Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
77 Cards in this Set
- Front
- Back
|
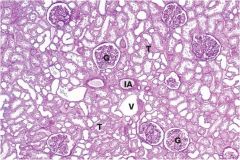
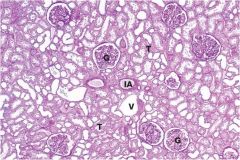
thick tubules are probbaly more proximle bc of brush border (left side of pic)
note how tubules are back to back; this is good; as you get disease they start to drop out and get farther apart |
|
|
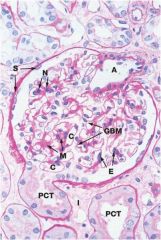
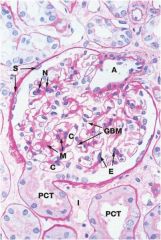
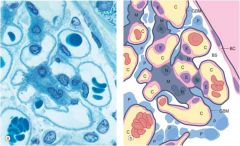
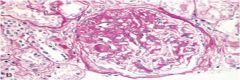
mesangium; produce basement membrane matrix; support glomeruli;
podocytes are on the outside of the loops notice symmetry; no fibrous deposits on one side vs the other not cellularity, not a lot of touching between nuclei (if they were = hypercellular) endothelial cells =inside of capillary loop podocytes = outside of capillary loop |
|
|
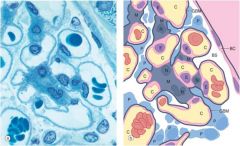
mesangium = meso = middle, angium = blood vessels => supports blood vessels
endothelial cells inside vessel podocyte cells outside vessel loops |
|

|

spikey parts = podocytes
mesangium next to capillary lumen which has blood cells in it |
|

two layers of basement membrane = lamina rare externa/interna
|
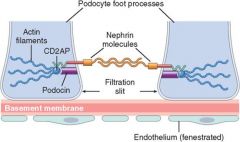
glomerular slit diaphragm: deficiencies in nephrin or podocin = proteinuria bc these compounds are very important for holding back protein
|
|
|
Non-collagenous disease
|
IgG anti-NC1, which is a component of the basement membrane collagen
|
|
|
azotemia
|
accumulation of nitrogenous wastes
|
|
|
increased BUN in GI bleeding
|
rbc breakdown in gi tract
|
|
|
increased BUN in increased protein intake
|
protein breakdown in gi tract
|
|
|
creatinine laboratory evaluation
|
not much creatinine secreted into tubules (10%);
you can lose alot of kidney function 50-60% and still have normal creatinine |
|
|
BUN/Creatinine ratio
|
10/1 Normal
|
|
|
BUN:Cr >= 20:1
|
Pre-renal azotemia likely; sluggish flow of circulation around tubules allows for more BUN resorption
Tubular secretion of creatinine persists blunting the marked rise serum creatinine (stone, clot, stenosis, low blood pressure) |
|
|
BUN: Cr = 10:1
|
Something wrong in kidney because nothings working right so both BUN:Cr are not being reabsorbed preferentially
|
|
|
BUN:Cr > 20:1
|
early phase BUN:Cr 20:1 in early phase urea absorbed from sluggish urine flow
Later phase BUN:Cr approximately 10:1, pressure from backup of urine can damage kidneys This will then result in intrinsic disease |
|
|
foamy urine
|
protein
|
|
|
upper limit of 24 hour protein excretion in normal adults
|
150mg
|
|
|
which proteins are dipstick sensitive too
|
only albumin; wont be sensitive to other proteins (benz-jones proteins for ex)
|
|

|
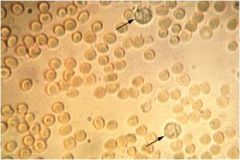
dysmorphic rbc; rbc going through diseased kidneys
|
|
|
Hematuria; intact rbc; indicates bleeding in kidney since it is not a rbc cast
|
|
|
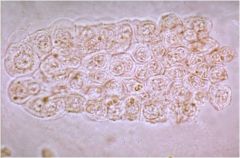
tubular cell cast; indicative of tubular casts
|
|
|
granular cell casts; indicative of tubular diseaes
|
|

|
uric acid crystals
|
|
|
cystine crystals
|
|
|
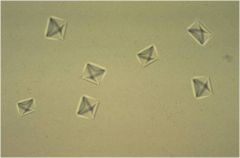
oxylate crystals; look like envelopes
|
|
|
why cant you just look at urine volume to evaluate kidneys
|
GFR-reabsorption = urine volume
BUT both could be low and thus still urinating normal volumes |
|
|
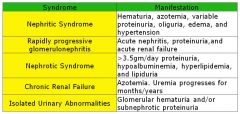
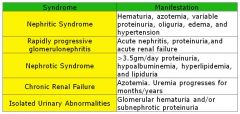
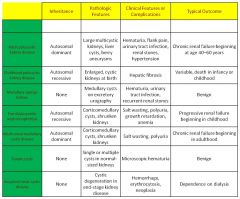
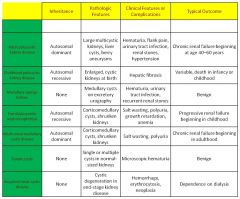
Memorize this chart
|
|

|

a. global
b. segmental c. diffuse focal/mesangial |
|
|
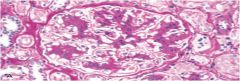
poststreptococcal glomerular nephritis; big hump is pathonomonic
|
|
Type I RPGN
|
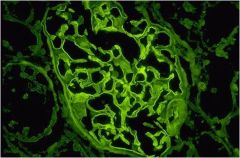
antiglomerular basement membrane antibody; linear deposition (IgG +/- C3); can go to lung and cause pulmonary hemorrhage
Goodpasture antigen = noncallagenous portion of the alpha 3 chain of type IV collagen |
|
Type I RPGN
|
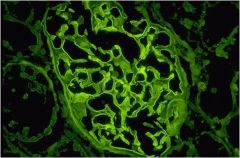
antiglomerular basement membrane antibody; linear deposition (IgG +/- C3); can go to lung and cause pulmonary hemorrhage
Goodpasture antigen = noncallagenous portion of the alpha 3 chain of type IV collagen |
|
|
Type IIII RPGN
|
Pauci-immune
c-ANCA: Wegners (cytoplasmic staining) p-ANCA: polyangitis ANCA may direct against the MPO and PR3 |
|
|
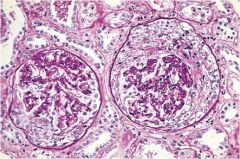
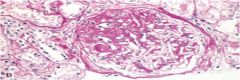
Crescents in RPGN; parietal epithelial cells proliferate and squeeze off glomerulus
fibrin proteins when spilled out into bowmans capsule promotes proliferation of parietal cells |
|
|
mc systemic causes of nephrotic syndrome
|
diabetes, amyloidosis, SLE
|
|
|
Spike and dome
|
membranouS Spikes (membranous nephropathy)
IC deposit between podocytes; BM grows around it = spikes |
|
|
minimal change diease (lipod nephrosis)
|

normal glomeruli on EM + nephrotic syndrome
effacement of foot processes |
|
|
focal segmental glomerulosclerosis
|
|
|
Type I MPGN
|
localization in glomerulus activates complment/alternative pathway
|
|
|
Type II MPGN
|
decreased levels of C3 w/ normal C4 (bc it snot involved in the classic)
|
|
|
Membrano proliferative glomerulonephritis
|
subendothelial IC with granular IF
basement membrane laid on top of IC deposits; IC deposition = granular |
|

|
Left: Type I: Subendothelial deposits, tram tracking
Right: Type II: Ribbon like deposits of electron dense material |
|
|
Where does IgA deposit
|
Mesangium
IgA nephropathy |
|
|
Henoch-Schonlein Purpura
|
vascular disease that results from immunological damage to the blood vessel walls
|
|
|
differentiate henoch-schonlein purpura from IgA nephropathy
|
HSP = lesions on butt + abdominal pain/vomiting, IgA affecting vessels in GI tract
|
|
|
diabetic nephropathy pathogenesis
|
NEG of GBM/capillary basement membrane -> increased permeability/thickening
|
|
|
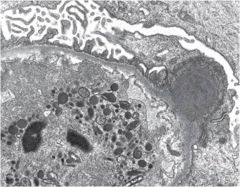
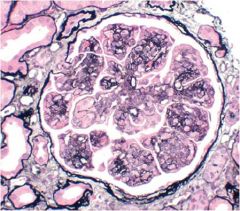
Kimmelstiel-Wilson Disease/DNP
|
nofdulcar glomerular sclerosis; one of the ways in which diabetes will affect the kidneys; large balls of PAS positive material (christmas tree dz)
|
|

|
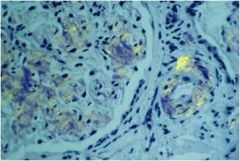
Amyloidosis
giant tongue |
|
|
maybe add a line for how they look grossly
|
|
|
|
|
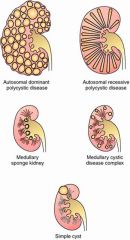
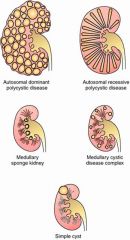
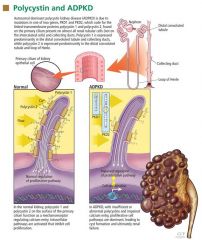
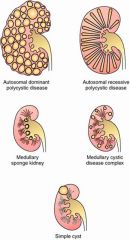
autosomal dominant (adult polycystic disease
|
expand out and affect entire functioning
mutation in ADPKD and PKD1/2 gene lack of calcium signal causes abnormal growth signaling = cellular proliferation, apoptosis, interactions w ECM and secretory function of the epithelia keep building cells around a tube |
|
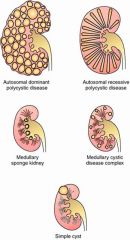
autosomal recessive polycystic kidney disease; radial dilitation of collecting ducts
|

also associated w biliary dsgenesis and portal tract fibrosis
gene mutation = PKHD1 gene -> messed up protein fibrocystin its on chromosome 6 |
|
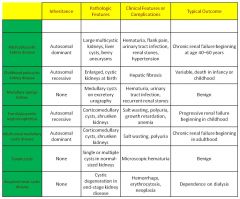
nephrononphthisis; type of medullary cystic disease
|
ar and ends in ESRD within the first 3 decades of life; consider this is young kids
|
|
medullary cystic kidney disease vs nephronopthisis
|

know nephronophthisis NPH1-6 gene mutations
MCKD1 and MCDK2 in medullary cystic disease |
|
|
mckd location
|

hug corticomedullary region
|
|
medullary sponge kidney
|
dilated medulary and papillary collecting ducts which result in the medulla having a sponge like appearance; occur at tips of pyramids
|
|
|
acquired (dialysis associated) cystic disease
|
chronic renal failure (dialysis) associated with the development of renal cysts in cortex or medulla (seen anywhere)
renal cancer (seen in 7% of dialyzed pts seen for 10 yrs) |
|

simple cysts
|
usually on cortex; translucent; smooth membrane; most asymptomatic
|
|

urinary tract obstruction
|
can occur anywhere
dysfunction in concentrating ability if you get to tubules; obstruction can eventually cause interstitial inflammation -> fibrosis, GFR may decline |
|

complications
|
infection (stasis), stone formation, permanent renal atrophy
acute obstruction = renal colick |
|

urolithiasis
|
increased conc. beyond soluility = precipitates = stones
|
|
|
ammonium magnesium phosphate
|

2nd mcc kidney stone; infection w urease-positive bugs (proteus vulgaris, staph, klebsiela); can form staghorn calculus
|
|
|
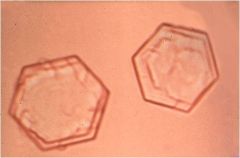
cystine stones
|
most often 2 to cystinuria; hexagonal shape. Rarely, may form cystine staghorn calculi
associated w genetic defects (cystinuria) faintly radiopaque; tx w alkalnization of urine |
|
|
urolithiasis
|
can lead to severe complications such as hydronephoriss and pyelonephritis; tx and prevent by encouraging fluid intake
|
|
|
ureterovesciular junction stone pain radiation
|
urinary uregency and frequency
|
|
|
stone in lower part of ureter
|
radiate to ipsilateral testicle and labium in women
|
|
|
stone in upper part of ureter
|
anterior radiation
|
|
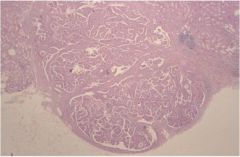
renal papillary adenoma (lots of little papilla; seen histologically as little islands)
|
cortical tumors arising from the renal TUBULAR epithelium
histologically they are indistinguishable from low grade papillary renal cell adenocarcinoma |
|
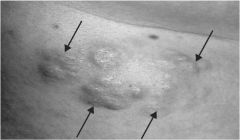
skin manifestations of tuberous sclerosis
|

shagreen patches in the lumbosacral region of patient + angiofibromas around nose + ash leaf macules (hypopigmentations) in a patient with tubule sclerosis
|
|
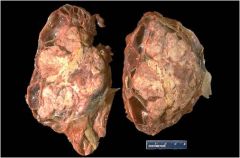
oncocytoma
|
mahogany brown surface
note large eosinophilic cells |
|
|
von hippel lindau syndrome association (VHL gene at 3p25)
|
AD syndrome w renal cell carcinoma association
also cerebellar hemangioblastoma retinal angiomas pheochromocytoma cysts in various organs |
|
|
VHL gene location
|
3p25; its a tummor supressor gene
|
|
|
variants of renal cell carcinoma
|
clear cell carcinoma
papillary carcinoma |
|
|
clear cell carcinoma
|
70-80% of RCC; many demonstrate loss of sequence on chromosome 3 (3p25); loss of VHL/tumor supressor gene
|
|
|
papillary carcinoma
|
Sporadic form (Trisomies 7, 16, 17)
Familia form (Trisomy 7) - chromosome 7 which encompasses the MET proto-oncogene |
|
|
chromophobe rcc prognosis
|
excellent prognosis
|
|

|
know this chart
|
|

|
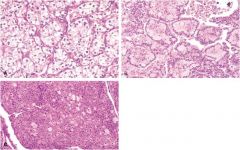
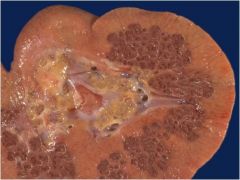
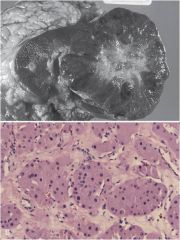
renal cell carcinoma; towards the top/pole of kidney; yellow = lots of lipids
a. clear cell type b. papillary type c chromophone |
|
|
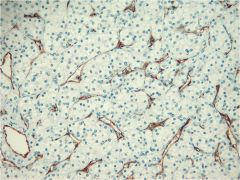
note lots of blood vessels in rcc
|