Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
299 Cards in this Set
- Front
- Back
|
What is a neglected tropical disease?
|
- serious bacterial & parasitic disease that affect > 1 bil people worldwide
- impair physical & cognitive development - cause maternal & child morbidity & mortality - impact earning capacity |
|

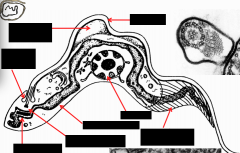
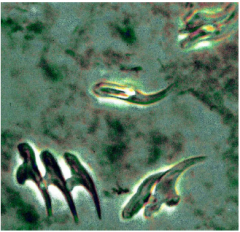
What parasite is this? What is labeled in the image? What are the 2 strains and where are they native?
What is there unifying feature? |
TRYPANOSOMES (-IASIS) - PROTOZOA
1. Kinetoplast 2. Nucleus "Old World" - Africa - cattle, sheep, goats, wild game, humans "New York" - South America - cats, dogs, armadillo, humans Unifying feature = KINETOPLAST; also has flagella & stains with Giemsa |
|

What insect is this? What parasite does it carry?
|
TSETSE FLY
In the east: G. morsitans In the west: G. palpalis Carries trypanosomes - protozoa Causes a PAINFUL bite |
|
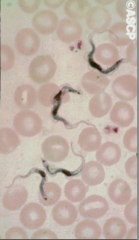
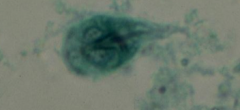
What parasite is this? Label.
|
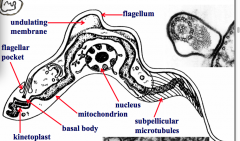
trypanosomes
|
|
|
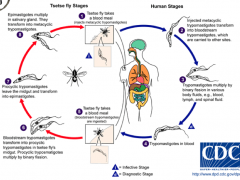
What is the life cycle of trypanosomes?
|
|
|
|
What is the species of African trypanosomiasis?
|
Trypanosoma brucei complex
- T. b. brucei - game animals/livestock - T. b. rhodesiense - E. African trypanosomiasis - wild animal reservoir = bush buck; zoonosis! - T. b. gambiense - W. & Central African sleeping sickness - 60 mil & risk, 25-45K cases, 3-500K estimated cases |
|
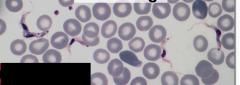
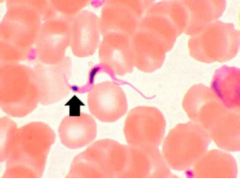
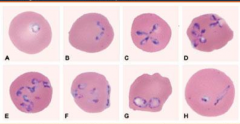
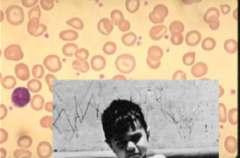
What disease is this? What stage?
|
trypanosomiasis!
BLOOD STAGE - in the blood stream: - it looks long and slender - rapidly replicates - undergoes binary fission - (at this point, can't tell if it's African or S. Am) |
|

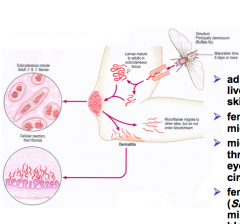
A bite from what animal caused this? What disease does it spread?
|
Tsetse bite - trypanosomiasis
- tsetse are 'pool feeders' which lacerate skin and suck up blood in the lesion - metacyclic trypomastigotes in the saliva enter the bite wound - the bite may cause PAIN and HYPERSENSITIVITY |
|
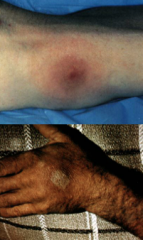
These images are WHAT STAGE of WHAT DISEASE?
|
- ACUTE/BLOOD STAGE of TRYPANOSOMIASIS
- 1-3 week asymptomatic incubation period - sometimes local inflammation - trypanosomal chancre - parasite replication at bite site - invasion of blood characterized by IRREGULAR FEVER & headache |
|
|
How do T. rhodesiense vs. T. gambiense differ in their disease course?
|
T. rhodesiense: can --> FULMINATING (rapid, R= rapid infection)
T. gambiense: can be self-limiting or slowly progressing to more serious disease |
|

What DISEASE and STAGE is depicted here?
|
-TRYPANOSOMIASIS - LYMPHATIC STAGE
-disease progression often involves invasion of lymphatics - Winterbottom's sign: CERVICAL ADENOPATHY - Itching - Edema - Continued febrile attacks - Weight loss - Weakness - CACHEXIA!!!!!!!! - severe weight loss |
|
|
What is the CNS disease course of trypanosomiasis?
|
- parasites cross blood-brain barrier
- meningoencephalitis - increased apathy & fatigue - confusion & somnolence - motor changes --> tics, slurred speech, incoordination - convulsions, coma - progression to CNS involvement is RAPID! IN EAST AFRICAN TYPE!!!! and SLOW in WEST AFRICAN TYPE!!! - death from disease or other infections |
|
|
Is CNS involvement faster in East African or West African types of trypanosomiasis disease?
|
EAST AFRICAN is fast
|
|
What disease is this?
|
trypanosomiasis
|
|
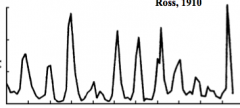
What is the significance of this graph as it relates to trypanosomes?
|
trypanosomiasis - parasitemia fluctuates in real time - there are variations in the surface glycoproteins - explains HIGH SPIKING FEVERS
- peak parasitemia usually associated with intermittent fever or other symptoms - parasites from peaks are antigenically distinct i.e. variant antigenic types which produce variant surface glycoproteins (VSG) |
|
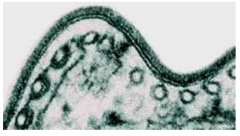
What is this image of trypanosomiasis depict?
|
- variant surface glycoprotein of trypanosomiasis - it changes often and that is why fevers spike variably
- form electron dense surface |
|
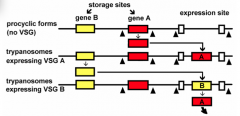
As it relates to trypanosomiasis, what is the significance of this image?
|
- antigenic switching
- genes convert back and forth - there are 100s of VSG genes - conserved regions - switch rate = 10^-3-10^-5 per generation - VSG is IMMUNOGENIC and HOST RESPONSE clears parasites - some trypanosomes will CHANGE VSG coat - this population expands until host develops immunity against new VSG |
|
|
How do you diagnose trypanosomiasis?
|
Clinical Features:
- travel/residence in endemic area - history or scar of 'trypanosomal chancre' (necrotic) - irregular fever, enlarged lymph nodes (post/cervical), loss of weight - behavioral changes/mental symptoms LAB - serological tests: IFA, ELISA, CATT - microscopy --> trypanosomes in blood or CSF (especially during fever) |
|
|
How do you detect African Trypanosomes?
|
Blood
- examine on several days - stained thin or THICK smears - fresh (characteristic movement) - buffy coat (microhemotocrit) - not routine - inoculate rats or mice |
|
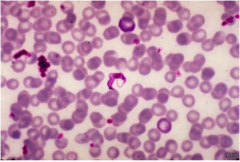
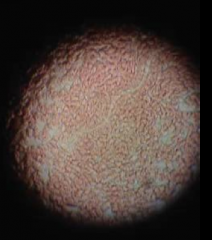
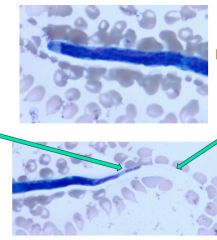
What is this?
|
trypanosomiasis on a blood smear
|
|

What is being done in this picture? What disease is it detecting?
|
- taking a lymph node aspirates
- fresh or stained - used to detect African Trypanosomes - you can also use CSF from spinal fluid - examine sediment, cells & protein |
|
|
What is the treatment for the early stage of trypanosomiasis with no CNS?
|
- suramin
- pentamidine - excellent prognosis |
|
|
What is the treatment of late stage of trypanosomiasis WITH CNS involvement?
|
- extremely difficult to treat
- Melarsoprol - arsenic based drug; HIGHLY TOXIC (4-12%) - Eflornithin (DFMO) +/- nifurtimox - expensive; 14 consecutive daily injections oral formulation in phase 3 trials |
|
|
What is the prophylaxis and control for trypanosomiasis?
|
- not drugs
- insect repellants - protective clothing - surveillance & treatment - traps, insecticides - habitat alteration |
|

The trap depicted here is meant to prevent what illness from spreading?
|
trypanosomiasis - trap tsetse flies
|
|
|
What does TRYPANOSOMA CRUZI cause? This disease is the leading cause of cardiac disease in which parts of the world?
|
Chagas disease!
S. and Central America |
|

What bug is this? What parasite and disease does it spread? Does the bite hurt?
|
- triatomine bug, reduviid bug, assassin bug, kissing bug, conenose bug
- spreads Trypanosoma cruzi - CHAGAS DISEASE - painless bite! |
|
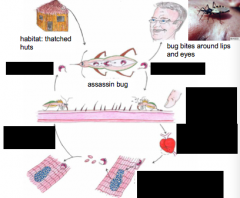
Which disease/parasite is indicated in this life cycle?
|
Trypanosoma cruzi
Bloodstream trypomastigotes are non-dividing Amastigotes in heart muscle replicate by binary fission |
|
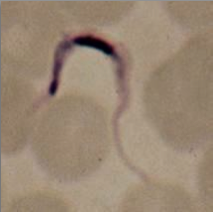
What parasite is this? What stain has been used?
|
- Trypomastigotes in blood smear
- Giemsa stain |
|
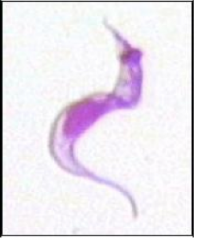
What parasite is this?
|
Trypomastigote
|
|
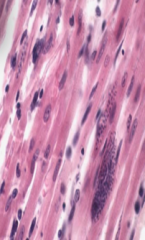
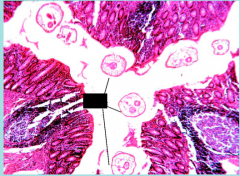
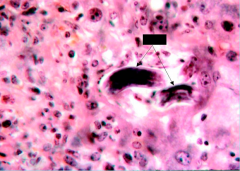
What does this image depict? What parasite?
|
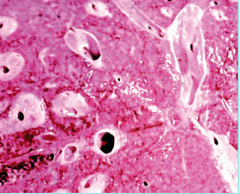
Amastigotes in heart muscle - TRYPANOSOMA CRUZI
|
|
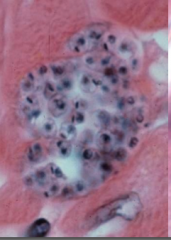
What does this image depict? What parasite?
|
Amastigotes in heart muscle - TRYPANOSOMA CRUZI
|
|
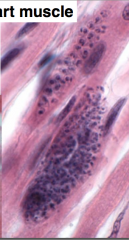
What does this image depict? What parasite?
|
Amastigotes in heart muscle - TRYPANOSOMA CRUZI
|
|

What bug is this and what does it spread?
What factors influence the HUMAN transmission of this disease? |
- kissing bug - TRYPANOSOMA CRUZI
Human transmission: - defecation dring triatomine bug feeding - bug bites human, poops near the bite, poop with parasite enters wound - colonization of human habitats - adobe walls, thatched roofs - para-domiciliary cycles - animal stalls next to homes - proximity to sylvatic cycle |
|
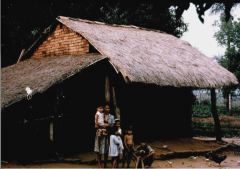
What is significant about this image as it relates to spread of trypanosoma cruzi?
|
Thatched huts are favorite hiding places for triatomine bugs
|
|
|
What is the clinical course of chagas disease?
|
Acute - active infection (1-2 week incubation); 1-4 months duration, MOST ASYMPTOMATIC
Indeterminate phase - 10-30 yrs of latency; relatively asymptomatic w/ no detectable parasitemia; seropositive Chronic phase - 10-30% of infected exhibit cardiomyopathy |
|
|
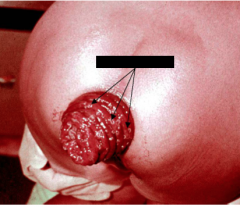
What are some potential symptoms in acute phase Chagas?
|
MOST ASYMPTOMATIC
- local inflammation - Romana's sign (puffy eye) - Chagoma (see lesion + worm on the surface of skin) - fever, malaise, lymphadenopathy, hepatosplenomegaly, nausea, diarrhea - acute, fatal myocarditis in SOME |
|

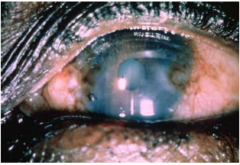
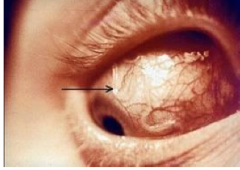
What is this? What disease is it indicative of?
|
ROMANA'S SIGN
Chagas' disease - trypanosoma cruzi Acute phase |
|

What is this? What disease is it indicative of?
|
Chagoma
Chagas' disease - trypanosoma cruzi Acute phase |
|
|
What is chronic chagas' cardiomyopathy?
|
- long latency characterized by seropositivity and no parasitemia
- progressive development of abnormalities - clinical presentations include: arrhythmias; heart block; conduction defects; congestive heart failures; thromboembolic phenomenon |
|
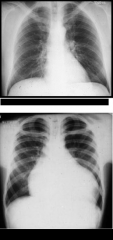
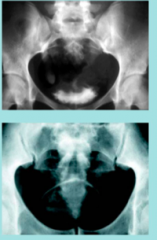
Which is normal? What parasitic disease is this indicative of?
|
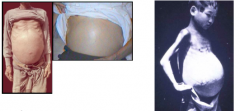
- Top is normal, Bottom has CARDIOMEGALY from Chagas' disease - trypanosoma cruzi
Typical pathology: - apical aneurysm - left ventricle - extensive fibrosis - hypertrophy - w/ or without cellular infiltrates |
|

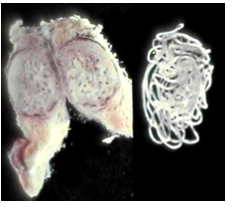
What parasitic disease has caused this cardiac disease?
|
Cardiomegaly due to Chagas' disease - trypanosoma cruzi
|
|
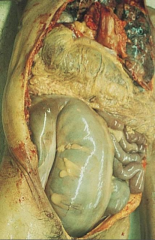
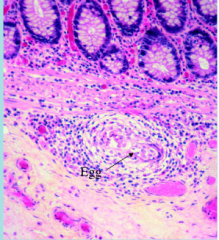
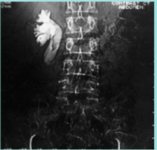
What is pathological here? What parasitic disease causes this?
|
- MEGAVISCERAE due to Chagas' disease - trypanosoma cruzi
- colon & esophagus most frequently affected - megaesophagus - painful swallowing, regurgitation - megacolon - severe constipation - loss of parasympthatic ganglia |
|
|
What is the basis of the pathogenesis of trypanosoma cruzi which causes Chagas' disease?
|
AUTOIMMUNITY vs. PARASITE-MEDIATED DESTRUCTION
- autoimmunity: because few if any parasites, anti-self responses (humoral & cellular), slow development, organ specificity - parasite-mediated destruction: persistent low level parasitemia (PCR), inflammation correlates w/ parasites, disease exacerbated by immune suppression - altered immune response? (Th1-Th2 switch correlated w/ severe disease) - chagistic factor or toxin? proposed, not found |
|
|
How do you diagnose Chagas' disease?
|
- parasite detection - direct examination, stained blood smears, in vitro culture, xenodiagnosis (rare)
- PCR - serological tests - hemagglutination, immunofluoresence, ELISA |
|
What parasite is this?
|
Trypanosoma
|
|

What parasite is this?
|
Trypanosoma
|
|
|
What is the treatment for Chagas' disease?
|
Acute stage:
- Nifurtimox (8-16 mg/kg/day, 60-90 days) - Benznidazole (5-7 mg/kg/day, 30-120 days) - been shown to do well after 8yrs if treated; but one study showed it wasn't effective - Azole antifungal agents (experimental) Chronic stage - treat symptoms - h |
|
|
How can we control the spread of Chagas?
|
- improve human dwellings
- separation of animal stalls from house - heath education - insecticides - screen blood supply |
|

What parasite is this?
|
Entamoeba histolytica (LEFT ARROW = fungal hyphase) (RIGHT ARROW = parasite ingesting fungus)
- cosmopolitan distribution - no animal reservoirs; facultative pathogen - can clear the infection spontaneously in 6-12 months with mild or no symptoms - can cause a serious invasive disease - worldwide incidence = 0.2-50% - estimated that 10% of world's population may be infected - 50 million cases of invasive amebiasis/yr - 100,000 deaths/yr - fungal hyphae |
|
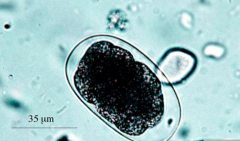
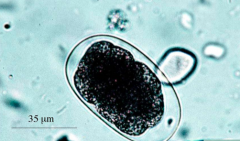
The lifecycle of what organism is depicted here?
|
Entamoeba histolytica
|
|

What organism is this?
|
Entamoeba histolytica - Excystation!
- occurs in small intestine - cyst wall disruption - ameba emerges - nuclear division (4-8) - cytoplasmic divisions - 8 amebala - trophozoites migrate to large intestine |
|
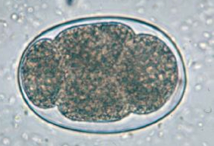
What parasite is this?
|
Entamoeba histolytica - trophozoite phase
- colonizes the large intestine - feed on bacteria/fungi and debris - replicate by binary fission |
|
What parasite is this?
|
Entamoeba histolytica - trophozoite phase
- colonizes the large intestine - feed on bacteria/fungi and debris - replicate by binary fission |
|

What parasite is this?
What process is depicted here? |
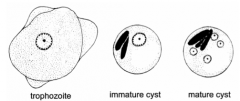
Trophozoite!
ENCYSTATION - - trophozoite rounds up - secretion of cyst wall - aggregation of ribosomes (= chromatid bodies) - 2 rounds of nuclear division (1-4 nuclei) - survive weeks to months |
|
|
What are the two types of Amebiasis?
|
NON-INVASIVE vs. INVASIVE
NON-INVASIVE - ameba colonize intestinal mucosa - asymptomatic --> pass cysts - may develop non-dysenteric diarrhea, abdominal cramps, nausea/emesis INVASIVE - necrosis of mucosa - ulcers, dysentery - ulcer enlargement - severe dysentery, colitis, peritonitis - metastasis - extraintestinal amebiasis |
|

What disease is depicted here?
|
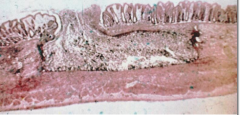
Amebiasis caused by Entamoeba histolytica
- note: ulcers with raised borders - little inflammation b/w lesions |
|
This histological slide is indicative of what disease?
|
Amebiasis caused by Entamoeba histolytica
- flasked-shaped ulcer - trophozoites at boundary of necrotic & healthy tissue - trophozoites ingest RBCs (hemophagocytic) - dysentery!!!!!! (blood & mucus) - spreads in muscular membrane - trophozoites chew, engulf and eat rbcs |
|
What disease is this? What is happening here?
|
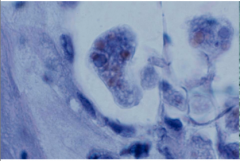
Amebiasis caused by Entamoeba histolytica
Here, the ameba are eating blood cells - hemophagocytic = erythrophagocytic = hematophagous trophozoites |
|

What disease is this? What is happening here?
|
Amebiasis caused by Entamoeba histolytica
Here, the ameba are eating blood cells - hemophagocytic = erythrophagocytic = hematophagous trophozoites |
|
What disease is this? What is indicated at the yellow arrow?
|
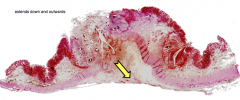
-Amebiasis caused by Entamoeba histolytica
-Lateral and Downward Expansion of Ameba into Lamina Propria -localized sloughing - ulcers coalesce yellow arrow = perforation of intestinal wall |
|

What disease caused this pathology?
|
Here, you see intestinal perforation associated with invasive Amebiasis caused by Entamoeba histolytica
|
|
|
What are the disease manifestations of Amebiasis caused by Entamoeba histolytica?
|
- asymptomatic
- dysentry - peritonitis - local abscesses - 2ndary bacterial infections from the gut, because it was invaded - toxic megacolon - ameboma = amebic granuloma (caecum) = inflammatory thickening of intestinal wall around the abscess (can be confused with tumor) |
|
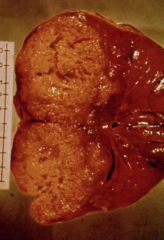
What disease is depicted here?
|
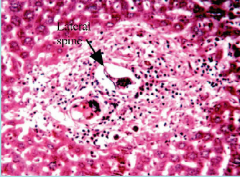
Amebiasis caused by Entamoeba histolytica
Extraintestinal amebiasis - this is an Amebic Liver Abscess - metastasis via blood stream - primarily liver (portal vein) - other sites less frequent - ameba-free stools common - hi antibody titers Amebic Liver Abscess - chocolate-colored pus - necrotic material - usually bacterial free - lesions expand and coalesce - further metastasis, direct extension or fistula |
|
|
Can you have pulmonary amebiasis?
|
Yes although it is rarely primary
- rupture of liver abscess thru diaphragm --> disease in lungs - empyema - lung abscess - 2ndary bacterial infections common - fever, cough, dyspnea, pain |
|

What disease is this?
|
Cutaneous Amebiasis caused by Entamoeba histolytica
|
|

What disease is this?
|
Cutaneous Amebiasis caused by Entamoeba histolytica
|
|

What disease/parasite is this?
|
Amebiasis caused by Entamoeba histolytica
|
|

What disease/parasite is this?
|
Amebiasis caused by Entamoeba histolytica
|
|

What disease/parasite is this?
|
Amebiasis caused by Entamoeba histolytica
|
|
|
What how do you diagnose Amebiasis caused by Entamoeba histolytica?
|
- intestinal = stool microscopy, sigmoidoscopy, lesions, aspirate, biopsy, antigen detection, PCR
- extraintestinal (hepatic) = signs/symptoms, imaging, serology, abscess aspiration, trophozoites at leading edge |
|
|
How do you treat Amebiasis caused by Entamoeba histolytica?
|
- asymptomatic or luminal nematode parasites - iodoquinol or paromomycin
- invasive & extra-luminal nematode parasites - metronidazole or tinidazole, followed by luminal agents - liver abscess - drain if high probability of rupture |
|
|
How do you handle control and epidemiology of Amebiasis caused by Entamoeba histolytica?
|
- avoid fecal-oral transmission
- not normally associated with travelers diarrhea except if >1 month stay - institutions - NOT MASS DRUG TREATMENT - better housing - focus on men who have sex with men - safe sex |
|
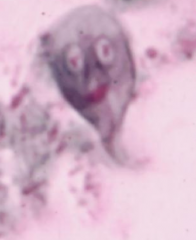
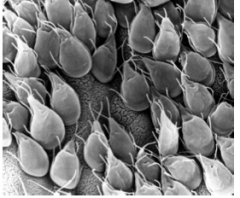
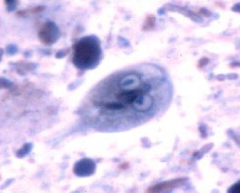
What pathogen/disease is this?
|
Giardia lamblia
Trophozoites with Owl's eye appearance -worldwide distribution -higher prevalence in tropical or developing countries (20%) -1-6% in temperate countries -most common protozoa in stools -~200 million cases/yr -often asymptomatic -acute or chronic diarrhea (giardiasis) -one human species: aka G. duodenalis & G. intestinalis -morphologically similar forms in other mammals |
|
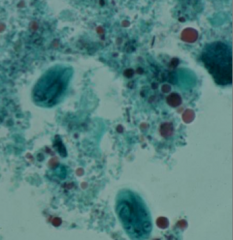
What pathogen/disease is this?
|
Giardia lamblia - giardiasis
Trophozoites with Owl's eye appearance -often asymptomatic -acute or chronic diarrhea (giardiasis) -one human species: aka G. duodenalis & G. intestinalis |
|
|
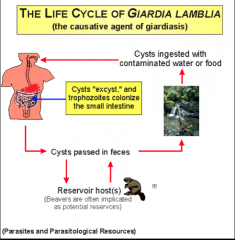
What is the life cycle of giardia lamblia?
|
|
|
What are factors of fecal-oral transmission in the disease depicted above?
|
Disease = giardia lamblia, giardiasis
- poor personal hygiene/sanitation - children (e.g. day care centers) - food handlers - developing countries - travelers - water-bone epidemics - MSM - oral-anal contact - zoonosis = controversial |
|
|
Is giardiasis a zoonosis?
|
• no definitive documentation
• transmission between humans and dogs rare (J.Parasit. 83:44, 1997) • person-to-person transmission is most prevalent |
|

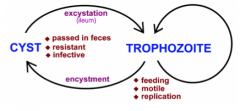
What disease is this? Label each part.
|
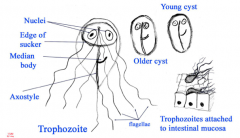
- giardia
- trophozoite - replicative stage inhabiting small intestine - cyst - infective stage passed in feces |
|
|
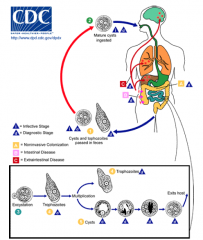
What is the life cycle of giardia?
|

|
|

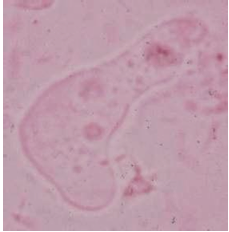
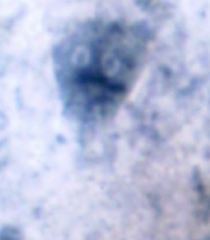
What parasite is depicted here? What phase of its life cycle is it?
|
giardia
cyst phase |
|
What parasite is depicted here? What phase of its life cycle is it?
|
giardia
cyst phase |
|

What parasite is depicted here? What phase of its life cycle is it?
|
giardia
cyst phase |
|
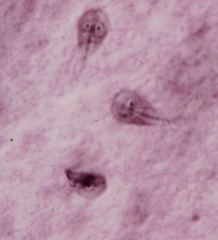
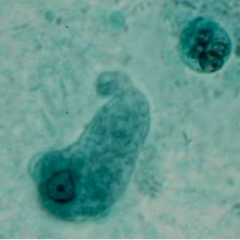
What parasite is depicted here? What phase of its life cycle is it?
|
giardia
trophozoite phase |
|
What parasite is depicted here? What phase of its life cycle is it?
|
giardia
trophozoite phase |
|
What parasite is depicted here? What phase of its life cycle is it?
|
giardia
trophozoite phase |
|
|
What are the clinical features of giardia?
|
- Range of Outcomes: asymptomatic/latent, acute short-lasting diarrhea, chronic/nutritional disorders
- Acute symptoms: 1-2 week incubation, sudden explosive, watery diarrhea, bulky, frothy, greasy, foul-smelling stools, no blood or mucus, epigastric pain, bloating, flatulence, belching, cramps, nausea, vomiting, anorexia, usually clears spontaneously (undiagnosed), but can persist or become chronic - Subacute/Chronic: recurrent diarrheal episodes, cramps uncommon, sulfuric belching, anorexia, nausea, weight loss & FTT |
|
What disease is this? What is the pathogenesis of this disease?
|
Pathogenesis
-epithelial damage -villus blunting -crypt cell hypertrophy -cellular infiltration -malabsorption -lactase deficiency (lactose intolerance) |
|
|
How do you diagnose giardia?
|
-stool antigen assay
-O&P (microscopy) -Previously: string test/enteric capsule (Enterotest), duodenal aspirate or biopsy - parasite can be difficult to detect - intermittent excretion in feces - patchy loci of infection |
|
|
How do you treat and control giardia?
|
-Treat - Drug of Choice = metronidazole (Flagyl) [500 mg/bid/5-7d] >90% cure rate
-Alternatives: tinidazole (single dose); nitazoxanide, paromomycin (safe in pregnancy); furazolidone (not in U.S.) -Prognosis is good with no sequelae CONTROL: avoid fecal-oral transmission, improve personal hygiene & sanitation, treat asymptomatic carriers, heath education, food handling, protect water supply, treat water if questionable - boiling & iodine |
|
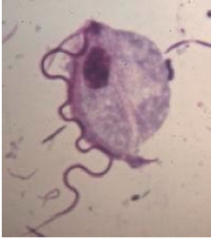
What pathogen is this?
|
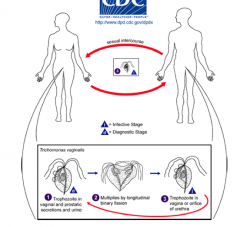
-Trichomonas vaginalis AKA 'trich'
- flagellated protozoa - most common curable STI: up to 15% women - incubation: 5-28 days - women: 85% asymptomatic; thin malodorous foamy vaginal discharge (green/yellow), vag/vulvar inflammation, dyuria, dysparunia - pregnancy: PROM,preterm delivery, LBW - men: most are asymptomatic; NGU, prostatitis |
|
|
What is the life cycle of trich?
|
|
|
|
How do you diagnose and treat trich?
|
Diagnosis:
-Fresh wet prep of vaginal, urethral, prostatic secretions (60% sensitive) -Dipstick test (immunochromographic; >83% sensitive) -Affirm VP (nucleic acid probe test; >83% sensitive) -NAAT (Amplicor, APTIMA, up to 98% sensitive) Treatment: Single dose of: metronidazole or Tinidazole Treat partners concurrently |
|

What family of parasite is this?
|
Intestinal coccidian
-Cryptosporidium parvum (famous outbreak Milwaukee 1993) -Cyclospora cayetanensis -Isosporal belli -spread by contaminated drinking / recreational water, food, person-to-person -watery diarrhea --> prolonged in HIV/AIDS -diagnosis: modified AFB -Rx: C. parvum=nitazoxanide - Cyclospora/ Isospora=TMP/SMX |
|
What parasite is this?
|
Balantidium coli
-Ciliated trophozoites; largest human protozoa -Causes dysentery but no extraintestinal disease |
|

What parasite is this?
|
Balantidium coli
-Ciliated trophozoites; largest human protozoa -Causes dysentery but no extraintestinal disease |
|
What parasite is this?
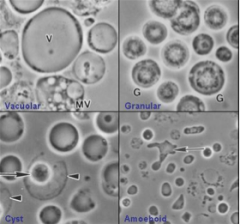
|
Blastocystis hominis - may be nonpathogenic
Rx: metronidazole, nitazoxanide |
|
|
What are the species of free-living amoeba?
|
Naegleria fowlerii (ponds & lakes)
Acanthamoeba spp * Balamuthia mandrallaris * * immunocompromised hosts |
|
|
Why is malaria considered a problem?
|
- almost half of the world's population is at risk for malaria?
- in 2010, 225 mil people w/ malaria - 2010 killed 1.2 mil people - 90% deaths occur in sub-Saharan Africa - 85% of deaths in children <5 yrs onset age i.e. most vulnerable population - malaria is most important single infectious killer of children on planet - drug resistance is prevalent |
|
|
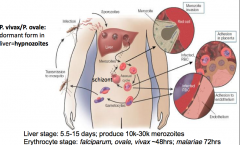
What is the lifecycle is malaria?
|
|
|
|
Which is the male and which is the female mosquito? Which is the one that can transmit malaria?
|
L - female - can spread malaria
R - male |
|
|
What are the strains of malaria?
|
Genus = plasmodium
Species = falciparum (worldwide) vivax - S. America, Asia ovale - Africa malariae - Africa, S. America, Asia knowlesi - primarily primates, Asia |
|
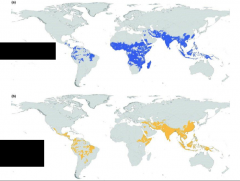
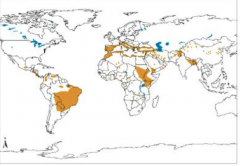
Which strains of malaria are endemic to each of the shaded areas?
|
blue = P. falciparum
yellow = P. vivax |
|
|
Which genes have been effected by malaria?
|
Malaria selected for mutations erythrocyte-associated genes:
1.sickle cell anemia gene 2.B-thalassemia gene 3.G-6PD gene 4.Duffy antigen (receptor for P. vivax) |
|
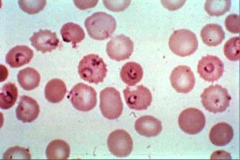
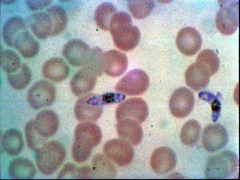
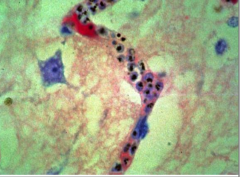
What parasite is this? What disease does it cause?
|
Plasmodium flaciparum - MALARIA
|
|
What parasite is this? What disease does it cause?
|
Plasmodium flaciparum - MALARIA
|
|
|
What are the symptoms of mild malaria?
|
-severe flu like syndrome
-headache -myalgia -bone pain -abdominal pain, diarrhea -recurrent chills/fever followed by defervescence. -anemia/splenomegaly |
|
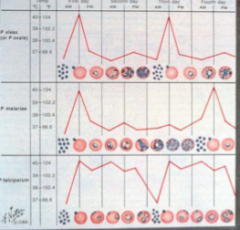
What, related to malaria, is depicted here?
|
Temperature curves relative to parasite levels
Top = P. vivax Middle = P. malariae Bottom = P. falciparum |
|
|
What are the symptoms of severe malaria?
|
-cerebral malaria- falciparum
-severe anemia- falciparum -placental malaria- falciparum -algid malaria - (bacterial sepsis) - falciparum -pulmonary/GI malaria - falciparum -blackwater fever - falciparum -hypoglycemia - falciparum -splenic rupture - vivax -nephrotic syndrome - malariae |
|
|
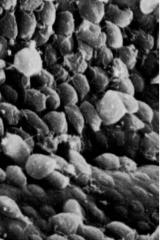
How does P. falciparum causes disease?
|
-Infected red cells have KNOB-LIKE protrusions on their surface.
-Knobs contain parasite proteins which STICK to walls of BLOOD VESSELS. -Infected red cells stick and clog small blood vessels and capillaries. -Location of clog dictates type of symptoms. |
|
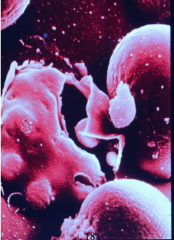
What parasite/disease is this?
|
P. falciparum - malaria
|
|
What parasite/disease is this?
|
P. falciparum - malaria
|
|
|
What is the WHO eradication plan for malaria?
|
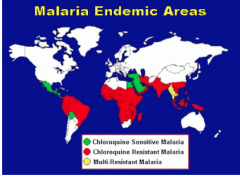
- In 1950’s, WHO sponsored a DDT/chloroquine eradication plan
- initially great success - insects and parasites rapidly became resistant to both interventions - Chloroquine sensitive: Central America west of Panama Canal, Haiti & Dominican Republic, Middle East |
|
|
How can you reduce the morbidity and mortality of malaria?
|
-Anti-malarials to treat and cure symptomatic cases
-Limitations: no vaccine yet, multi-drug resistance emerging, distribution & cost of drugs |
|
|
What are the issues with malaria in pregnancy?
|
-primigravid > secundigravid >>> multigravid
-Parasites bind placental chondroitin sulfate A (CSA) via PfEMP1 -major cause of IUGR, low birth weight, prematurity, perinatal infant mortality and anemia, and mortality in mother |
|
|
How do you diagnose malaria?
|
•Critical to obtain travel history!
•Microscopy ---- blood smears: thick for diagnosis and thin for speciation and quantitation ---- at least 3 blood tests if smear neg and suspicion high •rapid diagnostic tests - e.g. BinaxNOW; Paracheck •PCR (research) •leucopenia, anemia, thrombocytopenia, transaminitis, hyperbilirubinemia |
|
|
Do we have vaccines for malaria?
|
- no vaccines for parasites
- new malaria vaccine in Phase 3 trial: RTS,S - moderately effective in infants (30- 50%) |
|
|
How do you prevent spread of malaria?
|
-long-acting insecticide-treated bednets
-indoor residual spraying (IRS) -reduce mosquito breeding sites -Intermittent preventive therapy in pregnancy LONG-TERM SOLUTION: effective vaccine, effective/ cheap medications, and diverse control measures |
|
|
Which of the plasmodium species causes most serious complications in humans?
|
Plasmodium falciparum
|
|
|
What is leishmaniasis?
|
-parasitic disease transmitted by the bite of infected female sandflies (dusk to dawn)
->20 species of parasite transmitted by 30 species of sandfly (Phlebotomus and Lutzomyia). -found in >90 countries worldwide (tropics, subtropics, Middle East and southern Europe) -3 forms: -----cutaneous: involving the skin at the site of bite (L. tropica, L. major, L. mexicana, L. braziliensis) 0.7-1.2 million new cases/year -----mucocutaneous: involving mucous membranes of the mouth and nose after spread from a nearby cutaneous lesion (L. braziliensis) -----visceral: involving liver, spleen, and bone marrow (L. donovani) 0.2- 0.4 million new cases/year |
|
The distribution above is most associated with what form of Leishmaniasis?
|
VISCERAL
-90% of cutaneous leishmaniasis occurs in Afghanistan, Iran, Saudi Arabia, Syria, Brazil and Peru -90% of all visceral leishmaniasis occurs in Bangladesh, India, Nepal, Sudan, and Brazil -90% of mucocutaneous leishmaniasis occurs in Bolivia, Brazil and Peru |
|
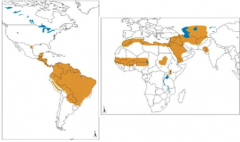
The distribution above is most associated with what form of Leishmaniasis?
|
CUTANEOUS
-90% of cutaneous leishmaniasis occurs in Afghanistan, Iran, Saudi Arabia, Syria, Brazil and Peru -90% of all visceral leishmaniasis occurs in Bangladesh, India, Nepal, Sudan, and Brazil -90% of mucocutaneous leishmaniasis occurs in Bolivia, Brazil and Peru |
|
|
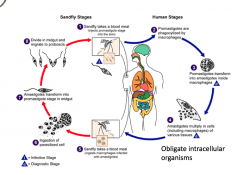
What is the lifecycle of Leishmaniasis?
|
|
|
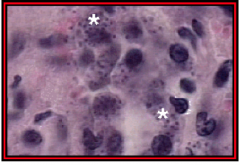
What parasite/disease is depicted here?
|
L. donovoni amastigotes in spleen - Leishmaniasis
|
|

What parasite/disease is depicted here?
|
L. donovoni amastigotes in spleen - Leishmaniasis
|
|

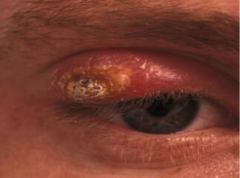
What disease is this? What organism?
|
-Cutaneous Leishmaniasis - L. tropica, L. major, L. mexicana, L. braziliensis
|
|

What disease is this? What organism?
|
-Cutaneous Leishmaniasis - L. tropica, L. major, L. mexicana, L. braziliensis
-Most common form -Characterized by one or more sores, papules or nodules on the skin -Sores can change in size and appearance over time -Often described as a volcano with a raised edge and central crater -Sores are usually painless but can become painful if secondarily infected -Swollen lymph nodes may be present near the sores (under the arm if the sores are on the arm or hand...) -lesions develop within weeks to months of the sandfly bite -lesions can heal on their own, but this can take months or even years -leave scars and can be disfiguring esp. if on face |
|

What disease is this? What organism?
|
-Cutaneous Leishmaniasis - L. tropica, L. major, L. mexicana, L. braziliensis
-Most common form -Characterized by one or more sores, papules or nodules on the skin -Sores can change in size and appearance over time -Often described as a volcano with a raised edge and central crater -Sores are usually painless but can become painful if secondarily infected -Swollen lymph nodes may be present near the sores (under the arm if the sores are on the arm or hand...) -lesions develop within weeks to months of the sandfly bite -lesions can heal on their own, but this can take months or even years -leave scars and can be disfiguring esp. if on face |
|

What disease is this? What organism?
|
-Cutaneous Leishmaniasis - L. tropica, L. major, L. mexicana, L. braziliensis
-Most common form -Characterized by one or more sores, papules or nodules on the skin -Sores can change in size and appearance over time -Often described as a volcano with a raised edge and central crater -Sores are usually painless but can become painful if secondarily infected -Swollen lymph nodes may be present near the sores (under the arm if the sores are on the arm or hand...) -lesions develop within weeks to months of the sandfly bite -lesions can heal on their own, but this can take months or even years -leave scars and can be disfiguring esp. if on face |
|

What disease is this? What organism?
|
-Cutaneous Leishmaniasis - L. tropica, L. major, L. mexicana, L. braziliensis
-Most common form -Characterized by one or more sores, papules or nodules on the skin -Sores can change in size and appearance over time -Often described as a volcano with a raised edge and central crater -Sores are usually painless but can become painful if secondarily infected -Swollen lymph nodes may be present near the sores (under the arm if the sores are on the arm or hand...) -lesions develop within weeks to months of the sandfly bite -lesions can heal on their own, but this can take months or even years -leave scars and can be disfiguring esp. if on face |
|
What disease is this? What organism?
|
-Cutaneous Leishmaniasis - L. tropica, L. major, L. mexicana, L. braziliensis
-Most common form -Characterized by one or more sores, papules or nodules on the skin -Sores can change in size and appearance over time -Often described as a volcano with a raised edge and central crater -Sores are usually painless but can become painful if secondarily infected -Swollen lymph nodes may be present near the sores (under the arm if the sores are on the arm or hand...) -lesions develop within weeks to months of the sandfly bite -lesions can heal on their own, but this can take months or even years -leave scars and can be disfiguring esp. if on face |
|

What disease is this? What organism?
|
Mucocutaneous Leishmaniasis - "espundia"
L. braziliensis -L. donovani in Central and South America -rarely L. tropica in the Middle East - cutaneous lesion on the face spreads to involve the nose or mouth -months to years after original skin lesion -lesions can be very disfiguring |
|

What disease is this? What organism?
|
Mucocutaneous Leishmaniasis - "espundia"
L. braziliensis -L. donovani in Central and South America -rarely L. tropica in the Middle East - cutaneous lesion on the face spreads to involve the nose or mouth -months to years after original skin lesion -lesions can be very disfiguring |
|

What disease is this? What organism?
|
-Visceral Leishmaniasis: L. donovani
-kala-azar - Hindi for “fatal fever/illness” -most severe form of the disease, may be fatal if left untreated -spiking fever, weight loss, & an enlarged spleen & liver -anemia (low RBC), leukopenia (low WBC), & thrombocytopenia (low platelets) are common (=pancytopenia) -lymphadenopathy may be present -Opportunistic infection in HIV/AIDS -symptoms usually occur months after sandfly bite - Soldiers from Desert Storm presented up to five months after leaving the Persian Gulf -because symptoms are non-specific there is usually a delay in diagnosis -visceral leishmaniasis should be considered in any chronic FEVER patient returning from an endemic area. |
|
|
How do you diagnose Leishmania?
|
-Heightened awareness -- think of Leishmania in exposed individuals
-Lesions that do not heal need to be referred for evaluation -Exposed individuals with fevers, weight loss, gastrointestinal complaints, anemia, abnormal liver tests should be referred for evaluation |
|
|
How do you diagnose cutaneous Leishmaniasis?
|
-Biopsy is required for diagnosis: Giemsa- stain of tissue smears
-Biopsy specimens can be sent to Walter Reed (WRAIR) for diagnosis -Leishmania Diagnostics Laboratory - microscopy, culture and PCR - mail out kits/instructions available |
|
|
How do you diagnose visceral Leishmaniasis?
|
-Presentation is usually very non-specific and should be considered in febrile patients with exposure
-Antibodies to Leishmania (Kalazar DetectTM) may be present in patient’s serum but this will not distinguish between past or current infection and cross-react with Trypanosomiasis -Diagnosis requires finding Leishmania on biopsy of bone marrow, liver, enlarged lymph node, or spleen (macrophages contain amastigotes) |
|
|
How do you treat cutaneous & mucocutaneous Leishmaniasis?
|
-Miltefosine for both cutaneous and visceral disease
-Antimony (Pentostam®, Sodium stibogluconate) is former drug of choice -----20 days of intravenous therapy -Fluconazole may decrease healing time in L. major infection -----Biopsy and culture to determine species is required -----6 weeks of therapy is needed |
|
|
How do you treat visceral leishmaniasis?
|
-Liposomal amphotericin-B (AmBisome®) is the drug of choice
----3 mg/kg per day on days 1-5, day 14 and day 21 -Pentostam® (sodium stibogluconate) is an alternative therapy ----28 days of therapy is required -Oral miltefosine ----99% cure rate at 6 months |
|
|
How do you prevent leishmaniasis?
|
-control the reservoir: rodents
-control the vector: sandfly -indoor residual spraying with insecticide -prevent sandfly bites: personal protective measures ----most important at night ----cover skin with clothes ----insect repellent with DEET ----permethrin treated bed nets |
|

What parasitic disease is carried by this?
|
Babesiosis
Ixodes tick - same as lyme disease mimics mild malaria: fever, hepatosplenomegaly, hemolytic anemia, thrombocytopenia, jaundice asplenia and immunosuppression are main risk factors for death Rx: clindamycin/quinine or atovaquone/azithromycin |
|
What disease is depicted here?
|
Babesiosis
- thick and thin blood smear - Maltese cross formations - PCR assay mimics mild malaria: fever, hepatosplenomegaly, hemolytic anemia, thrombocytopenia, jaundice asplenia and immunosuppression are main risk factors for death Rx: clindamycin/quinine or atovaquone/azithromycin |
|

What parasitic disease follows this pattern of distribution?
|
Babesiosis
|
|
|
What are the two main categories of Nematodes?
|
Nematodes = ROUNDWORMS
Luminal nematodes & Tissue Nematodes -ALL eukaryotes - caenorhabitis elegans is the best example, free-living in soul -MOST NON-PARASITIC: >dependence on O2 < likely to be parasites (Strongyloides stercoralis)... <dependence on O2, more advanced the parasite (Enterobius vermicularis) - almost 4 bil people w/ 1+, many have >1 - night soil - human excrement used as fertilizer - is responsible for much of the spread |
|
|
What are the luminal nematodes?
|
Ascaris - largest round worm
Hookworm - Fe deficiency Pin Worm - itchy butt Strongyloides - only worm that can multiply within host Whip Worm - rectal prolapse |
|
|
What are the soil-transmitted helminths? [Aka geohelminths]
|
Ascaris lumbricoides 1.2 billion
Trichuris trichiura 800 million Hookworms 740 million Mostly in sub-Saharan Africa, the Americas, China and east Asia |
|

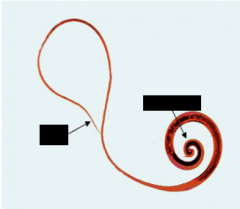
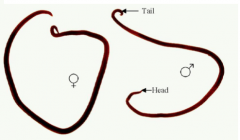
What parasite is this?
|

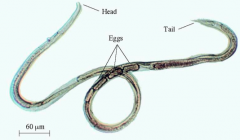
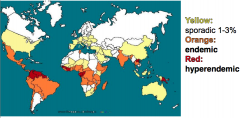
Enterobius vermicularis - Pinworm - (Adult Female)
Left --> Right = head, ovary with eggs, tail - NO CLINICAL DISEASE -most common human helminth in the U.S -ingest the eggs -no soil, lung or GI invasion phases -life cycle = eggs contaminate fingers --> kid sucking thumb --> larvae hatch in small intestine --> larvae migrate to colon --> adults mature in colon --> gravid adults migrate out of anus --> eggs embryonate on perineum --> back to beginning |
|

What parasite is this?
|
Heavy infection of Enterobius vermicularis
NO CLINICAL DISEASE |
|

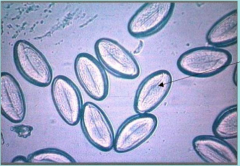
What parasite is this?
|
Eggs of Enterobius vermicularis
UNEMBRYONATED NO CLINICAL DISEASE |
|

What parasite is this?
|
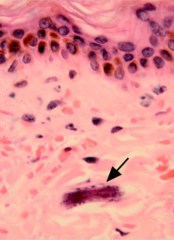
Eggs of Enterobius vermicularis
Embryonated - arrow points to LARVA NO CLINICAL DISEASE |
|
What parasite is this?
|
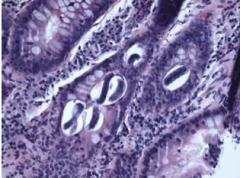
Enterobius vermicularis in appendix
Arrows: alae NO CLINICAL DISEASE |
|
What parasite is this?
|
Enterobius vermicularis
Arrows: larva These eggs may be found on microscopic examination of clear sticky tape - scotch tape test NO CLINICAL DISEASE |
|
|
How do you treat Enterobius vermicularis?
|
albendazole*
mebendazole* pyrantel pamoate single dose + repeat after 2 weeks * inhibits polymerization of microtubules which results in depetion of glycogen stores (has no effect on human tubulin) Difficult to prevent and control because children spread them; we outgrow pinworm in puberty |
|

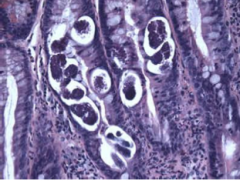
What PARASITE and GENDER is this?
|
Trichuris trichiura - Whipworm - FEMALE
-3rd most common human helminth globally -soil phase and local GI invasion but no lung phase --Ingest the eggs |
|
What PARASITE and GENDER is this?
|
Trichuris trichiura - Whipworm - MALE
-3rd most common human helminth globally -soil phase and local GI invasion but no lung phase --Ingest the eggs |
|

The life cycle of what parasite is depicted here?
|
Trichuris trichiura - whipworm
|
|
What is the parasite that caused this? What are the clinical findings of such a parasite?
|
Trichuris trichiura - arrow points to Trichuris adults
-asymptomatic -abdominal pain, nausea -mucus/blood in stool -anemia -rectal prolapse -chronic infection |
|
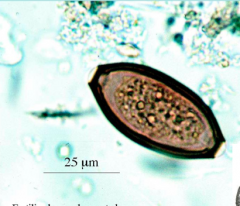
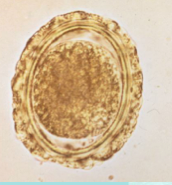
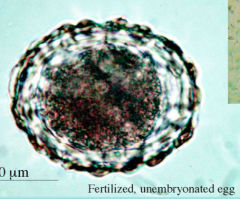
What is this a picture of? How do you diagnose this parasite?
|
-Trichuris trichiura - fertilized, unembryonated egg
-microscopic examination of feces for eggs - look for "TEA-TRAY" "TRICHURIS trichiura" shape of egg |
|
|
What is the treatment for tricuris trichura?
|
albendazole (3 days)*
mebendazole (3 days)* * inhibits polymerization of microtubules which results in depetion of glycogen stores (has no effect on human tubulin) |
|
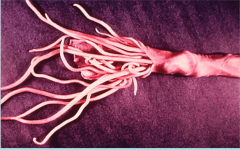
What organism is this?
|
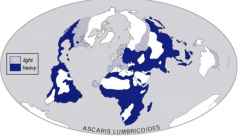
Adult Ascaris lumbricoides - GIANT intestinal roundworm
-most common human helminth globally -soil phase, GI invasion & lung phase -native to areas mapped in this image |
|

The life cycle of what parasite is depicted here?
|
Ascaris lumbricoides - GIANT intestinal roundworm
-most common human helminth globally -soil phase, GI invasion & lung phase -native to areas mapped in this image |
|
|
What are the signs of clinical disease in Ascaris lumbricoides?
|
Giant intestinal roundworm
1. light infections are asymptomatic as long as adult worms do not migrate 2. heavy infection --> a) protein calorie malnutrition - 'failure to thrive' syndrome b) bowel obstruction c) aberrant migratory events d) Loeffler's syndrome -ampula of vater, common duct, liver, pharynx, peritoneum |
|

What disease does this child have?
|
Heavy Ascaris lumbricoides infection
Giant intestinal roundworm |
|

What disease does this child have?
|
Heavy Ascaris lumbricoides infection
Giant intestinal roundworm |
|
What parasite did this person have?
|
Ascaris lumbricoides infection
Giant intestinal roundworm |
|
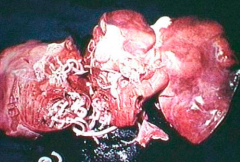
What parasite did this person have?
|
Ascaris lumbricoides infection - IN LIVER - FATAL
Giant intestinal roundworm |
|
What parasite is this?
|
Ascaris lumbricoides infection - EGG
Giant intestinal roundworm Disease is diagnosed by microscopic examination of feces for eggs |
|
What parasite is this?
|
Ascaris lumbricoides infection - fertilized, unembryonated EGG
Giant intestinal roundworm Disease is diagnosed by microscopic examination of feces for eggs |
|

What parasite is this?
|
Ascaris lumbricoides infection - EGG
Giant intestinal roundworm Disease is diagnosed by microscopic examination of feces for eggs |
|
What parasite is this?
|
Larvae of Ascaris lumbricoides in liver (giant intestinal roundworm)
Arrow = larvae |
|

What parasite is this?
|
Larva of ascaris lumbricoides in LUNG
|
|
|
How do you treat ascaris lumbricoides?
|
albendazole (1 dose)*
mebendazole (3 days)* * inhibits polymerization of microtubules which results in depetion of glycogen stores (has no effect on human tubulin) |
|
|
What are the 2 species of hookworms we learned about?
|
-Ancylostoma duodenale
-Necator americanus these are the -2nd most common human helminth globally -soil phase, GI invasion & lung phase |
|
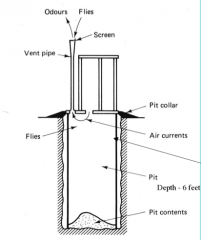
What is the significance of this image as it relates to hookworms?
|
PIT PRIVY
This was the cause of the reduction in distribution & installation began in 1920s following the Rockeffelar Sanitary Commission Report to Congress the height to which a hookworm larvae can crawl is only 4 fee |
|
What parasite is this?
|
- Adult ancylostoma duodenale - HOOKWORM
|
|

What parasite is this?
|
(Adult) Necator americanus - HOOKWORM
|
|
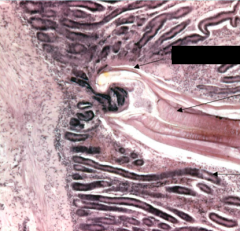
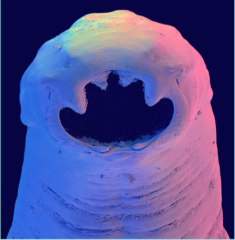
What parasite is this?
|
ADULT HOOKWORM attached to villus of small intestine
- Top arrow = head attached to villus - Middle arrow = muscular esophageal bulb - Bottom arrow = villus Hookworms ingest BLOOD and use powerful ANTICOAGULANTS |
|

This cycle is for which parasite?
|
the hookworms
|
|

What parasite is this?
|
Hookworm as seen on endoscopy
|
|
What parasite is this? What is the clinical disease associate with it?
|
1) Iron-deficiency anemia
2) Failure-to-thrive syndrome - idiopathic endocrinopathy |
|
|
How do you diagnose hookworm?
|
Microscopic examination of feces for eggs
|
|
What parasite is this?
|
Hookworm Egg
Used to diagnose hookworm in feces |
|
What parasite is this?
|
Hookworm Egg
Used to diagnose hookworm in feces |
|

What parasite is this?
|
Hookworm Egg
Used to diagnose hookworm in feces |
|

What parasite is this?
|
Infectious larva of Ancylostoma sp. - hookworm
|
|
|
How do you treat hookworm?
|
albendazole (1 dose)*
mebendazole (3 days)* pyrantel pamoate (3 days) * inhibits polymerization of microtubules which results in depetion of glycogen stores (has no effect on human tubulin) |
|

What parasite is this?
|
Cutaneous larva migrans - A. braziliense - helminth - luminal nematode (but these are babies and never make in all the way into the gut)
-"creeping eruption" on the foot of a patient who stepped on an infective larva - hookworms from young dogs & cats - 2 species: Ancylostoma braziliense & Ancylostoma caninum -fail to penetrate skin -“creeping eruption”= “ground itch” -warm climates |
|
|
How do you treat Cutaneous larva migrans?
|
albendazole (3 days)
ivermectin (1-2 days)* * Binds to glutamate-gated Cl- ion channels in invertebrate muscle and nerve cells causing paralysis and death of the parasite; also acts as an agonist of GABA, disrupting neurosynaptic transmission. |
|

What parasite is this?
|
-this is a free-living female Strongyloides stercoralis - helminth - luminal nematode
-soil phase, GI invasion, lung phase and free-living cycle -Larvae in soil PENETRATE SKIN |
|
What parasite is this?
|
Parasitic female Strongyloides stercoralis
Helminth - luminal |
|
This distribution is typical of what parasite?
|
Strongyloides stercoralis - Helminth - luminal
-Southeastern US and the Appalachia region (esp. eastern Tennessee, Kentucky, & West Virginia) & Puerto Rico -Immigrants, refugees, and military veterans |
|

This life cycle is typical of what parasite?
|
Strongyloides stercoralis
Helminth - luminal |
|
What parasite is this?
|
Strongyloides stercoralis larva in skin
Helminth - luminal |
|
What parasite is this?
|
Strongyloides stercoralis larvae and eggs in bowel
Helminth - luminal |
|
What parasite is this?
|
Strongyloides stercoralis larvae and eggs in bowel
Helminth - luminal |
|
|
What are the clinical symptoms of Strongyloides stercoralis?
|
(helminth - luminal nematode)
-asymptomatic -skin rash/urticaria at entry site (“ground itch”) -pulmonary symptoms (Loeffler’s Syndrome”) -abdominal pain, N&V, diarrhea, dysentery -malabsorption & loss of weight -anemia (ingest blood from intestinal walls) -bacterial sepsis (worms release bacteria/ translocation) -hyperinfection syndrome (HIV/ immunocompromised) with eosinophilia -death |
|

How do you diagnose Strongyloides stercoralis?
|
- microscopic examination of feces x6 (the image is what you might see)
- "string test" - gelatin capsule at end of the string dropped into the stomach - serology (EIA) |
|

What parasite is this?
|
Strongyloides stercoralis - 2nd stage larvae - may be seen in stool for diagnosis
Helminth - Luminal nematode |
|
|
How do you treat Strongyloides stercoralis?
|
ivermectin (2 days)*
albendazole (7 days) * Binds to glutamate-gated Cl- ion channels in invertebrate muscle and nerve cells causing paralysis and death of the parasite; also acts as an agonist of GABA, disrupting neurosynaptic transmission. |
|
|
What are the tissue nematodes?
|
Lymphatic filaria: Wuchereria bancrofti and Brugia malayi cause elephantiasis
Loa Loa: “eye worm” Onchocerciasis: river blindness |
|
What organism is this?
|
Wuchereria bancrofti - tissue nematode
Causes lymphatic filaria, elephantiasis |
|

What causes this?
|
Wuchereria bancrofti and Brugia malayi cause elephantiasis - Lymphatic filaria
These are tissue nematodes |
|
|
What are filariae?
|
-tissue dwelling nematodes with adults and larvae present in human host
-arthropod vector which takes up microfilariae and transmits infectious larvae -lymphatic filariasis, onchocerciasis, Loiasis (Loa Loa) |
|
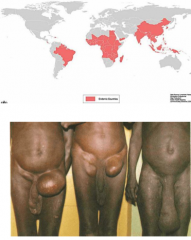
What causes this? What disease is it?
|
Caused by three species of filaria: Wucheria bancrofti, Brugia malayi, B. timori
LYMPHATIC FILARIASIS -High prevalence disease but only a minority of cases results in severe elephantiasis -120 million people infected of which 40 million show symptoms |
|
|
Where is Brugia malayi native?
|
India and China
Causes lymphatic filariasis |
|
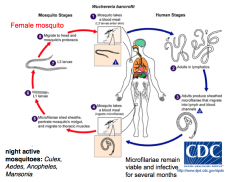
What life cycle is pictured?
|
Wuchereria bancrofti = lymphatic filariasis
Night active mosquitoes: Culex, Aedes, Anopheles, Mansonia Microfilae remain viable and infective for several months |
|

What disease shows this diurnal rhythm?
|
Microfilaria show diurnal rhythm:
-Wucheria and Brugia microfilariae are found in the blood during night time vs. Loa Loa in the day time |
|

What disease is this? What are the clinical findings?
|
LYMPHATIC FILARIASIS
-Bancroftian and Brugian disease is similar - Maturing larvae and adults provoke strong inflammatory reaction - painful lymph nodes, lymphangitis, ulcerations, abscesses, chyluria often accompanied by fever -elephantiasis (thick, hard skin) tends to affect legs > arms (signs after 9mo-1 yr) - bacterial / fungal superinfections contribute to disease progression - unclear what factors cause progression in only minority |
|

What disease is shown in this ultrasound? How do you diagnose this disease?
|
-lymphatic filariasis - nematode infection
-demonstration of microfilaria in blood or lymph (has to be done at night!) -antibody and antigen capture assays (dipstick format) -demonstration of adult worms by ultrasound; dult worms (macrofilariae) live in lymphatic vessels and lymph nodes of the lower body (esp. scrotal hydrocele); dying adult worms cause pathology in lymphatics; worm nest shows as multiple linear echogenic structures within a dilated lymphatic channel suggestive of “filarial dance sign” |
|
|
What are the infectious complications of lymphatic filariasis?
|
edematous lesions between fingers and toes are especially vulnerable to secondary bacterial infection
|
|

What disease is being treated here? What are the treatments for this disease?
|
Lymphatic filariasis
-early disease: albendazole PLUS either DEC (diethylcarbamamazine) OR ivermectin where onchocercaisis is endemic (beware Mazotti reaction) -antiparasitics kill microfilaria and most adult worms if present but NOT helpful for elephantiasis - experimental antibiotic treatment targeting Wolbachia -strict antiseptic regimens using soap and antibacterial ointments can greatly reduce or revert swelling, pain and disease progression |
|
|
What organism causes onchocerciasis?
|
Onchocerca volvulus = nematode
Found in FEMALE BLACKFLY - lives close to fast-moving water = river blindess; fast flowing, O2-rich waters RIVER BLINDNESS filarial nematode progressive inflammatory eye and skin disease 18 million people infected 770,000 impaired vision 250,000 blind West Africa > Central Arica > small areas in America |
|
What life cycle is depicted here?
|
-adult worms (macrofilaria) live in nodules under the skin = onchocercoma
-female releases L1 microfilaria -microfilaria migrate through the dermis and to eye but do not enter blood circulation -female black flies (Simulium) take up microfilaria through the blood meal and develop into infectious L3 larvae |
|

What disease is this?
|
onchocercoma in Onchocerciasis: adult worms form nodules enclosed by a fibrotic granuloma; nematode
-Inflammatory reaction against living macrofilaria is very mild -dead microfilaria stimulate potent inflammatory reactions --> treatment can cause severe allergic reactions - ivermectin --> mild side effects - DEC --> severe side effects! |
|
What disease is this?
|
onchocercoma in Onchocerciasis: adult worms form nodules enclosed by a fibrotic granuloma; nematode
-Inflammatory reaction against living macrofilaria is very mild -dead microfilaria stimulate potent inflammatory reactions --> treatment can cause severe allergic reactions - ivermectin --> mild side effects - DEC --> severe side effects! |
|

What disease is this?
|
skin inflammation associated with ONCHOCERCIASIS, nematode
-unbearable itch provoking scratching --> bacterial infection -depigmentation --> “leopard skin” or hyperpigmentation -loss of elasticity, skin hardening, lichenification, cracking |
|
What disease is this?
|
blindness associated with ONCHOCERCIASIS, nematode
-microfilaria also migrate to the eye -dying larvae cause inflammation -scarring of cornea (sclerosing keratitis), retina and optic nerve |
|

What is being diagnosed by skin snip and corneal biopsy here?
|
ONCHOCERCIASIS
diagnosed by skin snip, corneal biopsy, nodulectomy, serology |
|
|
How do you treat onchocerciasis?
|
- ivermectin --> paralyses microfilariae but doesn’t kill adult worms (successful in mass campaigns)
- repeat every 6 months until asymptomatic - DEC: contraindicated (can induce blindness) - spray with larvacides |
|
What disease is found in this peripheral blood smear?
|
Loa Loa, African eye worm; tissue nematode
|
|
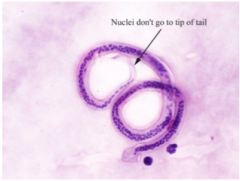
What disease is this?
|
Loa Loa, African eye worm; tissue nematode
- Left arrow = nuclei at tip - Right arrow = sheath - this is a wright-giemsa stain |
|

What parasite group is this?
|
Tissue nematodes!
1. Wuchereria bancrofti: Sheath, no nuclei in the tip of the tail 2. Brugia mal Sheath, 2 distinct nuclei in the tip of the tail 3. Loa: Sheath, nuclei extending to the tip of the tail 4. Onch volvulus (skin) No sheath, no nuclei in the tip of the tail 5. Mansonella perstans: No sheath, nuclei extending to tail 6. Mansonella ozzardi : No sheath, no nuclei in the tip 7. Mansonella streptocerca (skin): No sheath, nuclei the tip of the hooked tail |
|
What disease is this? Does it effect vision?
|
Loa Loa: African eye worm, tissue nematode
microfilariae under conjunctiva; does NOT effect vision |
|

What disease is carried by this deerfly/mango fly? Do they feed day or night?
|
Loa Loa: African eye worm, tissue nematode
Feed during the day! |
|

What disease is this?
|
Loa Loa: African eye worm, tissue nematode
Causes: migratory (2-4d) subcutaneous swellings (Calabar swellings) associated with pain & fever allergic response to filarial waste products |
|
|
How do you diagnose and treat Loa Loa?
|
Loa Loa: African eye worm, tissue nematode
Diagnosis -blood smear (daytime) -identify worm in skin or eye -serology -eosinophilia Treatment -surgical removal -DEC (exclude onchocerciasis) -albendazole (do not use ivermectin) |
|
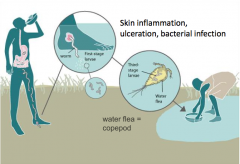
The life cycle of what parasite is depicted here?
|
Guinea worm; tissue nematode
Causes skin inflammation, ulceration, bacterial infection Is ingested and then crawls out through feet This will be the first disease to be eradicated without a vaccine or medication |
|

What parasite/disease is this?
|
Guinea worm; tissue nematode
It is crawling out of his foot |
|

What parasite/disease is this?
|
Guinea worm; tissue nematode
Extracting the guinea worm from the heal |
|
|
Where is guinea worm found?
|
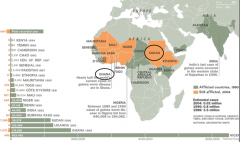
Sudan, Ghana, Niger & virtually nowhere else
|
|

What disease life cycle is this?
|
Trichinosis - Trichinella spiralis - tissue nematode
Clinical: most: asymptomatic fever myalgia/myositis encephalitis Diagnosis: Eosinophilia serology Treatment: albendazole or mebendazole |
|
|
What are the visceral larva migrans species?
|
Toxocara canis
Toxocara cati Animal nematodes |
|
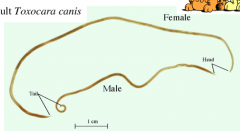
What organism is this?
|
Adult Toxocara canis
Cause visceral larva migrans Animal nematode |
|
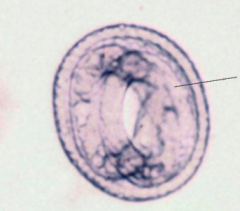
What organism is this?
|
Embryonated egg of Toxocara canis - visceral larva migrans - animal nematode
Puppies/kittens contaminate environment (eggs are NOT in human stool) |
|
|
What are the clinical features of visceral larva migrans?
|
-most: asymptomatic
-fever -hepatitis -pulmonary symptoms -carditis (myocarditis) -retinitis-->visual changes: ocular larva migrans -hypereosinophilia |
|
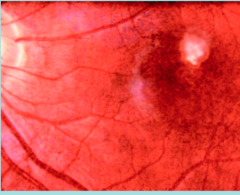
What organism is this?
|
Granuloma in retina due to Toxocara canis
visceral larva migrans - animal nematode |
|
|
How do you diagnose Toxocara canis? How do you treat and prevent it?
|
ELISA-based serological tests
-albendazole or mebendazole -sanitary disposal of dog & cat feces -periodically deworm pets -cover sandboxes at night |
|

What parasite is this? What disease?
|
Caused by Larvae (maggots) of bot fly, tumbu fly & screwworm fly
Myiasis Treat with vaseline and surgical removal |
|
|
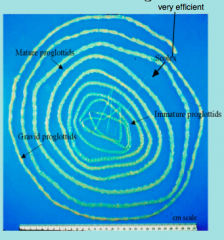
What are the species of tapeworm?
|
Cestodes: tapeworms
Taeniasis=GI tapeworm infection Taenia saginata (beef tapeworm) --> human Taenia solium (pork tapeworm) --> cystercercosis (human invasion + tapeworm) Echinococcus granulosus (dog) --> hydatid disease --> human invasion |
|
|
What are the definitive and intermediate hosts of T. saginata and T. solium?
|
T. saginata - definitive host = human, intermediate host = cow
T. solium - definitive host = human, intermediate host = pig, human |
|
What parasite is this?
|
Adult taenia saginata = cow tapeworm
|
|

What parasite is this?
|
Adult taenia solium = pig tapeworm
|
|
What parasite is present here?
|
LEFT = taenia saginata = cow tapeworm, larvae/cysts
RIGHT = taenia solium = pig tapeworm, larvae/cyst |
|
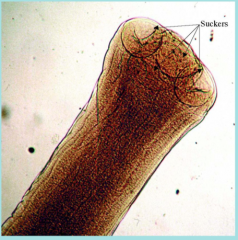
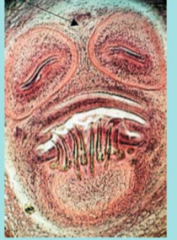
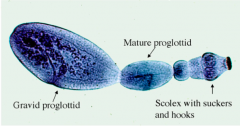
What parasite is this?
|
Taenia saginata
Scolex with suckers |
|

What parasite is this?
|
Taenia solium scolex
|
|

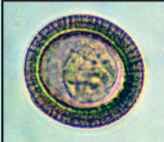
What parasite is this?
|
Taenia solium or taenia saginata eggs - can't tell the difference from just looking
|
|
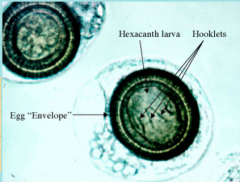
What parasite is this?
|
Taenia solium or taenia saginata eggs - can't tell the difference from just looking
|
|

What parasite is this?
|
Taenia solium or taenia saginata eggs - can't tell the difference from just looking
|
|
|
How do you diagnose taenia solium/saginata?
|
1) Find eggs or proglottids in stool
2) Identify species based on proglottid morphology, after formalin and India ink 3) Identify scolex |
|
What parasite is this?
|
Taenia solium or taenia saginata eggs - can't tell the difference from just looking
|
|
|
How do you treat Taenia solium or taenia saginata?
|
Praziquantel
Mode of action - increases permeability of flatworm tegument to Ca2+ ions, causing muscle tetany and worm detachment |
|
|
How do you prevent and control taenia saginatia infection?
|
- prevent cows from coming into contact w/ human feces, ie good sanitation and physical restraints
- freeze and/or cook all beef until well-done - federal meat inspection programs |
|
|
How do you prevent and control taenia solium infection?
|
- good sanitary practices on pig farms
- federal meat inspection programs - cook and/or freeze pork products thoroughly - treat pigs or vaccinate pigs, using new oncosphere mRNA vaccine, in eradication programs |
|
|
What parasitic disease causes brain seizures? How is it transmitted?
|
cysticercosis - taenia solium - pig tapeworm
brain --> seizures (space occupying lesion &/or inflammatory response) also --> eye, subcutaneous cysts - ingestion of T. solium eggs (not T. saginata) from someone else’s or ones own (autoinfection) tapeworm infection; i.e. not from eating infected pork! - people who don’t eat pork can get cysticercosis by ingesting food or water contaminated by an infected food preparer (e.g. orthodox Jews in NY outbreak) |
|
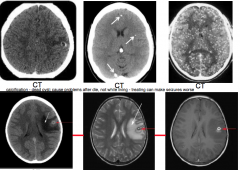
This head imaging shows what disease?
|
Neurocysticercosis from taenia solium, pig tapeworm
|
|

What parasite is this?
|
Taenia solium, cysticercosis of the eye
Cysticercus near optic near, mis-diagnosed as retinoblastoma; |
|
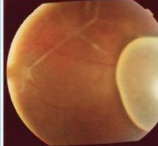
What parasite is this?
|
Taenia solium, cysticercosis of the eye
Cysticercus near optic near, mis-diagnosed as retinoblastoma; |
|
What parasite is this?
|
Taenia solium, cysticercosis of the eye
|
|

What parasite is this?
|
X-ray of leg with numerous calcified cystercerci of Taenia solium
|
|
|
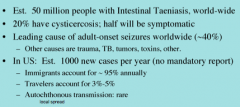
What is the clinical epidemiology of Cysticercosis?
|

|
|
|
What are the clinical findings in cysticercosis?
|
taenia solium, pork tapeworm
-asymptomatic -CNS: headaches, seizures*, hydrocephalus, paralysis -visual disturbance -lumps under the skin * major cause of adult onset seizures in low-income countries (caused by dying and calcified cysts) |
|
|
How do you diagnose cysticercosis?
|
-serology: blood, CSF (EIA or immunoblot)
-brain imaging: CT, MRI -ophthalmology: eye exam -stool: Taenia solium eggs and proglottids in the feces diagnoses taeniasis and not cysticercosis. -serology screening: persons who are found to have eggs or proglottids in their feces should be evaluated serologically since autoinfection, resulting in cysticercosis, can occur. |
|
|
How do you treat cysticercosis?
|
-depends on number of cysts, location and stage of infection (viable, degenerating, or calcified/dead)
-no anti-parasitic treatment for dead cysts -treat viable cysts with albendazole x 15-30 days (or praziquantel) plus steroids x few days (dexamethasone) to counteract the inflammatory edema induced by dying cysticerci (controversial) -anticonvulsants if needed -eye examine before starting therapy surgery (eye, brain) in some settings |
|
|
What disease is caused by echinococcosis?
|
Hydatid disease in humans
Dog tapeworm Definitive host = dog; intermediate host = sheep, human |
|
|
Sheep husbandry leads to what tapeworm disease?
|
Echinococcosis - hydatid disease
Dog tapeworm Found in America, Mexico, South America, Asia, Europe |
|
What parasite is this?
|
Adult Echinoccocus granulosus
hydatid disease Dog tapeworm |
|
|
What is the distribution of hydatid cysts in the body?
|
Liver - 63%
Lungs - 25% Muscles - 5% BM - 3% usually fatal Kidney - 2% Spleen - 1% Brain - 1% (usually fatal) |
|

What parasite is this?
|
Echinoccocus granulosus
hydatid disease Dog tapeworm |
|
What is this a diagram of?
|
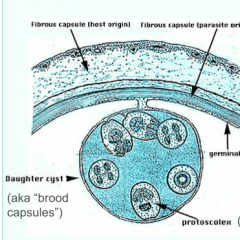
Hydatid Cyst
Echinoccocus granulosus Dog tapeworm |
|
What parasite is this?
|
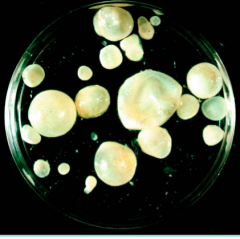
Hydatid Cyst
Echinoccocus granulosus Dog tapeworm |
|
What parasite is this?
|
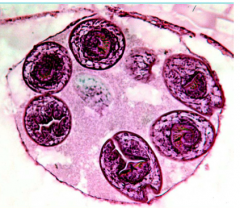
Hydatid Cyst - daughter cysts
Echinoccocus granulosus Dog tapeworm |
|
What parasite is this? What disease?
|
Echinoccocus granulosus
Dog tapeworm "Hydatid sand" which comes out of the daughter hydatids |
|
|
What are the clinical findings of hydatid disease?
|
1. When intact, it may be IMMUNOLOGICALLY and CLINICALLY silent, especially in liver
2. In other organs, it is a space-occupying lesion 3. It may leak or rupture, seeding adjacent areas 4. When ruptures --> allergic reactivity & anaphylaxis ensues; can be fatal |
|
|
How do you diagnose hydatid disease?
|
NO BIOPSY
Direct microscopic exam of fluid from hydatid after removal to look for hydatid sand Indirect - ELISA, MRI, CAT, x-ray, accurate case history |
|
|
How do you treat hydatid disease?
|
Surgical, whenever possible (liver > 10cm, brain, lungs, kidney)
PAIR Technique for liver lesions - puncture, aspirate, inject, re-aspirate Pharmacologic has <50% success = Albendazole, 1-6 months |
|
|
How do you prevent the spread of hydatid disease?
|
1) reguarly treat all dogs with niclosamide that have contact w/ sheep; this kills adult parasites
2) avoid feeding hydatid cyst material (sheep offal) to dogs 3) public health education of sheep farmers |
|
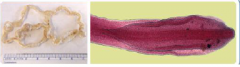
What parasite is this? What disease does it cause?
|
Diphyllobothrium latum = fish tapeworm
-ingestion of eggs from raw freshwater fish in northern hemisphere -can cause vitamin B12 deficiency--> anemia -treat with praziquantel |
|
|
What causes Schistosomiasis? Where is it found?
|
Blood fluke living in snails in water
-blood fluke -fresh water snails are the intermediate hosts -humans are definitive hosts -clinical disease related to parasitaemia, location of eggs in various organs, and to adult worms in ectopic sites. South America, Africa, China = S. mansoni/S. japonicum Urinary = Africa, India, Middle East Fishing/bathing are high risk sites |
|

What parasite is this? What disease does it cause?
|
Schistosoma mansoni - blood fluke
effects GI/liver |
|

What parasite is this? What disease does it cause?
|
Schistosoma haematobium (B = bladder!) - blood fluke
Bladder disease |
|

What parasite is this? What disease does it cause?
|
Schistosoma haematobium - blood fluke
Liver/GI in limited areas |
|

What parasite is this? What disease does it cause?
|
Miracidium of SCHISTOSOMA MANSONI caught in the act of hatching
Causes GI/liver disease |
|

What is this? What parasite does it carry?
|
Biomphilaria glabrata, the most common intermediate snail host of Schistosoma mansoni
|
|

What parasite is this? What disease does it cause?
|
Cercaria of SCHISTOSOMA MANSONI
|
|
|
What causes swimmer's itch?
|
SCHISTOSOMA MANSONI
|
|
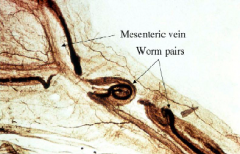
What parasite is this? What disease does it cause?
|
Adult flukes in schistosomiasis
Female resides inside male's gynecophoric canal |
|
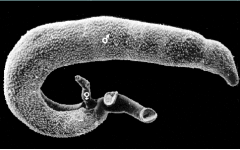
What parasite is this? What disease does it cause?
|
Adult flukes in schistosomiasis
Female resides inside male's gynecophoric canal |
|
What parasite is this? What disease does it cause?
|
Schistsome egg in tissue of small intestine = SCHISTOSOMA MANSONI causes Schistosomiasis
Note intense granuloma |
|
What parasite is this? What disease does it cause?
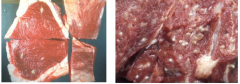
|
Pipe stem fibrosis in liver due to heavy infection with Schistosoma mansoni; note normal liver tissue next to fibrotic vessels
|
|
What parasite is this? What disease does it cause?
|
Pipe stem fibrosis in liver due to heavy infection with Schistosoma mansoni; not surrounding eggs
Schistosomiasis |
|
|
What are the signs of acute and chronic clinical disease in schistosomiasis from schistosoma mansoni?
|
Acute phase: katayama fever, paralysis, CNS involvement
Chronic phase: 1) GI bleeding and diarrhea 2) portal hypertension due to blockage of pre-sinusoidal capillaries 3) esophageal varices 4) ascites 5) rupture of varices, bleeding, death 6) Cor pulmonale, right side heart failure, death 7) Toxic brain syndrome |
|
What disease is this?
|
Advanced schistosomiasis - ascites, splenomagaly, collateral circulation, schistosomal dwarfism
|
|
What are the complications of bladder schistosomiasis?
|
1) Squamous cell epithelioma / squamous cell carcinoma
2) Calcification of dome of bladder due to accumulation of dead eggs 3) Hydronephrosis |
|
What complication of bladder schistosomiasis is shown here?
|
Hydronephrosis
|
|
|
How do you diagnose bladder schistosomiasis?
|
1) Microscopic examination of feces, urine, rectal 'snip' for eggs
2) Capture ELISA for detecting circulating antigens (experimental) 3) serological tests (ELISA etc): indirect measure of exposure, not active disease |
|
|
How do you treat schistosomiasis? What encourages transmission? How do you prevent schistosomiasis?
|
Praziquantel - increases permeability of flatworm tegument to Ca2+ ions, causing muscle tetany and worm detachment
Transmission is encouraged by: 1) dam building, irrigation projets (e.g., 3 Gorges Dam, China) 2) Reservoir hosts (primates, oxen) 3) Indiscriminate dispersal of feces and urine into environment Prevent with: mass drug administration with praziquantel in hi risk groups, snail control & environmental management, health education, sanitation, safe water, economic development |
|

What organism is this?
|
Clonorchis sinensis = Chinese liver fluke
-eating raw/undercooked infected fish -biliary tract inflammationpigmented gallstones -associated with cholangiocarcinoma |
|
|
What organism is spread by ingestion of raw/pickled/undercooked freshwater crap or crayfish?
|
Paragonimus westermani
Oriental lung fluke -ingestion of raw/pickled/undercooked infected freshwater crab or crayfish -chronic infection may mimic pneumonia or TB with hemoptysis, chest pain, lung cyst/cavity -Rx: praziquantel |
|
|
What does 50c/person/year buy?
|
“Rapid impact package” of 4 drugs:
1) albendazole or mebendazole = ascariais, hookworm, trichuriasis 2) DEC or ivermectin = lymphatic filariasis (elephantiasis), onchocerciasis (river blindess, avoid DEC) 3) praziquantel = schistosomiasis from flukes 4) azithromycin = trachoma (Chlamydia, blindness) also covers nematode (strongyloides), cestode (tapeworms), trematodes (flukes!), scabies (ivermectin) |