Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
98 Cards in this Set
- Front
- Back
|
what's grading and staging of liver disease
|
grading: degree of inflammation
staging: degree of fibrosis |
|
|
4 causes of ACUTE liver failure (ALF)
|
DRUGS
alcohol bile obstruction viruses (e.g hepA) |
|
|
jaundice can be classified in 2 ways
|
SITE: pre, intra, post - hepatic
TYPE: conjugated/ unconjugated (by liver) |
|
|
what's the cause of pre-hepatic jaundice
|
excess bilirubin (unconjugated) from too much haem broken down:
- haemolysis - haemolytic anaemias unconj = not water-soluble (not excreted in urine) |
|
|
what causes intra-hepatic jaundice
|
liver cells INJURED/ DEAD + some cholestasis (intra-hepatic bile ducts):
- ALF - hepatitis (alcoholic, autoimmune, viral, drug-induced) - cirrhosis (acute-on chronic/ decompensated) - bile duct loss (PBC, PSC) - preg - storage diseases (Wilson's, haemoachromatosis, a1-antitrypsin def) |
|
|
what causes post-hepatic jaundice
|
bile OBSTRUCTION--> conjugated bilirubin (water-soluble= dark urine, pale stools):
- gallstones in CBD - congenital biliary atresia - CBD strictures - tumours (head of pancreas, cholangiocarcinoma) - PSC, PBC |
|
|
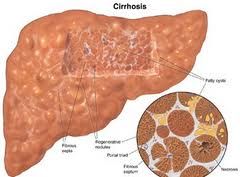
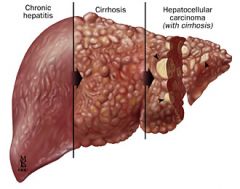
what the pathology behind liver cirrhosis
|
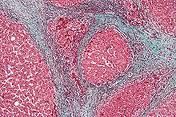
final common END-PT ....IRREVERSIBLE liver damage
fibrosis & nodular regeneration loss function |
|
2 important complications of liver cirrhosis
- what does each complication lead to (effects) |
1) PORTAL HTN: ascites, splenomegaly, varices, caput medusae...
2) liver FAILURE: coagulopathy, encephalopathy (liver flap, confusion), hypoglycaemia, sepsis (also: hepatocellular carcinoma & mallnutrition) |
|
|
what's the progression of alcoholic liver disease with time & which is reversible:
- 2-3d - 4-6wks - months-yrs - yrs |
- 2-3d.................reversible FATTY liver
- 4-6wks............reversible HEPATITIS - mnths-yrs.....irreversibleFIBROSIS - yrs...................irreversible CIRRHOSIS |
|
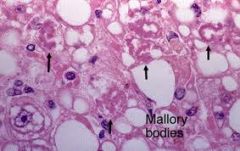
features of ALCOHOLIC hepatitis & NASH/NAFLD (4)
|
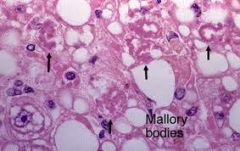
hepatocyte NECROSIS
NEUTROPHILS MALLORY-BODIES pericellular FIBROSIS |
|
|
what's non-alcoholic steatohepatitis (NASH)
- who - may lead to fibrosis & cirrhosis (& liver ca) |
identical pathology to alcoholis liver disease
- non-drinkers - DM, obese, hyperlipidaemia |
|
|
common & rare causes of viral hepatitis
|
hep A,B,C,D,E
delta agent EBV CMV HSV yellow fever virus |
|
|
compare outcomes of hep B and C viral hepatitis
|
B: acute fulimant (death), chronic, cirrhosis, ca, asymp
C: chronic, cirrhosis |
|
|
6 causes of CHRONIC hepatitis
|
viral: hep B & C
PBC PSC autoimmune drug-induced |
|
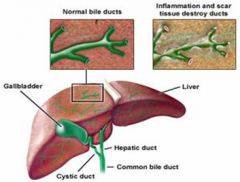
PBC;
- pathology & effects - serology/ test results - age & sex presentation |
rare AUTOIMMUNE chronic non-caseating GRANULOMATOUS inflammation = progressive CHOLESTASIS, CIRRHOSES & portal HTN
- obstructive jaundice, AMA (M2 antimicrobial ab's), IgM - F~50yrs |
|
|
autoimmune hepatitis:
- path - specific features (test results) - age & sex presentation |
Chronic inflammatory.
Auto-ab's: ANA, SMA, LKM, ↑IgG, ↑γGT young/middle-aged F |
|
clinical presentation S&Ss of PBC
specifics in CAPS |
F~50yrs
asymp ↑Alk phos & γGT fatigue PURITIS (itch) XANTHELASMA jaundice/ skin pigmentation portal HTN hepatomegaly |
|
|
clinical presentation S&Ss of autoimmune hepatitis
|
young/ middle-aged F
ACUTE-on-chronic: jaundice, fatigue, abdo pain, nausea CLD: leuconychia, clubbing palmar erythema, spider naevi, DUPUYTREN's contrapture (cirrhosis), hepatomegaly, ascites, portal HTN encephalopathy PBC, PSC, UC, Graves, EXTRAHEPATIC (urticaria) |
|
|
don't forget drug-induced hepatitis:
- which drugs - presentation |
MANY!
mimics any liver disease (acute/ chronic) |
|
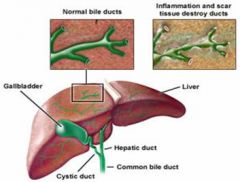
PSC:
- patho - age & sex - stong assoc with which disease - specific features |
CHRONIC inflammation/ fibrosis/ strictures intra- & extra- HEPATIC BILE ducts, F~40yrs
- 80% have UC - post-hepatic jaundice: chronic biliary obstruction - ↑Alk phos, may have ↑AMA & SMA - secondary biliary cirrhosis |
|
|
difference between PBC & PSC
|
PBC: commoner, granulomas, intra-heaptic +ve AMA & IgM
PSC: UC, intra & EXTRA hepatic, biliary obstruction- abnormal LFTs, jaundice, cholangitis |
|
|
3 liver storage diseases
|
Haemochromatosis (iron)
Wilson's (copper) a1-antitrypsin def |
|
|
Haemochromatosis:
- how inherited - how acquired - what are the outcomes if untreated (2) |
1) Autosomal RECESSIVE = ↑iron deposition in liver (& other sites)
2) ↑diet iron/ transfusion/ iron therapy - cirrhosis, hepatocellular carcinoma |
|
|
clinical presentation & features of haemochromatosis (incl age & gender)
|
middle-aged MEN
asyp...then... fatigue arthralgia (iron deposits in joints) slat-grey skin DM ('bronze DM') CLD: hepatomegaly, cirrhosis |
|
|
what's wilson's disease
- key features for Dx - what 2 diseases does it cause |

autosomal RECESSIVE ↑Cu in liver & CNS....treatable.
- Kayser-Fleischer rings (deposits in iris) - lo serum caeruloplasmin - Cu in urine CHRONIC hepatitis & NEUROLOGICAL deterioration |
|
|
what's a1-antitryprin def
- inheritance - what 2 diseases does it cause |
autosomal RECESSIVE
↓synthesis in liver (enzyme inhibitor)....globules trapped in liver CLD (cirrhosis) & EMPHYSEMA |
|
|
2 primary tumours of the liver
|

hepatocellular ADENOMA.......................benign ♀
hepatocellular CARCINOMA (HCC)......malignant- 90% of 1° tumours |
|

secondary tumours (mets) in the liver are much more common than primary ones.
- S&Ss |
fever, malaise, anorexia, loss wt, RUQ pain (liver capsule stretch)
late- jaundice hepatomegaly |
|
|
what diseases is HCC (hepatocellular carcinoma) related with (3)
how does it normally present |
HBV, HCV
cirrhosis mas, pain, obstruction |
|
|
cancer associated with the biliary tree
|
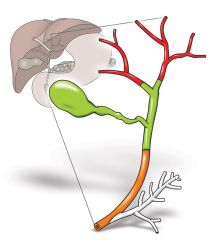
cholangiocarcinoma
|
|
all hepatitis viruses can be ACUTE
which viruses can be CHRONIC? |
[A (only Acute)]
B C D E |
|
|
whats the lab confirmation for hepatitis infection
|
CLOTTED blood for SEROLOGY
(B: surface antigens & ab's also) |
|
|
which hepatitis virus can only co-exist with hepB and exacerbates the infection
|
hepD
|
|
|
hep E:
- similar to which hep virus (clinically and transmission) - where is it common - associated with severe disease when |
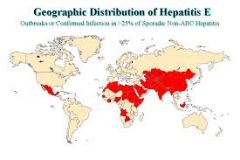
similar to hep A (think vowels!)- young adults, ingestion
common in tropics/ INDIA severe in PREG! |
|
|
how is hep A transmitted?
peak incidence what age? incidence in UK? can only cause ACUTE infection (not chronic) can cause OUTBREAKS! |
INGESTED!
faecal-oral poor hygiene/ overcrowding food & water - travellers - young adults reducing in UK |
|
|
what ab assoc with hep A
control/ prevention? Treatment |

clotted blood for serology- IgM
VACCINE & hygiene monitor for encephalopathy & resolution NO ANTIVIRALS |
|
|
how is hep B & C transmitted (4)
|
BLOOD (IVDUs)
SEX DIRECT VERTICAL transmission (chronic infection more likely) |
|
lab confirmation of Hep B
- how long classifies chronic infection - which component indicates INFECTIVITY - which component in ACUTE / recent infection - which component = IMMUNITY |
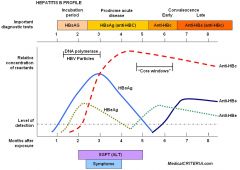
>6months = chronic
HBsAg/HBeAg & DNA = INFECTIVE ant-HBc IgM = current/ recent ACUTE infection Anti-HBs = IMMUNITY |
|
|
which components in the blood indicates chronic hep B carrier
|
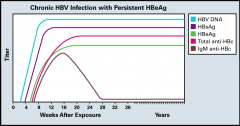
HBsAg >6mnth
Anti-HBc IgG (+/- eAg/anti-eAg, c IgM) |
|
|
what does anti-HBsAg alone indicate
|
vaccination w/o disease
(or transfusion with blood possessing immunity) no anti-HBc IgG |
|
|
what does presence of HBsAg & HBeAg indicate
|

incubating infection
|
|
|
what does ↑↑↑LFTs, HBsAg/HBeAg, Anti-HBc IgM & anti-HBc IgG indicate
|
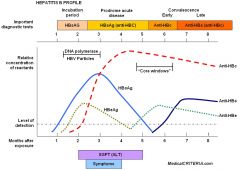
ACUTE infection
|
|
|
what does anti-HBs & anti-HBc IgG indicate
|

recovery from INFECTION
|
|
|
which antibody after HBV infection indicates immunity from NATURAL infection that vaccination doesn't give in addition to anti-HBsAg
|

anti-HBcAg IgG
|
|
|
clinical features of viral hepatitis
|
fever, malaise, anorexia, nausea, arthralgia, jaundice, hepatomegaly, splenomegaly, lymphadenopathy
(extra-hepati common in HBV) |
|
|
clinical features of HBV
|

viral hep: fever, malaise, anorexia, nausea, arthralgia, jaundice, hepatomegaly, splenomegaly, lymphadenopathy
+ EXTRA-hepatic: arthralgia, urticaria (itchy rash- pic) |
|
|
control and treatment of HBV
|
minimise blood exposure & safe sex
VACCINATION prophylaxis (e.g travel) & after ANTIVIRALs: - peginterferon - suppresive antivirals (entecavir, Tenofovir) |
|
|
which viral hepatitis (B,C,D,E) is more commonly chronic
|
~85% HCV chronic
|
|
|
if an individual tests +ve for anti-HBV, what test is done to assess if they have an active/ past infection
|
VIRAL RNA PCR
|
|

which 2 viral hepatitis's can be prevented with VACCINE
|

A (acute) & B (prophylaxis & after)
|
|
|
3 outcomes for hep A
|
asymp & resolution
acute infection ---> resolution acute liver failure (rare) ---> death/ resolution [NB: no chronic infection] |
|
|
outcomes for hep B & C viruses
|
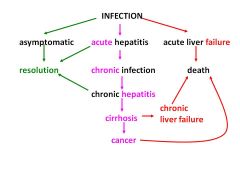
.
|
|
|
in chronic viral hepatitis, how many yrs is taken to cirrhosis and hepatocellular carcinoma
|
>20rs Cirrhosis
>30yrs carcinoma |
|
|
what's significant about vertical transmission of hep B to a baby- what pattern of infection do they show
|
more likely to show CHRONIC infection & complications
|
|
|
when are antivirals used in viral hepatitis
|
CHRONIC infection only (not acute!)
infalmmation before complications adults |
|
|
what test results would confirm you could treat chronic infection with
- HBV - HCV how long is considered chronic infection |
HBV: HBsAg & DNA
HCV RNA present (active) >6 months |
|
|
what's peginterferon-α
what is it used to treat ✔advantages ✕. disadvantages |
immune response to viral infection- given via injection as adjuvant for HBV & HCV:
✔sustained ✔predict who will benefit ✕.side effects! ✕. suppression rather than cure ✕. minority benefit |
|
|
2 drugs used in HBV & HCV
|
peginterferon-a & ribavirin
(HBV- also other antivirals) (HBC- antiviral PROTEASE inhibitors: triple therapy) |
|
|
antivirals for HBV
✔advantages ✕. disadvantages |
eg Entecavir, Tenofvir
✔safer ✕. supression ✕.resistance ✕.life-long Rx |
|
|
adverse effect of ribavirin (1)
|
anaemia
|
|
|
what's triple therapy for HBC
- name 2 antivirals used in triple therapy |
newer antivirals give in combination with PEGINTERFERON & RIBAVIRIN
PROTEASE inhibitors: TELAPREVIR & BOCEPREVIR |
|
|
side effects of protease inhibitors used in HCV triple therapy:
- Telaprivir - Boceprevir |
TELAPRIVIR: puritis, nause, rash, anaemia, rectal pain, diarrhoea
BOCEPREVIR: anaemia, distorted sense & smell |
|
|
define ACUTE liver disease
|
rapid development of liver dysfunction w/o prior liver problems
<6mths ENCEPHALOPATHY |
|
|
difference between LFTs & TRUE LFTs
|
LFTs: ALT/AST, Alk phos, GGT
TRUE: BR, Alb, PTT |
|
|
important Q's to ask when suspecting ACUTE liver failure (ALF) (6)
|
symps
duration DH (OTC, herbal, supplements) TOXINS INFECTIONs ALCOHOL TRAVEL |
|
|
Ix's for acute liver disease (ALD)
|
LFT's (incl alb, BR, PTT)
glucose Virology & micro (bloods, urine) & AUTOab's (e.g IgM, AMA) ferratin, caeruloplasmin, a1-antitrypsin USS rare- biopsy |
|
|
treatment of ALD
|
3mnth REST
FLUIDS, no alcohol ↑CALORIES- metabolic considerations treat ITCH (eg. UDCA) treat hypoglycaemia!!! |
|
|
treatment of PBC & PSC
|
PBC: uresodeoxycholic acid (UDCA)
PSC: corticosteroids & uresodeoxycholic acid (UDCA) |
|

what's Budd-chiari syndrome
- what disease / presentations S&Ss can it cause |
hepatic vein obstruction (eg thrombosis, hypercoaguable, tumour)
acute epigastric pain, N&V, shock, insidious portal HTN, ascites, jaundice & cirrhosis, tender hepatomegaly. ACUTE LIVER DISEASE (ALD) |
|
|
how long do hepatic reactions to drugs take
- 3 commonly used medication that can cause ALD |
6 wks
- NSAIDs, amox, co-amoxiclav (also: euphomisms & imported illegal drugs) |
|
|
define FULMINANT hepatic failre
|
JAUNDICE & ENCEPHALOPATHY in a pt with prev normal liver!!!!!!!!!!!
|
|
|
S&Ss of fulminant liver failure
|
JAUNDICE & ENCEPHALOPATHY
hypoglycaemia coagulopathy circulatory failure]renal fulure]infection |
|
|
treatment for fulminant hepatic failure:
- SUPPORTIVE - DEFINITIVE |
SUPPORTIVE: inotropes & FLUIDS
- renal replacement - manage complications TRANSPLANT (life-long immunosupression) |
|
|
some criteria for liver transplants in acute liver FAILURE
|
<pH
↑PTT (clotting) / INR (bleeding) ↑creatinine (renal failure) jaundice/ encephalopathy ↑lactate ↑bilirubin >40yrs |
|
|
which cells initiate fibrosis (which eventually leads to cirrhosis)? (2types)
|
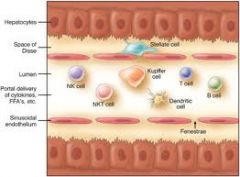
activated quiescent hepatic STELLATE cells (HSC)
by-prods of activated KUPFFER cells |
|
|
what type of liver disease does metabolic syndrome predispose to?
(type 2 DM, obese, low HDL, HTN, hyperlipidaemia) |
NAFL (non-alcoholic fatty liver disease)
|
|
|
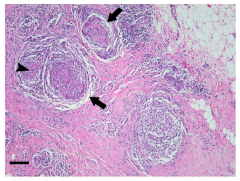
what type of gramulomas are seen in PBC
|
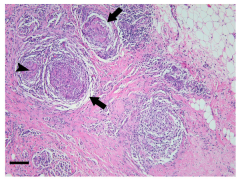
non-caseating
|
|
|
what test results are characteristic for PBC
key |
↑↑↑alk phos (obstructive LTF's)
AMA ab's type M2 (anti-mitochondrial) fatigue, itch (PRURITIS), XANTHELASMA, hepatomegaly |
|
|
treatment of PBC
what symptom is a poor indicator |
uresodeoxycholic acid (helps itch)
jaundice poor indicator |
|
|
distinguish between the 2 types of autoimmune hepatitis
- age - serum ab's |
type 1: ADULT, ANA +/- SMA
type 2: CHILDREN, LKM-1 |
|
|
histopathology of autoimmune hepatitis- BIOPSY to rule out:
- Wilson's disease, a1-antitrypsin def, viral hep, drug-induced, ... |
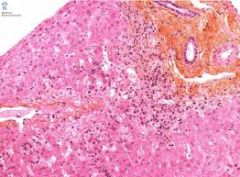
INTERFACE hepatitis
necrosis eosinophils, lymphocytes & inflam cells fibrosis / cirrhosis |
|
|
treatment of autoimmune hepatitis
|
corticosteroids (prednisolone)
azathioprine |
|
|
treatment of haemochromatosis
|

venesection
|
|
|
hwo to Dx & treat Budd-Chiari syndrome (obstruction of hepatic veins)
|
USS
Recanalisation/ TIPS (transjugular intrahepatic portosystemic shunt) |
|
|
which drug used to treat RA & psoriasis shows does-dependent liver toxicity
what does it cause (in the liver) |
METHOTREXATE
fibrosis |
|
|
what causes cardiac cirrhosis
|
secondary to RHF:
- tricuspid valve incompetence - congenital -rheumatic fever - constrictive pericarditis/ cardiac tamponade/ effusion) |
|
|
presentation of cardiac cirrhosis
|
CCF/ RHF
hepatomegaly portal HTN: ascites, varices, caput medusa, liver impairment.... |
|
|
which viral hepatitis is most common worldwide
|
HCV
|
|
|
treatment for compensated liver cirrhosis
|
reduce salt intake
avoid aspirin & NSAIDs good nutrition (support) no alcohol |
|
|
score used to cirrhosis to predict prognosis & variceal bleeding risk
|
CHILD-PUGH
|
|
|
how does portal HTN cause renal failure
|
hepatic vessels release vasodilators = ↓systemic MAP = baroreceptor reflex = renal artery myogenic response 'autoregulation' = renal hypoperfusion = failure = accumulate creatinine & urea = toxicity
|
|
|
Ix's for ascites
|
spontaneous bacterial infection?- tap & neutrophil count
USS |
|
|
treatment for ascites spontaneous bacterial peritonitis (3)
|
ABX's
TERLIPRESSIN for vascular instability maintain renal PERFUSION NUTRITION & NO Na+ |
|
|
which drugs to avoid in ascites
|
NSAIDs & aspirin
|
|
|
treatment for ascites
|
SPIRONOLACTONE (monitor U&Es)
PARACENTESIS- rapid relief TIPS transplant |
|
|
how to quickly relieve ascites
|
paracentesis
x. risk infection x. encephalopathy x. hypovolaemia |
|
|
what causes asterixis (liver flap)
|
ammonia not metabolised by liver--> circulates to CNS, affects signalling
|
|
|
what can asterixis indicate
|
liver disease
salbutamol use (tremor) CO2 retention alcohol-withdrawal anything neurological |