Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
143 Cards in this Set
- Front
- Back
|
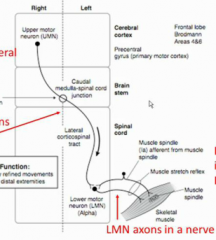
Show the control of reflex sensory fibers and UMN's on LMN activity.
|
|
|
|
When do the UMN exert their inhibitory effect on a reflex?
|
After one reflex contraction, they inhibit the LMN's.
|
|
|
The subcortical spinal tracts control which kinds of muscles?
|
trunk muscles
|
|
|
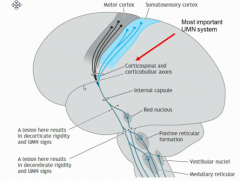
Can you show a pic of the corticospinal vs subcorticospinal tracts? (subcortical intitiated from cortical collaterals)
|
|
|
|
WHat happens if you have a lesion of one side of a corticospinal vs subcortical spinal tract? Why?
|
corticospinal- contralateral motor deficits
subcorticalspinal- no noticable deficits because they innervate trunk muscles bilaterally so the other side can compensate |
|
|
Does the rubber mat or ViP only control flexor/extensors?
|
No they are biased towards f/e, but they can do both.
|
|
|
DO we have to consider the accessory motor pathways extensively? Why?
|
No because they are poorly understood and also compensate for one another because they have bilateral innervation.
|
|
|
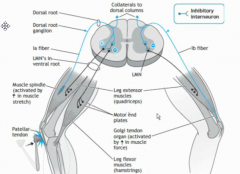
Is the agonist muscle in a tendon stretch reflex the only muscle affected by the reflex arc? What other pathway happens?
|
No, the antagonist is inhibited via inhibitory interneurons.
|
|
|
Show a picture of the activating and inhibitory pathway in a muscle stretch (myotactic) reflex.
|
|
|
|
Is there an inhibitory interneuron present in the GTO reflex? WHat is the general rule?
|
Yes! Anytime you need to relax a muscle reflexively, there is an inhibitory interneuron involved.
|
|
|
What is an alternate name for the GTO reflex?
|
inverse muscle stretch reflex.
|
|
|
NOW WE TALK ABOUT COMMONLY TESTED NEUROLOGICAL SIGNS!
|
CLINICALERIFFIC!
|
|
|
essentially what neurons are we trying to test for when we test a DTR?
|
all UMN's above it and the LMN at that level feeding that muscle.
|
|
|
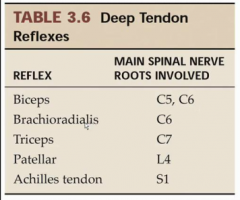
Give the chart of what spinal level each DTR tests. (5)
|
|
|
|
What nerve is being tested in the patellar reflex? Which spinal roots come out to make this giant leg nerve?
|
The femoral nerve created by L2-L4
|
|
|
What nerve is being tested in the achilles tendon reflex? Which muscles does it innervate?
|
The posterior tibial nerve innervating the calf muscles (gastrocnemius and solieus)
|
|
|
What is he scale for grading muscle strength? What is 0?
|
0/5-5/5
0 is paralysis |
|
|
Are people with UMN lesions going to have weakness? Why?
|
Yes because they have lost part of their ability to tell that muscle what to do. (nevermind that it is tense and hyperreflexive on its own)
|
|
|
What is he scale for grading muscle reflex? What is 0?
|
0-4+
0 is no reflex |
|
|
What kind of grade would a person with a LMN lesion vs UMN lesion get on DTR's? Normal?
|
LMN- 0
UMN- 4+ Normal- 2+ |
|
|
How would you use words to describe a DTR that is 2+?
|
Normal, moderately brisk
|
|
|
What is clonus?
|
repeated reflex contractions after a stretch
|
|
|
When does fasiculations vs atrophy come about in a severe LMN lesion?
|
fasiculations- early manifestation (during anterograde LMN degeneration)
atrophy- late manifestation |
|
|
What are the clinical terms to define the type of weakness in LMN vs UMN lesions?
|
LMN- flaccid paralysis
UMN- spastic paresis (weakness) or paralysis (total loss of movement) |
|
|
What does pathognomonic mean?
|
A sign that indicates a certain disease beyond a doubt
|
|
|
What is a positive babinski's sign pathognomic for?
|
an UMN lesion
|
|
|
What is the meaning of phyte?
|
something that grows on something else
|
|
|
Give a medical and ecological example of the usage of -phyte.
|
osteophyte- bone grwoth
saprophyte- fungus that grows of dead or decaying matter. |
|
|
A person is weak. Do they have UMN or LMN lesion?
|
You don't know. It could be either.
|
|
|
How can you find out if it is LMN or UMN?
|
do a DTR test
LMN- areflexia UMN- hyperreflexia/clonus |
|
|
Is tone and reflexivity always in the same direction?
|
yes
|
|
|
What happens if you have untreated carpal tunnel syndrome for a long time?
|
the median nerve will degenerate and then the muscles of the hand will atrophy
|
|
|
What sign happens before degeneration in a LMN lesion?
|
fasiculations
|
|
|
Do we know how fasiculations happen physiologically? What do they look like?
|
Like a bunch of muscle twitches. (no one really knows why so Dr. Najeeb was just making a plausible explanation)
|
|
|
Why does a UMN lesion usually just result in paresis rather than paralysis?
|
Because there are accessory UMN's (extrapyrimidal) to help with conrol of the muscle
|
|
|
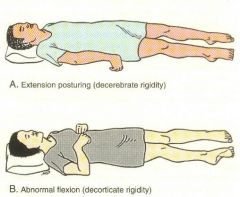
Show a picture of decorticate vs decrerebate rigidity/posturing.
|
|
|
|
What kind of subcortical collateral lesion would result in decorticate or decerebate posturing? WHy?
|
the one to the red nucleus because this controls wrist muscles for support.
|
|
|
What determines if a pt with a UMN lesions will have paresis or paralysis?
|
the extent of the damage
|
|
|
TIME TO TALK ABOUT THE CEREBELLUM
|
lovely
|
|
|
What is the main 3 functions of the cerebellum?
|
1. To promote the smooth execution of muscle movements (fine tuning)
2. To plan muscle movements 3. Motor learning |
|
|
What does it prevent?
|
1. Fine tuning function- jerky movements
2. Planning- something else (can't think of it) |
|
|
How does the cerebellum do these things on a general level?
|
by comparing the intended movement (corticopontine) with the actual movement (spinocerebellar)
|
|
|
Show the vermis and how deep down the cerebellum it goes.
|
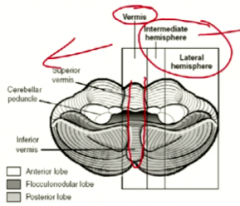
not just the cortex!
|
|
|
What muscles does the vermis vs paravermis/intermediate hemisphere control?
|
vermis- axial and proximal limb movements
paravermis- distal limb movements |
|
|
What does the "lateral hemisphere" control? WHy does it's location next to the intermediate hemisphere make sense then>
|
motor planning
distal limbs need the most amount of motor planning |
|
|
Show the flocculonodular lobe?
|

|
|
|
What region of there cerebellum (vermis etc) is it a part of?
|
It is a little bit of all of them depending on the zone.
|
|
|
Which part of the floccolonodular lobe looked the biggest?
|
The vermis part
|
|
|
So what can you infer about it's function from that?
|
it is important for control of trunk muscles
|
|
|
What are trunk muscles mainly used for?
|
Posture and balance
|
|
|
What is another name for the flocculonodular lopbe?
|
The archicerebellum
|
|
|
What structure does the flocculonodular lobe get it's input from?
|
The vestibular nuclei
|
|
|
So What are it's two functions?
|
1. Help body stand up (ViP) and balance
2. Regulate MLF for eye movement |
|
|
Which region of the cerebellum will send out fibers to the extrapyrimidal tracts the most?
|
The vermis/flocculonodular lobe
|
|
|
What is the only type of neuron to exit the cerebellum?
|
purkinjie cells
|
|
|
What are the most giant cells in the cerebellum?
|
the purkinjie cells
|
|
|
What NT does the purkinjie cells only use? Implications?
|
GABA. All output of the cerebellum is inhibitory
|
|
|
What is the only type of input going into the cerebellum?
|
mossy and climbing fibers which are both excitatory
|
|
|
What do all purkinjie cells end at?
|
deep cerebellar nuclei, which means they carry out all the effective cerebellar output
|
|
|
What will the deep cerebellar nuclei neurons end on?
|
always UMN's (main and supporting)
|
|
|
What is the main function of the mossy fibers?
|
To update the cerbellum about ongoing movements or motor plans
|
|
|
What is the main function of the climbing fibers?
|
They update the cerebellum about errors in movment
|
|
|
What would you not have if you had damage to your inferior olive or the climbing fibers?
|
You would not be able to have motor learning
|
|
|
Name whihc fibers fufill the following functions.
Tell cerebellum about... 1. The motor plan 2. The motor outcome 3. Help with motor leanring |
1. plan- corticopontine
2. outcome- spinocerebellar 3. learning- inferior olive/climbing fibers |
|
|
Which spinocerebellar tracts are responsible for arm vs leg movement?
|
ventral- arm proprioception
dorsal- leg proprioception (the slide on his lecture was ******* wrong, textbook) |
|
|
What is the only real thing you need to know about what comes in and out of the cerbellar peduncles?
|
input comes through mainly the inferior and middle peduncles
output mainly goes through the superior |
|
|
What are the two fissures of the cerebellujm?
|
primary and posterolateral
|
|
|
What is anterior and posterior in the cerebellum? (think embryology)
|
up top is anterior
|
|
|
Show the cerebellum and point out where the two fissures are
|

|
|
|
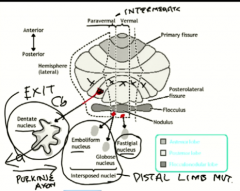
Show which region of the cerebellum each deep nuclei is in. Note their size and shape too.
|
|
|
|
Where do the do the deep cerebellar nuclei mainly send their fibers out? (peduncle) exception?
|
the superior peduncle except the vermis/flocculonodular lobe goes through the inferior
|
|
|
What is the general rule for what must pass through the thalamus?
|
Any fiber, sensory or motor, must pass through the thalamus if they want to REACH THE CORTEX
|
|
|
Judging from their functions, the fibers from which deep nuclei go to the red nucleus vs the corrtex?
|
red nucleus- paravermal- eboloform and globus
cortex- dentate |
|
|
So which part of the thalamus will relay the denate nuclei fibers?
|
the ventral anterior and ventral lateral
|
|
|
Do the cerebellar cortical fibers cross? Where?
|
Yes, in the midbrain
|
|
|
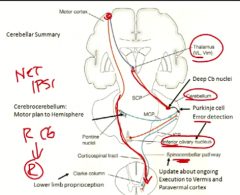
What side of the cortex will the right cerebellum plan and fine tune for? What side of the body is this?
|
the left of the cortex
the right of the body |
|
|
Show how the fibers cross back and forth in a frontal view.. Note which level they cross at.
|
|
|
|
What sx will a person with cerebellar disease have? Will they have weakness?
|
tremor WITH MOVEMENT (intention tremor)
no weakness |
|
|
Which side will a pt tend to fall with a cerbellar lesion?
|
the side ipsilateral to the lesion
|
|
|
What kind of sx will a person will a pt with a vermal lesion have? Why?
|
an ataxic gait becase they cannot use their thigh muscles well
|
|
|
Dissect a-taxic gait.
|
a- not
taxic- ordered disordered gait |
|
|
How will a person with an ataxic gait walk? Why?
|
With their feet very far apart because they are probably scared of falling
|
|
|
What kind of ataxia is this when you have a cerebellar lesion?
|
a MOTOR ataxia
|
|
|
Under what conditions will a person with motor ataxia lose their balance?
|
under all conditions
|
|
|
do you have tremors with cerebellar lesions at rest?
|
no, only with movement
|
|
|
When do these intention tremors increase? Why?
|
As you are nearing the object because that requires the most fine tuning which you don't have.
Since it is motor, looking won't help it much. |
|
|
What other two intention tremor disorders may people with cerebellar lesions have?
|
dysmetria and dysdiachokinesis
|
|
|
What is the classic test for dysmetria?
|
finger to nose
|
|
|
How many times do you need to test finger to nose?
|
Twice, once on each side.
|
|
|
What are the only two NT's used in the cerebellum?
|
GABA and glutamate
|
|
|
WHat two sx would someone with a flocculonodular lobe dysfunction have?
|
scanning speech (scanning dysarthria)
and abnormal conjugate gaze |
|
|
What is scanning speech like?
|
you isolate each syllable you say so it sounds really chopped up.
|
|
|
dissect dys-arthria
|
dys- bad
arthria- articulation |
|
|
What blood thing will damage purkinjie cells in the short vs long term?
|
short- alcohol excess
long- thiamine deficiency |
|
|
What particular part of the cerebellum purkinjie are affected? Mnemonic?
|
the vermal purkinjie cells because they are involved with balance and officers use the straight line test
|
|
|
NOW WE TALK ABOUT THE BASAL GANGLIA
|
WOOT
|
|
|
What is the main job of the basal ganglia?
|
To get movements started
|
|
|
How do the basal ganlia and cerebellum work together?
|
CB helps plan the movement
the BG gets the movement started and the Cb makes sure it is run smoothly |
|
|
What regions of the basal ganglia are subtelecephalic (4), diencephalon (1), and brainstem (1)?
|
subtelencephalic- CN, putamen, GPI, GPE
diencephalic- subthalamus brainstem- SN |
|
|
Is subtelencephalic part of the telencephalon?
|
yes
|
|
|
WHat is the destination of the BG?
|
UMN in the cortex
|
|
|
WHat 4 NT's are used by the BG?
|
GABA, Glutamate,
ACh, dopamine |
|
|
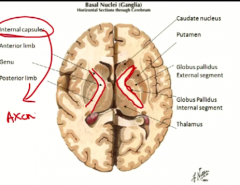
Show a netters diagram of what the internal capsule looks like.
|
|
|
|
What passes through the internal capsule?
|
ALL AXONS THAT LEAVE OR ENTER THE CORTEX
|
|
|
highlight where the straitum is in the last pic.
|

|
|
|
Show a coronal view of what the internal capsule (blue) and striatum (red) look like.
|

|
|
|
What NT's will enhance the direct vs indirect pathways?
|
direct- DOPA
Indirect- ACh |
|
|
WHat is it called to have two inhibitory neurons next to each other?
|
disinhibition (the following neuron is activated)
|
|
|
What things do the direct and indirect pathway have in common?
|
They both start and end with an excitatory neuron
They both contain one set of disinhibitory neurons |
|
|
Which thalamic nuclei does the BG feed fibers through?
|
same as the cerebellum
VA and VL |
|
|
What is the same about the begining couple of neurons in the direct and indirect pathways? What is different later?
|
They are both
exite-inhibit-inhibit-excite The indirect has an extra alternamting inhibit-excite afterwards |
|
|
How does the indirect pathways complement the direct?
|
It inhibits all other muscle movements so you can focus on the tast at hand
|
|
|
WHat is the net effect of dopamine on movement?
|
promotes more movement by aiding the direct and inhibiting the indirect
|
|
|
What is the MAIN effect of ACh?
|
To suppress unwanted movement and help the indirect pathway. (although it has a small aiding effect on the direct as well)
|
|
|
What kind of of tremors will parkinson's people have?
|
tremors at rest (problems in suppressing movement)
hypokinesia |
|
|
Basically sum up the main function of dopamine and ACh in the BG.
|
Dopamine- help direct pathway intitate movements
ACh- help indirect pathway suppress movements |
|
|
Which side of the body will be afected by a lesion of the BG on one side?
|
the opposie side because the BG affects the ipsilateral cortex which innervates the contralateral body.
|
|
|
What pathway is affected in Parkinson's?
|
the direct pathway, which is underactive
|
|
|
WHy do pt's with Parkinsons get resting tremors then?
|
We're not really sure
|
|
|
What is an example of a parkinson's resting tremor? WHat does it look like?
|
A pill rolling tremor which looks like the pt is trying to roll a pill between their fingers
|
|
|
Show a pic of the guy with pill rolling tremors
|

|
|
|
Can parkinson's affect young people?
|
YES! Juvenille onset parkinson's
|
|
|
What can you see often in the dopaminergi neurons that are degenerating?
|
Lewy bodies which are eosinophilic inclusions containing alpha synuclein
|
|
|
What degenerates and where in Huntington's disease? Mnemonic?
|
The GABA neurons contained in the head of the caudate nucleus.
(why the caudate nucleus shrinks) |
|
|
What happens to the activity of the cortex in Huntington's vs Parkinson's?
|
H- overactive
P- underactive |
|
|
dissect the word chorea
|
dance (choreography) like
|
|
|
What is athetosis?
|
writing limb movements
|
|
|
Why don't we just give dopamine for parkinson's pts?
|
because it can't cross to BBB
|
|
|
Does L-DOPA fix all sx?
|
No, the resting tremors are still there and we don't know where they are coming from
|
|
|
WHat other drug could help people with parkinson's? WHy?
|
a muscarinic blocker so block the ACh's promoting of the indirect pathway... allowing more movement
|
|
|
What surgery has been shown to help with tremors?
|
taking out a part of the BG
|
|
|
Is L-DOPA a sustainable treatment option for Parkinson's?
|
No, it wears off over time
|
|
|
Wilson's disease is also known as _____ degeneration.
|
hepatolenticular degeneration
|
|
|
What is pathognomonic for Wilson's disease?
|

a Kayser-Flischner ring (can be VERY SUBTLE)
|
|
|
Will people with WIlson's have sx more like parkinson's or huntington's?
|
Either one depending on which pathway gets degeneration (direct or indirect)
|
|
|
what characteristic tremor will pts with wilson's get?
|
wing beating tremor
|
|
|
Show the boy with the wing beating tremor. Describe it?
|

arms contracted slightly and beating. No movement in legs.
|
|
|
What types of drugs are used to treat Wilson's?
|
a copper chelator or another mineral to block absorption
|
|
|
Which is the copper chelator?
|
pencillamine
|
|
|
which is the mineral to block absorption?
|
zinc acetate
|
|
|
What type of stroke causes a hemiballism? (think logically)
|
It would havew to be an intracranial stroke to reach the subthalamus.
Specifically, a lacunar hemorrhagic stroke. |
|
Whaty disease is this? What side of the body is affected?
|
Parkinson's disease for the left side of the body
|
|
|
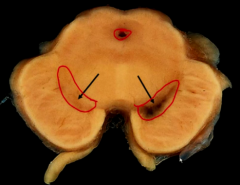
Why is the substantia niagra black?
|
It releases melanin as a byproduct of dopamine synthesis.
|