Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
4 Cards in this Set
- Front
- Back

10yo B s/p injury Fig A. Immediate CR was performed in the ER w/ conscious sedation. Post-reduction xrays Fig B post-reduction CT Fig C. What is the next step in management? 1-Repeat CR; 2. Skeletal traction x 1 mth; 3-Hip arthrotomy via post approach; 4-Hip arthrotomy via ant approach; 5- WBAT w/ close f/u and serial xrays
|

post dislocation, post-reduction xrays must be assessed for joint congruity and articular widening. Persistent joint incongruity is likely to be caused by soft tissue interposition consisting of a torn labrum including the lateral acetabular apophysis. A post-reduction CT can be performed to look for interposed bone/osteochondral elements located within the hip joint. Surgical extirpation of osteochondral fragments is warranted.Ans3
|
|

3yo child w/short-limbed dwarfism has the clinical features shown in Fig. A & B. What is the pathoanatomy of this dz? 1-Sulfate transport protein gene mutation affecting cartilage matrix formation; 2-Mutation in the gene CBFA-1 affecting osteocalcin formation; 3-Defect in lysosomal-storage; 4-Defect in lipid-storage; 5-Mutation in gene FGFR-3 resulting in growth plate growth abnormality
|
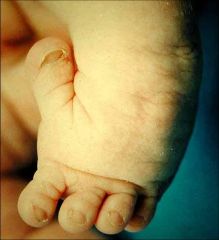
Diastrophic dysplasia is a condition caused by a defect in the SLC26A2 gene, which encodes for a sulfate transporter. The impaired function leads to under-sulfation of proteoglycans in cartilage matrix and abnormalities in the hydraulic properties of cartilage. Multiple cartilaginous structures are affected including the trachea, ear, and ligaments. The pinnae of the ears have a characteristic swelling referred to as cauliflower ear. Neonates can develop tracheomalacia which can be fatal. An abducted hitchhiker thumb and symphalangism (generalized finger stiffness) are both common hand manifestations of this disease. Kyphosis in the c-spine occurs early in life but frequently spontaneously resolves.Ans1
|
|
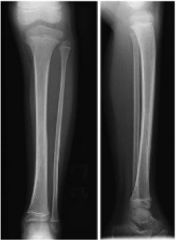
23mo G refuses to WB s/p falling on the playground yesterday, is afebrile WBC (ESR) are w/in nl limits. On PE= leg has no erythema, but does have mild tenderness along the distal tibial shaft. xrays=(-). What is the management? 1. vit D & ca; 2-MRI of the pelvis; 3-LLC; 4-chromosomal analysis; 5-aspiration of the knee
|

toddler's fx, which is treated with a LLC. Initial xray are often (-) but follow-up xray see healing periosteal reaction, one of the MC injuries in the child younger < 2 years. They are non-displaced spiral fx of the tibia caused by low-energy twists and falls. The Tx is application of a LLC x 3-4 wks.Ans3
|
|
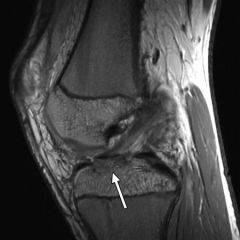
19yo pt is undergoing an arthroscopic tx of a R knee with suture fixation via transosseous tunnels Tibial Eminence Fx. What is the most likely postop complication? 1-Infection; 2-Arthrofibrosis; 3-Spontaneous osteonecrosis of the knee (SONK); 4-Hardware prominence in the intercondylar notch necessitating removal of implants; 5-Increased posterior tibial excursion
|

adolescent or adult patients need to be counseled as to the risk of development of stiffness and arthrofibrotic scar tissue. This often presents with the inability to achieve full knee extension.Ans2
|