Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
29 Cards in this Set
- Front
- Back
|
Within the germinal center there are two types of B cells
|

centroblasts- actively dividing- in the dark zone
centrocytes- resting B cell- in the light zone |
|
|
What is the general life cycle happening with the b cells in the germinal center?
|
the centroblasts divide and then go to the light zone to rest, but they must then receive signal 1 then 2 or they enter programmed death
|
|
|
How is somatic hypermutation happening?
|
In the dark zone the centroblasts shed their receptors (don't want to have a mix) and using the AID enzymes do the point mutations. At a certain point they stop dividing and turn into centrocyte and express their new receptors. In the light zone they compete for the Ag- they only have ~20 hours to get it before they apoptose.
As time goes on- 8 weeks later- and Ag is low in supply, it gets very competitive and a cell must have very strong affinity to survive |
|
|
What kinds of things happen in germinal center to cause class switching?
|
during the second week after some of the somatic hypermutation has already been going on, some of the higher affinity cells will take in the Ag, process it, and get cognate with helper t cell for signal 2. They can shed receptors and go back to centroblast OR they can class switch instead.
When centrocyte expresses AID does class switching- VDJ moved near other Ig isotype. |
|
|
How is class switching regulated?
|
The helper cells make different cytokines combinations over time and it causes different isotypes to come out from the Ig A G E. (Ig3 then 1 2 and 4 in that order which is just down the chromosome actually)
|
|
|
Plasma cells in the blood indicates what?
|
you have a very sick pt- a myeloma. They're supposed to be in the bone marrow.
|
|
|
After the somatic hypermutation and class switching, what's another fate the centrocyte may have?
|
become a Memory B cell. The receptors/Ab they have will be whatever isotype they had from class switching. These are regulated the same for if they're receptor or Ab form. These home onto secondary lymphoid tissues throughout the body
|
|
|
What happens during congenital deficiency of CD40L?
|
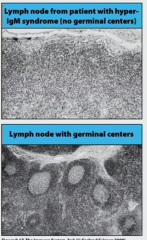
hyper-IgM syndrome
you can't get second signal from helper T cells, so no affinity maturation, isotype switching, or memory cell generation (all these steps need signal 2 feedback for centrocyte) |
|
|
What are plasma cells like?
|
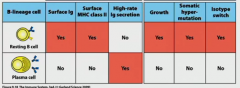
they are Ab factory and they don't do anything else. They are terminally differentiated.
|
|
|
So, what's the big difference between TD and TI antigen responses?
|
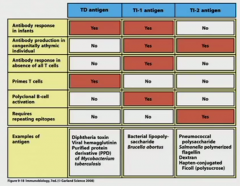
in both you need signal 1 and 2, but only in TD can you go from parafollicular response to germinal center response for the affinity maturation, isotype switching, and memory cells
|
|
|
Which Ig isotypes do you find where?
|
Lots of IgG in blood and body
Lots of IgA monomeric in blood and body Lots of IgA dimeric in mucousal surfaces (so if you ever sample these surfaces there should be a bunch- they have a problem it's all IgM) IgM in blood IgE on basophils and mast cells right below epitheliod barriers-- was for parasites, but now just allergies |
|
|
What Ab's go across placenta?
|
All subtypes of IgG though these are passive transfer so only last a while
|
|
|
What Ab's can go through breast milk?
|
IgA dimeric-- so definitely recommend
|
|
|
The endothelial cell receptor, ___, transports Ig_ from the bloodstream into extracellular spaces.
It's also what does.. ? |
FcRn puts out IgG
puts IgG across the placenta- that's why only IgG's go across-- this FcRn |
|
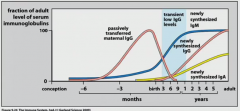
what is missing in the diagram?
|
IgA coming across in the breast milk
|
|
|
Every once in a while maternal Ab interfere with ..
|
vaccines because maternal Ab's address- especially live attenuated viral vaccines
|
|
|
Along your epitheliod barrier you have your immune responses which drive germinal centers to make Ig_ and Ig_ plasma cells.
|
IgA and IgM
|
|
|
Which form of IgA are made in the sub epitheliod barrier areas?
|
the dimeric version because it has to be dimeric form to interact with the poly-Ig receptor (PIG receptor). That's how you get transcytosis of IgA. IgM, remember, makes pentamers all the time nbd.
|
|
|
the IgA is modified as it gets transcytosed- what is that about?
|
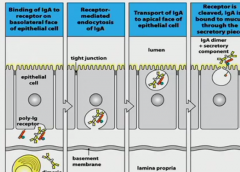
when it interacts with the PIG R it actually gets attached to it. In order to release there's a cleavage event except that it leaves a fragment of the PIG R to the IgA and they call that the secretory component- that piece is important because it protects the Ab from cleavage of digestive enzymes
|
|
|
What is one of the main jobs of IgA on the mucousal surface? (this happens in the body too though)
|

virus neutralization. Viruses have trophism (attaching to our cells, like HIV for CD4). If they can't bind like during neutralization, the virus can't work.
If a bacteria binds, it colonizes which is bad. |
|
|
What are toxins (as far as we're concerned now)?
|
small lightweight protein that moves away from site of infection and wreaks havoc doing bad things-- because it leaves, it's really difficult to make Ab to this. So vaccines are really really helpful for these (tetanus and diphtheria)
|
|
|
IgM has low affinity for complement but they're good at fixing it
|
because as a pentamer they have good avidity
|
|
|
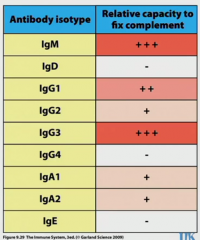
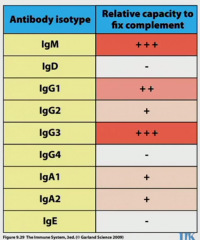
Different Ab isotypes and how they fix complement
what's another affinity they have that varies in this same pattern? how does affinity maturation vary? |
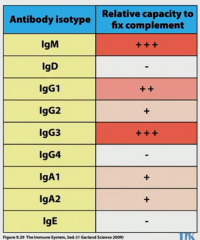
order of expression: IgM, IgG3, IgG1, IgG2, IgG4
highest complement to lowest: same order gene order on chromosome: same order affinity for Fc gamma to facilitate phagocytosis: same order for IgG's there are more somatic hypermutation rates as you go down the list so IgG3 has much less change than IgG4 |
|
|
So comparatively IgG2 and IgG4 have the best affinity but don't do anything good when it comes to inflammation- why do we bother with these isotypes?
|
inflammation can be really damaging, so it needs to be turned off at some point. These aren't giving B cells the signal 2 and IgG4 actually sends a signal through FcR to turn off signal 1 in b cell
|
|
What about IgA- why is it so weak at inflammation?
|
do u want your guts inflamed? You don't want these to be really sensitive because you have so much bacteria in your gut
|
|

why for IgG3?
|
IgG3 has the weakest affinity, but the super flexible hinge means avidity is not so bad but these are turned over quickly because the long hinge can be targeted?
|
|
|
Fc receptors are pretty useful for stuff like
|
innate cells phagocytose opsonized materials (IgG3 IgG1)
|
|
|
NK- how do they work?
|
IgG goes through CD16 FCgamma RIII
IgA goes through CD89 FCalpha RI if this happens they release cytotoxins to target cell ADDC antibody-dependent cell-mediated cytotoxicity |
|
|
What's IgE doing?
|
on mast cells using Fc epsilon RI. When they have something cross-link across, mast cell activated. Supposed to be for parasites, but domestically we have more problems with pollen or mite feces
|