![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
140 Cards in this Set
- Front
- Back
|
What is pulse pressure? |
Difference between systolic and diastolic pressure |
|
|
What is mean arterial blood pressure? What is the formula? |
Average pressure in arterial system during ventricular contraction and relaxation. MABP = CO x VR (vascular resistance) |
|
|
What is Cardiac Output (CO)? |
HR x SV |
|
|
What are the autonomic systems for regulation of BP? |
- Baroreceptors (in carotid arteries) - Chemoreceptors |
|
|
What are the hormonal systems for regulation of BP? |
- RAAS (renin, angiotension, aldosterone system) - Anti Diuretic Hormone (ADH) - Arenaline |
|
|
If BP is 120/80, how would this be classified? |
Normal |
|
|
If BP is 130/85, how would this be classified? |
Prehypertensive. 120-139/80-89 is classified as prehypertensive |
|
|
What BP is determined to be hypertensive? |
140+/90+ |
|
|
What is the target BP for someone with diabetes mellitus? |
130/80 |
|
|
What is the difference between primary, secondary or malignant hypertension? |
Primary is a chronic elevation in BP without evidence of other disease. Secondary occurs as a result of another disease. Malignant is an accelerated form |
|
|
If only systolic or diastolic pressure is elevated, what is this called? |
Systolic or Diastolic hypertension |
|
|
What is the BP of a newborn? How does this change throughout life? |
BP of a newborn is approx 50/40. Progressively increases until end of adolescence when systolic pressure reached 120. Diastolic pressure continues to rise until approx 60yo then declines |
|
|
Which race is most susceptible to hypertension? |
African Americans and indiginous Australians |
|
|
What are some lifestyle factors that contribute to hypertension? |
- high salt intake - obesity - alcohol consumption - contraceptive drugs - stress - potassium, calcium and magnesium intake |
|
|
What are some clinical manifestations of hypertension? |
- waking headaches, with nausea and vomiting - nose bleeds - bruits (audible turbulence in blood flow) - blurred vision - confusion - fatigue - dizziness, unsteadiness in gait |
|
|
How is hypertension treated? |
Modification of lifestyle factors (e.g. weight loss, reduce salt intake, stop smoking, etc) Drugs - diuretics - vasodilators - beta blockers - ace inhibitors - etc. |
|
|
What are some causes of secondary hypertension? |
- illicit drugs - kidney disease - adrenal cortical disorders - sleep apnoea |
|
|
Who is most susceptible to malignant hypertension? |
- young people, particularly african american males - women with toxaemia of pregnancy |
|
|
Why are kidney disorders associated with hypertension? |
Most kidney disorders cause decreased urine formation, resulting in higher salt and water retention. This results in a higher volume of blood and therefore hypertension |
|
|
What is malignant hypertension. |
An accelerated form of hypertension. There is a sudden, significant increase in BP with other life-threatening organ dysfunction. |
|
|
What are the 3 types of hypertension in pregnancy? Briefly describe each.
|
Gestational - rise in BP during pregnancy without proteinuria Preeclampsia/eclampsia - rise in BP during pregnancy with proteinuria Chronic - Hypertension before and after pregnancy |
|
|
What is hypertension treated in pregnancy? |
- early prenatal care - refraining from drinking or smoking - reduced salt intake - careful chosen antihypertensive meds |
|
|
What are the usual causes of hypertension in infants? |
- high umbilical catheterisation and renal artery thrombosis |
|
|
What is orthostatic hypotension? |
- an abormal drop in BP that occurs when patient stands |
|
|
What are likely causes of orthostatic hypotension? |
- decrease in venous return to the heart (can be due to blood pooling in lower body) - inadequate cardiac output - anything that reduces blood volume, e.g. dehydration, diuretics, excessive vomiting/diarrhea) - impaired mobility / bed rest |
|
|
What are some complaints associated with orthostatic hypotension? |
- dizziness - visual changes - head/neck discomfort - unable to concentrate while standing - presyncope/syncope (feeling faint/fainting) |
|
|
What is it called when there are elevated levels of any kind of lipids? (triglycerides, phosopholipids, cholesterol, etc) |
Hyperlipidemia |
|
|
What is hypercholesterolemia? |
Elevated levels of cholesterol in the blood.
Above 240mg/dL |
|
|
What is hypercholesterolemia a major risk factor for? |
Artherosclerosis |
|
|
How is hypercholesterolemia managed? |
- reduced fat intake (particularly saturated and trans) - exercise + weight reduction - quitting smoking - lipid/cholesterol lowering drugs |
|
|
Briefly describe artherosclerosis |
The formation of fibrous fatty lesions in the internal lining of blood vessels |
|
|
What is the typical steps to artherosclerosis formation changing vessel structure? |
1. Vessel endothelium damaged (chemical irritants, haemodynamic stress, etc) 2. LDL and VLDL infiltrate and lodge in vessel wall, leading to further dysfunction and inflammation 3. Causes WBC to migrate to area 4. Fibrous cap develops |
|
|
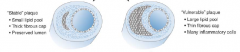
What is the difference between a stable and unstable artherosclerotic plaque? |
|
|
|
What complications of artherosclerosis are more likely to occur on larger vessels? |
Thrombus formation and weakening of vessel wall |
|
|
What complications of artherosclerosis are more likely to occur in medium sized vessels? |
Ischaemia, leading to hypoxia and infarction |
|
|
Which arteries are most commonly effected by artherosclerosis? |
Arteries supplying heart, brain, kidneys, lower extremities and small intestine |
|
|
What are the major risk factors for artherosclerosis? |
- hypercholesterolemia (and low HDL cholesterol) - smoking - hypertension - obesity - diabetes - family history of heart disease - age |
|
|
What is the manifestation of artherosclerosis? |
- Loss of peripheral pulse - Limb ischaemia (pain, cramping, sensory and motor weakness) - pale skin or cyanosis (blue skin due to poor circulation) - necrosis - angina |
|
|
What are the major complications of artherosclerosis? |
- Hypertension - Stroke - Embolism - ischemic heart disease - heart attack - peripheral vascular disease - erectile dysfunction |
|
|
How is artherosclerosis treated? |
- reduce risk factors (fatty foods, smoking, hypertension, weight loss, sedentary lifestyle) |
|
|
Broadly speaking, what is peripheral vascular disease? |
Any disorder of circulation in the extremities |
|
|
What is vasculitis? |
An inflammatory immune response directed against the vessel wall |
|
|
What are the manifestations of vasculitis? |
- fever - myalgia (muscle pain) - arthralgia (joint pain) - malaise |
|
|
What is an acute arterial occlusion, and what's the usual cause? |
A sudden event that occludes an artery. Usually caused by thromus or embolus |
|
|
What are the manifesations of acute arterial occlusion? |
The 7 P's - Pistolshot (acute onset) - Pallor (pale skin) or cyanosis (blue skin) - Polar (cold) - Pulselessness - Pain - Parasthesia - Paralysis |
|
|
Where is artherosclerotic occlusive disease most common? |
Vessels of lower extremities (e.g. femoral/popliteal arteries). Risk factors same as artherosclerosis. |
|
|
What is thromboangitis obliterans? |
Inflammatory arterial disorder causing thrombus formation |
|
|
Which type of arteries are most commonly affected by thromboangitis obliterans? |
Medium size arteries
(e.g. vessels in foot/lower leg and arm.) |
|
|
What is raynaud disease? |
A disorder affecting small arteries and arterioles (usually fingers and toes). Causes a vasospasm in response to cold (significant constriction) resulting in pallor and cyanosis |
|
|
What is an aneurysm? |
An abnormal, localised dilation of a blood vessel |
|
|
What is a berry aneurysm? Where are these most often found? |
Small, spherical vessel dilation. Often effects the circle of willis |
|
|
What is a fusiform/saccular aneurysm and where are they most often found? |
Gradual enlargement of the aorta. Usually found in thoracic and abdominal aorta |
|
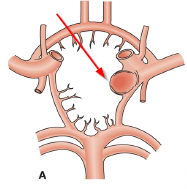
Label this structure |
Berry aneurysm, in the circle of willis |
|
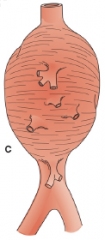
What is this an example of? |
Aneurysm of abdominal aorta |
|
|
What is a dissecting aneurysm? |
When the inner layer of the blood vessel tears, blood haemorrhages in between the vessel walls. This is an acute, life threatening condition. |
|
|
What are the manifesations of a dissecting aneurysm? |
- Abrupt, excruciating pain, described as 'tearing' or 'ripping' - elevation of BP (initial stages) - drop in BP (later stages) - syncope (loss of consciousness due to low BP) - Hemiplegia or paralysis - heart failure |
|
|
What are the manifestations of an aneurysm? |
Variable, depending on location. Thoracic aneurysm may cause pain around sternum, back and neck as well as breathing difficultes Abdominal may cause abdominal/low back pain |
|
|
What are varicose veins? |
Abnormaly twisted, lengthened and dilated superficial veins on lower legs, which often appear raised |
|
|
What are the most common causes of varicose veins? |
- venous valve dysfunction/incomptence - venous wall dilation - believed to be genetic link |
|
|
What is venous insufficiency? |
When blood flow in the veins is no longer unidirectional due to inability of valves to completely close. |
|
|
What is thrombophlebitis? What is the most common form? |
The formation of a thrombus in a vein with inflammation. Deep vein thrombosis is a common form |
|
|
What is a complication of thrombophlebitis? |
Pulmonary embolism |
|
|
What are risk factors for thrombophlebitis? |
- Venous stasis (prolonged bed rest, immobilisation, etc) - Vessel trauma - Blood coagulation |
|
|
What are the signs and symptoms of thrombophlebitis? |
- Usually asymptomatic until embolism moves elsewhere, but may be inflammatory symptoms depending on location (femoral vein thrombosis causes pain in distal thigh and popliteal) - Pain, swelling, tenderness - fever - malaise |
|
|
How is thrombophlebitis treated? |
- Elevation of legs to prevent stasis - Heat - Legs extended - Gradual ambulation - anticoagulations |
|
|
What is the general description of an ischaemic heart disease? |
When an imbalance between myocardial oxygen demand and supply occurs. |
|
|
What is often the cause of ischaemic heart disease? |
Occlusion to the coronary circulation |
|
|
What is another name for ischaemic heart disease? |
Coronary heart disease |
|
|
What is chronic ischaemic heart disease? |
Chronic IHD is recurrent episodes of myocardial ischaemia. |
|
|
What is Angina Pectoris? What is the usual cause? |
Chest pain due to ischemia of heart muscle |
|
|
What is the manifestation of angina pectoris? |
- Constricting/squeezing pain in the chest/substernal area. - pain may radiate to arms, jaw and thorax - usually relieved by rest |
|
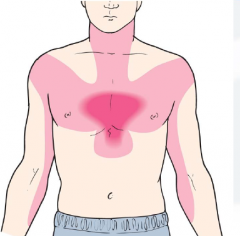
This pain map could indicate what? |
Angina Pectoris |
|
|
What is the most common cause of Angina Pectoris? |
Angina is caused by occlusion to coronary arteries. Usually as a result of artherosclerosis |
|
|
What is the difference between a stable and unstable lesion? |
Unstable lesions can rupture and cause thrombus formation and platelet adhesion. |
|
|
In stable angina, chest discomfort is predictable during exertion or emotional stress. Why is this? |
In stable angina, the artery occluded may still allow enough blood flow to satisfy the oxygen demands at rest. However, with increasingly demanding activities, supply will be insufficient.
This is why pain usually occurs during exertion. |
|
|
What are the manifestations of stable angina? |
- Discomfort/Pressure/Tightness/Burning/Heaviness in the chest. - Rarely lasts more than 5-10 minutes (eases with rest) - Increases HR (tachycardia) - Excess sweating (diaphoresis) - breathing difficulties (dyspnoea) - nausea - fatigue and weakness |
|
|
What are the 3 phases of unstable angina? |
- Artherosclerotic plaque disruption - Platelet aggregation - Secondary haemostasis |
|
|
What are some manifestations of unstable angina? |
- Progressively worse angina attacks - sudden onset angina at rest - attacks lasting 20+ minutes - myocardial infarction |
|
|
What is another term for an acute myocardial infarction? |
Heart attack |
|
|
What is the difference between an acute myocardial ischaemia and acute myocardial infarction? |
Infarction is necrosis (cell death) as a result of ischemia. If the ischemia is severe enough, infarction will result |
|
|
What are some risk factors for acute myocardial infarction? |
- cardiovascular disease - Hypertension - smoking - high cholesterol - obesity - drug/alcohol abuse - stress - age |
|
|
In terms of occlusion, what is the difference between a NSTEMI (non ST-elevation myocardial infarction) and a STEMI? |
NSTEMI is caused by a PARTIAL occlusion. Only part of the heart muscle supplied by occluded artery dies STEMI is caused by a COMPLETE occlusion. Practically all muscle supplied by occluded artery dies. |
|
|
How can you determine is a cardiac event is an unstable angina or an NSTEMI? |
- test for presence of cardiac enzymes |
|
|
In terms of ECG, what are the major differences between a STEMI and NSTEMI? |
1. During the acute phase, there is a marked elevation of the ST segment in a STEMI. In a NSTEMI there may be a t-wave inversion or ST depression 2. In a STEMI, the Q wave becomes deeper and the R wave is reduced following the acute event. |
|
|
What are the manifestations of myocardial infarction? |
- Sudden onset - Severe, crushing pain. Usually substernal and may radiate to left arm, neck and jaw - Nausea + Vomiting - Fatigue and Weakness - Tachycardia, anxiety, restlessness. - Feeling of doom - Pallor (pale, cool skin) |
|
|
What are the complications of MI (6)? |
- Embolism - Cardiogenic shock - Arrythmia - Pericarditis - Cardiac tamponade - Congestive heart failure |
|
|
What factors determine the extent of infarction? |
- Location + extent of occlusion - Amount of heart tissue supplied by vessel - Duration of occlusion - Metabolic need of the tissue - Extent of collateral circulation - HR, BP and cardiac rhythm |
|
|
What is the difference between a transmural and subendocardial infact? |
Transmural - involves full thickness of ventricular wall Subendocardial - involves only inner part of ventricular wall (1/3 - 1/2) |
|
|
What are some methods of diagnosing ischemic heart disease? |
- History - ECG - Stress Testing - Standard exercise testing - Imaging techniques (echo/angiogram/nuclear imaging) |
|
|
How is ischemic heart disease treated? |
- medication - revascularisation (e.g surgery) - quit smoking - reduce stress - reduce BP - lose weight (if over) - reduce fatty (particularly cholesterol) foods |
|
|
What types of surgical interventions can be used for ischaemic disease (revascularisation)? |
- Coronary Artery Bypass Grafting (CABG)
- Percutaneous Coronary Intervention (PCI) - Stents - Atherectomy (removal of plaque with catheter) |
|
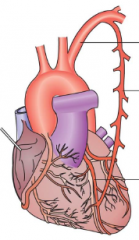
This image is an example of what? |
A coronary artery bypass graft, using the internal mammary artery (branching off left subclavian) |
|
|
What is a cardiomyopathy? |
A disease of the myocardium associated with mechanical or electrical dysfunction
|
|
|
What are the 3 types of cardiomyopathies? |
- Dilated (enlargement of ventricular chamber) - Hypertrophic (abnormal thickening of left ventricular wall) - Restrictive - (stiffening of myocardium) |
|
|
In a dilated cardiomyopathy, is ventricular contractility reduced or enhanced? |
Ventricular contractility is reduced. In dilated cardiomyopathy, the ventricular wall thickness is reduced thereby reducing muscle content and therfore contractility |
|
|
What are the manifestations of dilated cardiomyopathy? |
- Low cardiac output - fatigue, lightheadedness - dyspnoea - low BP - venous congestion - oedema |
|
|
What is hypertrophic cardiomyopathy? |
Abnormal thickening of left ventricular wall and septum |
|
|
What is the most common cause of sudden cardiac death in young athletes? |
- hypertrophic cardiomyopathy |
|
|
What are the manifestations of hypertrophic cardiomyopathy? |
Manifestation vary from none to significant physical limitations - dyspnoea + fatigue - angina - syncope - arrythmia + palpitations |
|
|
How is cardiomyopathy treated? |
- medication - pacemakers - defibrillators - ablation - ventricular assist devices - heart transplant (most treatments are symptomatic) |
|
|
What are 4 types of pericardial disorders? |
- Pericarditis (inflammation of pericardium) - Pericardial effusion (fluid build up in pericardium) - Cardiac tamponade (compression of heart due to fluid build up in pericardium - Constrictive pericarditis (fibrous scar develps between layers of pericardium) |
|
|
What are the manifestations of acute pericarditis? |
- sudden onset of severe chest pain, which radiates to the back - pain worsens with respiration and when lying down - dyspnoea |
|
|
What are possible causes of pericarditis? |
- infection - SLE - RA - uremia - postcardiac surgery - trauma |
|
|
What are the manifestations of pericardial effusion? |
- may be asymptomatic - dull constant ache in left side of chest - may present with cardiac tamponade - dysphagia - dyspnoea - muffled heart sounds |
|
|
What is a distended jugular vein a manifestation of? |
- Right sided heart failure
- Cardiac tamponade - constrictive pericarditis |
|
|
What are the manifestations of cardiac tamponade? |
- distended jugular veins - hypotension - arrythmia - dyspnoea - tachypnoea (rapid breathing) - pulsus paradoxus (decrease in BP of around 10mmHg while inspiring) |
|
|
What is pulsus paradoxus? |
Abnormal drop (around 10mmHg) in systolic BP while breathing in |
|
|
What are the manifestations of constrictive pericarditis? |
- ascites (swollen abdomen) - oedema - dyspnoea - jugular vein distension - hypotension -arrythmias - weight loss - exercise intolerance |
|
|
What is infective endocarditis? |
- Infection of the endocardial surface, including valves |
|
|
What is the mortality rate of infective endocarditis? |
- Very high. - 100% if not recognised and treated correctly |
|
|
What are some predisposing factors for endocarditis? |
- prosthetic heart valves - preexisting valvular disease of endocardial defect - oral lesions |
|
|
What are the manifestations of endocarditis? |
- fever, malaise and endurance fatigue - heart murmur, weight loss and coughing - anaemia - night sweats - splenomegaly |
|
|
The narrowing of a heart valve opening so it does not open properly is known as what? |
Stenosis |
|
|
What are common manifestations of valvular disease? |
- pulmonary congestion - dyspnoea - hypertension - dizziness and fatigue - tachycardia, palpitations and angina - thromboembolism - ascites and oedema - syncope |
|
|
What are the causes of heart failure? |
- myocardial disease - valvular heart disease - congenital heart defects - constrictive pericarditis - acute myocardial infarction - Hypertension - Excessive work demand - volume overload |
|
|
What is the difference between systolic and diastolic heart failure? |
In systolic HF, the ventricular contraction is inadequate, causing a reduced SV. In diastolic HF, the ventricle does not adequately relax, causing inadequate filling of the ventricle and reduced SV. |
|
|
What is the difference between high output and low output heart disease? |
In high output, the heart is still pumping out a significant amount of blood, but still inadequate due to excessive metabolic demands of the body. This condition is rare In low output, there is an impaired ability to the heart to pump. This causes vasoconstriction and cold, pale cyanotic extremities. |
|
|
In right sided heart failure, where does blood back up? |
In the systemic circulation (right side moves blood from systemic to pulmonary) |
|
|
In left sided heart failure, where does blood back up? |
In the pulmonary circulation (left side moves blood from pulmonary to systemic) |
|
|
What are some causes of right sided heart failure? |
- Stenosis of right AV or semilunar valves (tricuspid and pulmonary) - infarction of right ventricle - cardiomyopathy - pulmonary disease |
|
|
What are some causes of left sided heart failure? |
- infarction of left ventricle - cardiomyopathy |
|
|
Would jugular vein distention be a sign of right or left side heart failure? |
Right side |
|
|
What are some manifestations of left sided failure? |
- tachypnoea/dyspnoea - lung crackles - breathlessness - wheezing, dizziness - pulmonary oedema - cyanosis - galloping heart rhythm - heart murmurs (many breathing difficulties) |
|
|
What are some manifestations of right sided heart failure? |
- pitting oedema (pit indentation after pressure applied) - ascites (abdominal swelling) - hepatomegaly (enlarged liver) - impaired liver function - distended jugular veins - excess fluid accumulation in body - nocturia (night time urination) |
|
|
What are some compensatory or adaptive mechanisms in heart failure? |
- frank starling mechanism - activation of sympathetic nervous system to increase HR - the RAAS system - myocardial hypertrophy/remodelling |
|
|
How is heart failure treated? |
treatment focussed on symptoms - correction of causes (e.g. hypertension) - reduce cardiac workload - medications - surgery |
|
|
What are the surgical treatments for heart failure? |
- resynchronisation - defibrillator implants - ventricular assist devices - transplant |
|
|
What is the definition of cardiac shock? |
- collapse of systemic arterial blood pressure - blood diverted away from peripheral tissues and organs to supply vital organs (heart/lungs/brain) |
|
|
What is hypovolaemic shock? |
When the volume of circulating blood is reduced |
|
|
What are the manifestations of hypovolaemic shock? |
- hypotension - anxiety, restlessness - rapid, weak pulse - cold clammy skin - rapid, shallow breathing - hypothermia - thirst + dry mouth - fatigue/inability to concentrate |
|
|
What is cardiogenic shock? |
Damage to the heart results in sudden inability to effectively pump blood. |
|
|
What are the additional manifestations of cardiogenic shock? |
In addition to hypovolaemic shock manifestation - distended jugular veins - arrythmia |
|
|
What is obstructive shock? |
Obstruction to coronary blood supply causes ineffective pumping |
|
|
What are the additional manifestations for obstructive shock? |
- distended jugular veins - pulsus paradoxus in case of cardiac tamponade |
|
|
What is distributive shock? What are 3 types of distributive shock? |
Vasodilation in the vessels causes reduced BP. - Septic shock (following infection) - Neurogenic shock (sudden loss of vascular tone due to neural injury/dysfunction) - anaphylactic (following allergic response and release of inflammatory agents) |
|
|
What are the additional manifestations for septic shock? |
- fever - vasodilation / hypotension - reduced contractility - increase white blood cells (leukoctyes + neutrophils) - warm, sweaty skin |
|
|
What are the additional manifestations for neurogenic shock? |
- bradycardia due to damaged sympathetic NS - warm, dry skin with clear sweat lines |
|
|
What are the additional manifestations of anaphylactic shock? |
- skin eruptions and large bumps - localised oedema - breathing difficulties due to narrowed airways |
|
|
What are some complications of shock? |
- Tissue hypoxia and necrosis - respiratory distress - renal failure - gastrointestinal complications - multiple organ dysfunction syndrome |
|
|
How is shock treated? |
- improve cardiac output - reducing workload and oxygen demands - increasing coronary perfusion - monitoring volume - affecting peripheral resistance |