Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
87 Cards in this Set
- Front
- Back
|
Whyis it important to know sacral really well?
|
it's very heavily tested on the boards
|
|
|
What is the model of sacral mechanics that we teach and that will be tested? Why?
|
The mitchell model because it works clinically
|
|
|
What does sacrum mean?
|
"sacred"
|
|
|
When does the 5 sacral bones fuse?
|
between 16 and 26
|
|
|
How much stress is the sacrum under and what is it held up by?
|
an incredible amount because it holds up the whole upper body and is only held in place by the ilium
|
|
|
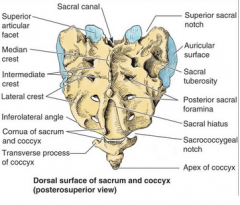
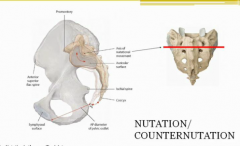
What is the sacral promontory?
|
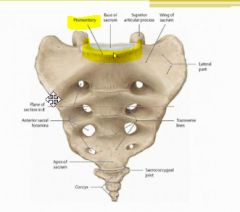
the most top, disc-like part of the sacrum
|
|
|
What part Of the bone do we always named dysfunctions for?
|
The direction that the top of the bone is going in.
|
|
|
So what are sacral dysfunctions named for?
|
what the promontory is doing
|
|
|
Imagine what the sacrum looks like from the side. What shape is the sacroiliac joint in?
|
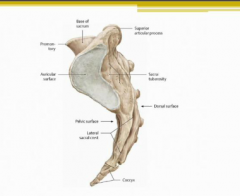
The sacrum looks like a curved bone to the shape of your but. The sacroiliac joint like a C headed in the opposite direction
|
|
|
Where do all the Coccxygeal nerve roots come out of?
|
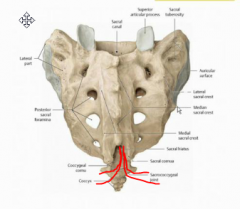
The sacral hiatus
|
|
|
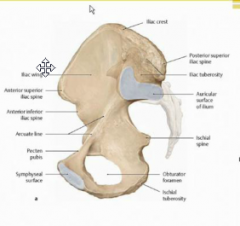
From the front, what are some differences between the male and female pelvis?
How can you visualize what is happening if you wanted to turn the male pelvis into the female? |
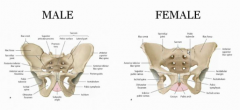
1. The pubic arch is much wider on a female
2. The iliac crests are much broader and wider on a female as well You would pull all the prominences outward (iliac crests, ischial tuberosities, sacral promonence) |
|
|
From the top, what are some differences between the male and female pelvis?
How can you think about the shape of the whole pelvis? |
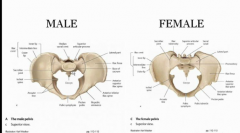
1. The female pelvic brim is oval-shaped whereas the males is somewhat heart-shaped because the sacrum kind of impinges on the space
on top, there is a big semi bowl facing front. on the back, there is a smaller semiibowl facing the back. |
|
|
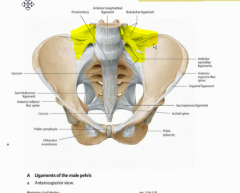
Now we talk about the ligaments of the sacroiliac joint.
What does the end of your anterior spinal ligament looks like? How far does the anterior sacral iliac ligament go? Why? |
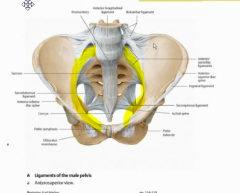
The anterior spinal ligament covers all the way down to the coccygeal but narrows in between the foramen.
The anterior sacroiliac ligament goes in almost a complete ring around the pelvic brim ending just short of the pubic symphysis |
|
|
WHat is the ilio lumbar ligament? Why is it clinically relevant?
|
It is the strong set of ligaments that attaches L4, L5 to the iliac bone.
It is clinically relevant because there are a lot of pain receptors here that are responsible for back pain in the case that they are sprained |
|
|
|
|
|
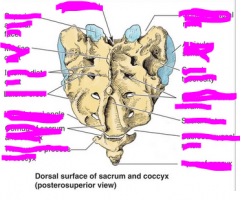
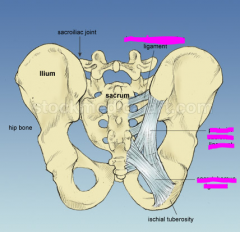
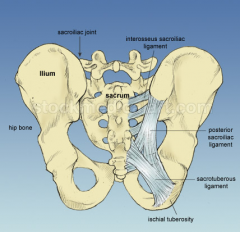
Dissect the meaning/ attachments of these following ligaments:
1. Sacral tuberous ligaments 2. posterior Sacroiliac ligaments 3. Interosseous sacroiliac ligaments |
1. Sacral tuberous ligaments - from sacrum to ischial tuberosity
2. Posterior Sacroiliac ligaments- from PSIS to sacrum 3. Interosseous sacroiliac ligaments- a bunch of tiny ones from each sacral level to the iliac |
|
|
|
|
|
What is the relationship between the posterior sacral iliac ligament and the sacral tuberous ligament?
What point of the sacrum do they both touch? |
They actually act as one long continuous ligament from the PSIS to the ischial tuberosity and connecting to the sacrum at the inferior lateral sacral angle
|
|
|
What muscles attach to the posterior sacrum? Name what fascia are involved.
|
1. gluteus maximus vis thoraco lumbar fascia
2. multifidus |
|
|
What muscles attach to the anterior sacrum? Name what fascia are involved.
|

1. piriformis
|
|
|
SO why do we need to know these muscles?
|
in case we need to use muscle energy to pull the sacrum forward or backwards
|
|
|
Where along that the spinal canal is the dura attached?
What does this explain? |
At the OA, AA, and very upper cervicals and then S2 where the meningeal sac ends.
This explains why you can feel a stratching of the dura when you move your head or legs |
|
|
What is unique about the dorsal root ganglia on location in the sacrum?
|
They are encased within the sacrum
|
|
|
Show how the sacrum sits on the pelvis from a side view.
What is the main motion that the sacrum can go through? |
The sacrum since almost horizontally on the pelvis.
It's main motion is rocking |
|
|
Describe the composition of the sacroiliac joint anteriorly and posteriorly
|
It is a fibro cartilaginous joints anteriorly and a synovial joint posteriorly
|
|
|
What model of naming sacral motion do we use? Dissect the name.
What structures motion is it based off of? |
We use nutation/counternutation which is based off the motion of the promontory and means "to nod"
|
|
|
Show nutation.
What level is the axis you base it on? What action does your sacrum do when you inhale? Why? |
It will counter nutate because you are pulling the whole spine up and it will straighten out of its kyphosis.
axis at S2. |
|
|
What is the oblique axis of sacral motion?
When do we use this axis vs when do we use nutation? |
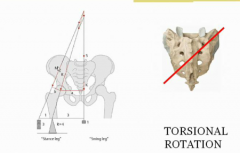
torsional rotation for walking
we use nutation/cn all the time because we breath. |
|
|
Where does the vector of force go through the sacrum and femur when you are standing on one leg?
|
Through the SI joint and the head of the femur
|
|
|
At what point of our gait do we rotate around the torsional axis?
What gets locked in and what is free to move on the sacrum? For which direction is the axis named? |
When one leg is on the ground and the other one is off the ground.
The sacroiliac joint of the leg on the ground is locked in whereas the joint of the leg moving is rotating the sacrum The is named for the upper SI joint which is locked in (right versus left) |
|
|
What kind of sacral rotation would you have when you are swinging your left leg?
What structure are you basing this naming off of? |
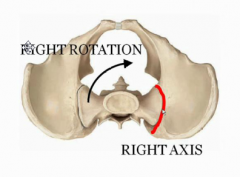
Right rotation because the sacral promontory is rotating to the right
|
|
|
What rotation would you have swallowing your left leg backwards?
|
You would have left rotation of the sacrum
|
|
|
What is the proper naming for sacral dysfunction?
|
SI joint that is moving (rotaion) on SI joint that is locked (axis)
|
|
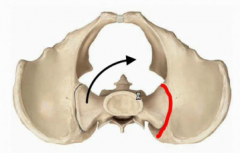
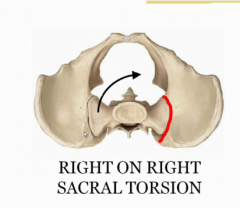
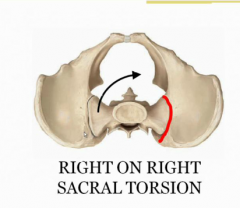
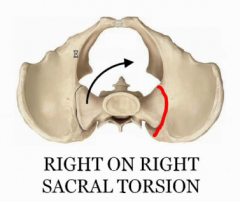
Name this
|
Right on right sacral torsion
|
|
|
What are anterior versus posterior sacral torsion? Why?
Give the nomenclature |
Right on right and left arm left our anterior sacral torsions because you are moving your leg forward with them.
|
|
|
Which torsions are physiologic versus non-physiologic? And why?
|
Only anterior portions are physiologic because they occur normally during gait
|
|
|
What muscle would you use to treat anterior Versus posterior sacral torsion?
|
Gluteus maximus for anterior
Piriformis for posterior |
|
|
What is the relationship between L5 and the sacrum in terms of flexion/extension?
What other bony pair does this remind you of? |
They are always opposite to one another because they push on one another much like the manubrium and the Gladiolus
|
|
|
So what direction with your sacrum go when you bend it to touch your toes?
|
Your sacrum would be in counter nutation
|
|
|
How does the sacrum matchup with L5 in terms of side bending?
|
It goes to the same side because it drags it along
|
|
|
What kind of sacral dysfunction would you get if you had L5 SLRL?
|
Right on left sacral torsion
|
|
|
What two things must you treat before you treat the sacrum?
|
L5 and inominnts dysfunction To make sure that it isn't responsible for the dysfunction
|
|
|
What should you imagine happening to be sacrum when the L5 is side bends and rotated to a certain side?
|
The side that it is sidebending towards is the joints that is locked in
The side that it is rotating is the joint that is moving forward |
|
|
If L4-5 is SRRL what is the sacral dysfunction?
|
Right on right sacral torsion
|
|
|
Now we talk about sacral shear. Is this common? What is it usually caused by?
|
It is always pathological and very uncommon. It's usually related to trauma
|
|
|
What motion is sheer incredibly similar to? In what ways?
|
It is based off of flexion/extension a.k.a. nutation/counternutation.
It is named for the promontory and goes around the transverse access of S2 |
|
|
What categories you have to put in when naming sacral sheer?
|
The direction, whether it is one side or both, whether it is forward or backwards
|
|

Name this.
|
|
|
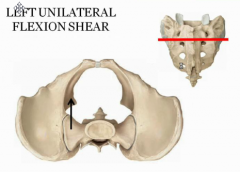
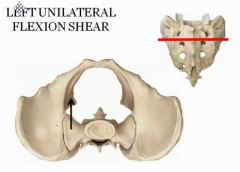
What would move forward versus backwards versus staying neutral in this dysfunction?
|
The left SI will move anteriorly
the right SI will a neutral the left inferior lateral sacral angle will move posteriorly |
|

Give two names for this dysfunction
|
Bilateral extension shear
stuck in counter nutation |
|
|
Where would you apply force to treat flexion versus extension shears?
What is this similar to treating? |
Treated like a seesaw like the Gladiolus.
If it is in flexion apply force to the apex to rotate the sacrum back. If it is in extension apply force to the base at the top of the sacrum to make it go into nutation |
|
|
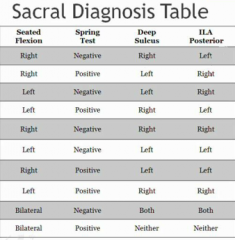
How many things Can we test for to make a diagnosis?
How many of them we need? |
We need three out of four possible pieces of information
|
|
|
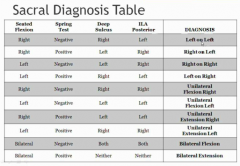
Can you list the four tests that we can do?
|
1. Seated flexion test
2. Spring test a.k.a. sphinx test 3. Sacral sulcus depth 4. Inferior lateral angle position |
|
|
In the seated flexion test, why is the side that moves first the side of the dysfunction?
What is the normal order of movement when you bend forward ? |
Your lumbar is supposed to fully lockout before the pelvis rotates forward. If there is tightness, the SI joint will lock earlier and rotate the pelvis earlier.
|
|
|
Give a step By step guide on how to do the seated flexion test.
Where should your eyes be? |

1. Put your thumb on the PSIS
2 have the patient bend forward starting with the thoracic slowly rolling to the lumbar 3. Check to see which side earlier (which side "ask for help earlier") make sure eyes are level with your thumb |
|
|
What information does the seated flexion test give us? What information doesn't not give us?
|
It tells us which side had a rotational dysfunction, but does not tell us what direction that dysfunction is in
|
|
What side would be positive on the seated flexion test here?
|
The left side because this is the side that is rotated
|
|
What side would be positive on the seated flexion test here?
|
The right side because this is the side that is rotated
|
|
|
Can the seated flexion test detect shear dysfunction as well?
|
Yes, but again it cannot detect that the direction
|
|
|
How can you use the seated flexion test to see if you have a bilateral Shear?
|
If you are thumbs start moving before the lumbar spine is fully flexed
|
|
|
What should you be doing during the spring test?
What position should the patient be in? |
You should be pressing down on the sacrum directly to see if it springs up.
The patient should be in the Sphinx position |
|
|
What should you feel in a positive spring test?
What dysfunction does this indicate? |
No recoil upon direct compression
This means that the sacral base is displaced posteriorly, which means it already rotated in the direction that you are pressing it down so there is no normal to "spring back to" |
|
|
What should you feel in a negative spring test? Does this indicate a dysfunction?
|
You should feel a spring upon compression. This means that the sacrum is displaced anteriorly at the base
|
|
|
What information does the spring test give you?
What information does it not give you? |
It tells you if the sacrum is stuck anteriorly or posteriorly but does not tell you if it is left or right doing it
|
|
What kind of spring test would you get for this dysfunction?
|
A negative spring test because it is displaced anteriorly so it will spring
|
|
|
How would you test for the sacral sulcus?
|
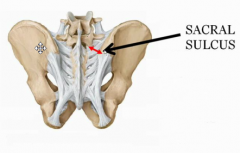
You put your thumb just medial to the PSIS and see how far down you can press
|
|
|
How would you describe the sacral sulcus on a right on right sacral torsion?
|
It would be deep on the left
|
|
|
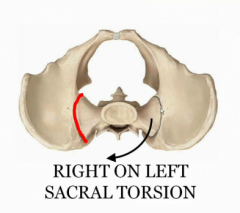
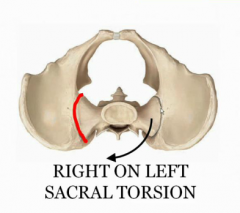
How would you describe the sacral sulcus on the left on right sacral torsion?
|
It would be shallow on the left
|
|
|
Upon palpation, do you know which sacral sulcus is shallow/deep versus neutral?
|
No, one usually feels deeper than the other but you don't know if it actually deep or if the other one is just shallow.
|
|
|
How do you test for the inferior lateral angle (ILA) posterior?
|
You feel for the ILA and see which side is more posterior
|
|
Try a couple of these.
|
|
|
|
Is spring testing of the sacral sulcus and inferior lateral angle following the same logic as lumbral sacral spring testing?
|
No, if those things are displaced deep/anterior, they will tend to spring more because you are putting them more in the direction of their dysfunction. (From OMT review)
|
|
|
What is the axis of rotation for each shear dysfunction?
|
The transverse access along S2. So the top and the bottom of the sacrum should move in opposite directions
|
|
|
Which part of the bone is dysfunction usually named for?
|
the most anterior and superior part.
|
|
|
can spring test vary with torsions? How?
|
yes, a forward torsion is negative spring test (does spring)
a backwards torsion is positive spring test |
|
|
how can you tell a backwards from a forwards torsion in the naming?
|
if they are different, (left on right) then it is backwards
|
|
|
what can you do to visualize how the sacrum moves in your hands?
|
use a flexible rectangle like a piece of paper and move it about the axis
|
|
|
where are you pressing for the spring test?
|
between L5 and the sacrum
|
|
|
why would the spring test work in flexion?
|
you are pusing the top of the sacrum more into the direction of dysfunction
|
|
|
If you are leaning on your left leg to shovel snow and then throw out your back, what is the dysfunction??
what part of the back will the pt complain of> |
right on left
people will complain they threw their right back out |
|
|
what if you bent down to pick something up with both hands and throw your back out? dysfunction?
|
bilateral extension because you lumbar is flexed
|
|
|
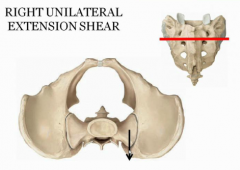
What in you just picked up a suitcase with one hand and threw your back out? dysfunction?
|
unilateral extension
|
|
|
how can you shear just one side of the sacrum which is one big bone?
|
you technically can;t, but this is the mitchell model that works
|
|
|
how can you think about what is actually happening?
|
there is disturbed forces being placed on the sacrum in the direction of the dysfunction (muscles pulling it)
the bone is not actually moving! |
|
|
how common are unilateral shears?
|
not common
|
|
|
what are the most common dysfunctions?
|
the physiologic ones (anterior torsion)
|
|
|
What are a little more common than unilateral shears, but still kind of uncommon?
|
posterior torsions.
|