3: Wetmore and Drennan revealed that poor outcomes are associated with triple arthrodesis in CMT. Answer 5: Lateral column lengthening is used in pes planovalgus foot deformities..Ans4 |
|

Hx:22yo F c/o frequent ankle sprains and an awkward gait. LE nerve conduction velocities show prolonged distal latencies in the peroneal nerves. DNA testing shows a duplication on chromosome 17. Which of the images is most likely the xray of this patient? 1- accessory navicular.
2-calcaneonavicular coalition; 3 foot without pathology 4-ball-and-socket ankle, associated with fibular hemimelia;5-high arched foot |
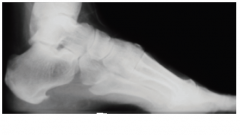
Charcot-Marie-Tooth disease (CMT), or Hereditary Motor Sensory Neuropathy, is a demyelinating disorder of the peripheral nervous system. Manifestations in the foot include pes cavovarus, claw toes, and frequent ankle sprains. The cause of the foot deformities in CMT is an imbalance of distal musculature, with the peroneus brevis and tibialis anterior being relatively overpowered by the peroneus longus.Ans5
|
|

HA:10yo B ED p/injuring his L knee while playing soccer. He localizes the pain to the distal femur, and is unable to bear weight on the affected leg. PE=tender to palpation only directly over the distal femoral physis, swelling about the distal thigh, w/out any signs of knee effusion. xray affected knee Figures A & B. An AP and lateral xray of the contralateral knee are shown in Fig C & D. What is the most appropriate tx? 1-Hinged knee brace w/ early ROM WBAT; 2-LLC w/ close clinical f/u; 3-CR & PP; 4-OR & PP; 5ORIF w/plate
|

The clinical presentation, physical exam, and radiographs are consistent with a Salter-Harris Type I fracture of the distal femoral physis. The radiographs show subtle physeal widening, but no displacement. If there is no displacement following the injury, as in this case, then cast immobilization is acceptable treatment. However, these fractures are associated with a high incidence of deformity so close clinical followup is mandatory. If there is evidence of displacement with a SHI or SHII, then closed reduction percutaneous pinning would be indicated. Open reduction is reserved for SHIII and SHIV fractures, or fractures that can not be reduced.Ans2
|
|

Hx:10yo B falls off his bicycle sustaining the injury FigA and B. After initial unsuccessful CR, he undergoes operative fixation. When comparing ORIF w/ (IMN), which of the following is true? 1- Non-union rates are significantly > in the IMN;
2-Blood loss is >IMN; 3-Restoration of radial bow is similar in both; 4-Surgical time is> IMN; 5- Forearm rotation is > in the ORIF group |
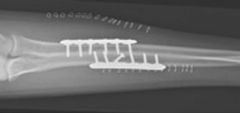
The clinical scenario and radiographs depict a pediatric diaphyseal radius and ulna fracture. Operative indications include open fractures and fractures with unacceptable alignment after closed reduction. The optimal fracture patterns are midshaft pediatric both bone forearm fractures with minimal comminution and acute fractures prior to the presentation of fracture callus. IMN is commonly used for both transverse and oblique patterns. Restoration of radial bow has been shown to be similar with both IMN and ORIF.Ans3
|
|

Hx:12yo B c/o 2yr x hx foot pain that prevent participation in athletic activities and is symptomatic with walking. UCBL and custom made orthoses for 1 year with no relief of sx. His hindfoot is supple and he has full dorsiflexion. Clinical images of the foot are shown in Figures A . A surgical plan to address the deformity would include which of the following? 1-Lat calcaneal slide osteotomy; 2-Transfer of the peroneus longus to the peroneus brevis ;3-1st MT dorsiflexion osteotomy ; 4-Calcaneal neck lengthening osteotomy; 5-PTT transfer to dorsum of the foot
|

clinical presentation is consistent with pediatric flexible pes planovalgus, or flatfoot. The vast majority of these cases are asymptomatic and do not require treatment, and Level 1 evidence shows no benefit with corrective orthotics. In rare situations when nonoperative treatments fail to relieve pain under the head of the talus or in the sinus tarsi, surgery is indicated. A calcaneal lateral column lengthening osteotomy (Evans procedure) is the procedure of choice. Illustration A shows a line depicting the long axis of the talus and a line following the long axis of the 1st metatarsal. The angle between the 2 lines is referred to as Meary's angle and a plantar apex angle of greater than 4 degrees indicates collapse of the longitudinal arch. Illustration B shows an example of a normal Meary's angle and pes planus foot with a Meary's angle of 12 degrees. All of the other options are used in the treatment of pes cavus deformities.Ans4
|