Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
27 Cards in this Set
- Front
- Back
|
Sporotrichosis transmission/infection and demographic
|
cuts or lesions on hands or arms is most common from soil, tree bark, garden plants and frequent in male gardeners, farmers in Mexico, Brazil, Uruguary, S. Africa
|
|
|
Sporotrichosis post infection presentation
|

papules as site of infection, spreads through lymphatics, will eventually manifest as (lymphocutaneous) lesions on the skin that follow lymphatics pattern
|
|
|
Sporotrichosis causative agent
|
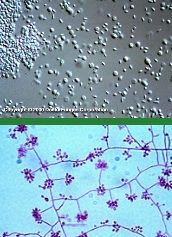
Sporothrix schenkii, thermally dimorphic w/ 37C - round yeast, 25C septate hyphae, rosette shaped clusters of conidia at tips of conidiophores
|
|
|
Sporotrichosis Dx
|
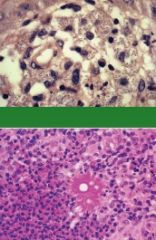
Microscopy of pus or sputum, *Asteroid bodies in histo biopsy within yeast cells and Splendore-Hoeppli, culture, serology
|
|
|
Sporotrichosis Tx
|
spontaneous, topical/oral (potassium iodide)
|
|
|
Sporotrichosis rare presentation
|
pulmonary, osteoarticular, disseminated
|
|
|
Chromoblastomycosis transmission/infection and demographic
|
Caused by trauma (splinters, thorns), in men in tropical/subtropical regions, affecting extremities
|
|
|
Chromoblastomycosis rare presentation
|
systemic
|
|
|
Chromoblastomycosis post infection presentation
|

1)cauliflower nodular lesions
2)plaques, central healiing with atrophic yellow scar tissue |
|
|
Chromoblastomycosis causative agent
|
Fonsecaea (F. pedrosoi), Cladosporium (C. carrionii)
|
|
|
Chromoblastomycosis Dx
|
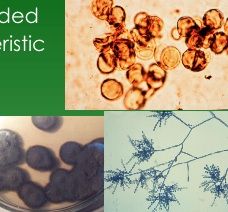
KOH microscopy with sclerotic cells/bodies, velvety culture
|
|
|
Chromoblastomycosis Tx
|
antifungal tx, surgery, cryosurgery
|
|
|
Mycetoma transmission/infection and demographic
|
trauma infection of trunk, feet usually from walking barefoot, mainly in men of subcutaneous tissue and bone, more frequent in tropical and subtropical climates
|
|
|
Mycetoma post infection presentation
|

painless swelling, thickening of skin -> enlarge to become tumorous -> discharge viscous fluid containing GRAINS
|
|
|
Mycetoma causative agents
|
40% Eumycetoma (Pseudodallescheria boydii (US), Madurella mycetomatis (WW)), Actinomyces
|
|
|
Mycetoma Dx
|
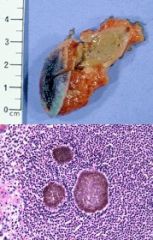
Clinical triad: tumefaction, draining sinuses, granules. Granules are the most significant
|
|
|
Mycetoma Tx
|
Surgical antifungal combo, 80% recurrance with surgery
|
|
|
Mycetoma rare presentation
|
can spread to bone, muscle, blood vessels
|
|
|
Phaeohypomycosis transmission/infection and demographic
|
saprophytes cause infection, presents on hands and feet, sometimes looks like a synovial cyst, firm or fluctuant to touch, painless
|
|
|
Phaeohypomycosis post infection presentation
|

cyst, can spread to face and trunk, hyperpigmented demarcated plaques
|
|
|
Phaeohypomycosis causative agent
|
over 20 saprophytes, but remember Exophilia jeanselmei and Wangiella dermtitidis
|
|
|
Phaeohypomycosis Dx
|

Microscopy w/ brown pigmented, branching septate hyphae and dark walled yeast, histo with hyphae with giant cells
|
|
|
Phaeohypomycosis Tx
|
surgical, antifungal
|
|
|
Zygomycosis transmission/infection and demographic
|
traumatic implantation
|
|
|
Zygomycosis causative agent
|

C. coronatus in males' nasal submucosa; B. ranarum in male children's limbs, trunk
|
|
|
Zygomycosis Dx
|
Biopsy, so histo necessary: focal clusters of inflammation eosinophils and zygomycotic hyphae - Splendore-Hoeppli phenomenon
|
|
|
Zygomycosis Tx
|
Surgery, anti-fungal (itraconazole, oral potassium iodide)
|