Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
49 Cards in this Set
- Front
- Back
|
What is the exact opposite of anemia?
|
Erythrocytosis
|
|
|
What is the definition of Erythrocytosis? Another quasi-name?
What are the two classifications of causes? |
An increase in the number of circulating RBCs per volume of blood.
Synonym = polycythemia Primary, Secondary |
|
|
What causes Secondary Erythrocytosis?
|
tissue hypoxia --> EPO production by the kidney
|
|
|
Can treatment with EPO and/or androgens cause pirmary or secondary erythrocytosis?
|
secondary
|
|
|
What is hyperviscosity syndrome? This is developed by some patients with...
|
Headaches
Visual changes Tinnitus Dizziness Paresthesias Decreased mental acuity ...erythrocytosis. |
|
|
What does the decision to treat secondary erythrocytosis depend on?
|
prescence of hyperviscosity syndrome. yes = treat, no = don't treat.
|
|
|
Define/Characterize the myeloproliferative disorders. Are they clonal or non clonal?
|
Stem Cell Disorders leading to autonomous production of hematopoietic cells from ALL THREE LINEAGES (red cells, white cells, platelets)?
Clonal. |
|
|
Name the neoplastic disorder arising from a pluripotent stem cell, generally characterized by erythrocytosis, with or without concomitant thrombocytosis and leukocytosis.
Is this an example of primary or secondary erythrocytosis? |
Polycythemia vera.
primary. |
|
|
Primary vs. Secondary Erythrocytosis?
|
Primary: BM is doin' whatever it wants.
Secondary: BM is doing what it's told. |
|
|
In P. vera, many if not all of the circulating blood cells are derived from a ______ neoplastic stem cell? Why is this?
|
single
They can divide w/o EPO. |
|
|
How do we Dx. P. vera these days?
|
We do two tests:
EPO = it will be low. JAK2 mutation |
|
|
Will EPO be low or high in p. vera?
|
low.
|
|
|
JAK2 V617F causes loss of _______ leading to _____ ____ of JAK 2.
Is this seen in normal people? |
auto-inhibition
constitutive activation Never. |
|
|
What the 4 phases of the progression of P vera?
|
Latent phase - asymptomatic
Proliferative phase - pts may be hypermetabolic or have sx of hyperviscosity or thrombosis Spent phase - anemia, leukopenia, secondary myelofibrosis, increasing liver and spleen size Secondary AML 1-2% of pts treated with phlebotomy alone Certain drug therapies increase risk |
|
|
What is the 'spent' phase of P vera?
|
patients have anemia, thrombocytopenia
liver enlarged, splenomegaly. Marrow is filled with scar tisue, liver and spleen start showing hematopoesis. |
|
|
What are 6 Sx more specific to P vera and myeloproliferative diseases?
* note that all of the other erythrocytosis sympt still apply in addition. |
Pruritis after bathing
Erythromelalgia Hypermetabolic symptoms Thrombosis (arterial or venous) Hemorrhage |
|
|
What is Erythromelalgia?
|
platets produced are too active
|
|
|
PEx findings in P vera?
Lab values? |
Facial Plethora
Splenomegaly Hepatomegaly Distention of Retinal veins. elevated platelets, basophilia (can be seen in any MPD) LOW EPO lvls + JAK2 V617F elevated uric acid, elevated B12 elevated leukocyte alkaline phosphatase |
|
|
P vera Tx?
What has shown to decrease risk of thrombosis in PV patients? |
Phlebotomy until they're iron deficient.
Hydroxyurea Low dose aspirin, give it to all patients. |
|
|
What are the downsides of treating P vera w/ phlebotomy?
|
Increased risk of thrombosis
No effect on progression to spent phase May be insufficient to control disease |
|
|
What is the wimpier sibiling of P.vera?
What % is clonal? Those that aren't clonal, explain? |
ET: essential thrombocythemia
50% the rest have polyclonal increase in megakaryocytes |
|
|
How do we make the Dx of essential thrombocythemia (ET)?
|
First, rule out secondary causes of thrombocytosis: cancer, infection, inflammation, bleeding, iron deficiency
Exclude P vera Exclude CML Platelets must be >600 on two separate occasions |
|
|
Does ET progress to AML? What is the major complication of ET?
Can ET progress to myelofibrosis? |
No, rarely.
thrombosis. Yes, it can. |
|
|
Thrombosis in ET is mainly which type?
|
You see both arterial and venous.
|
|
|
Labs in essential thrombocythemia (ET)?
Which percentage have a JAK2 mutation? |
If the plt count is very high, there may be pseudohyperkalemia and pseudohypoglycemia. This goes away if the blood is drawn into a heparinized tube.
50%. |
|
|
What is the Dx if patients have a + JAK 2 and high platelets?
|
ET is the Dx
|
|
|
What are pseudohyperkalemia and pseudohypoglycemia? when is this seen?
|
platetes eat the sugar in the tubes where there is no heparin... can make the potassium & glucose artifically high.
|
|
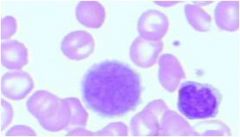
What is this?
|
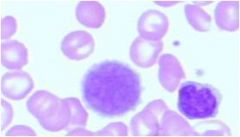
A giant platelet.
|
|
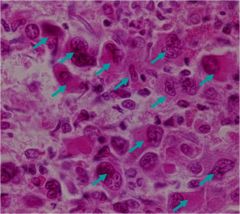
What are these? When are they seen?
|
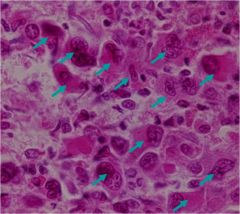
abnormal megakaryocytes, ET.
|
|
|
ET Tx? Who do we Tx?
How do we tx? |
Treatment targeted at reducing the platelet count
those who have had or are at risk for thrombosis, those >65 y.o., or pts with plts > 1-1.5 million Anagrelide Hydroxyurea Interferon alpha |
|
|
In Myelofibrosis (MF), why can't the patients eat even though they're hungry?
|
Spleen is HUuuuuGE, 'n takes up the space.
Hepatomegaly too. |
|
|
MF peripheral smear shows....
|
leukoerythroblastic picture, with teardrops, NRBC and early granulocytes
|
|
|
"Dry tap" is what? associated with what?
What is seen on BM biopsy? |
inability to aspirate liquid marrow
MF Increased collagen and reticuluin |
|
|
What is the Tx of MF?
Is splenectomy a good idea? |
There is no definitive therapy
If patient is young, BM transplant can be done, but older patients have too high mortality well, it's very risky., frequent complications of thrombosis, hemorrhage, and infection. |
|
|
What does 'myelo-' mean?
|
marrow
|
|
|
Define myelodysplastic syndromes.
|
Conditions in which there is disordered maturation in 1 or more cell lines, usually producing cytopenias
Population of dysplastic cells represent an abnormal clone of cells |
|
|
Myelodysplastic syndromes are a ____ of disorders. Are they inherently progressive?
|
spectrum
No. |
|
|
Are myelodysplastic syndromes (MDS) a disease of the old or the young?
|
elderly.
|
|
|
What are the lab findings in MDS?
|
Macrocytosis w/o low B12 or folate
neutrophils can be hypogranular or bi-lobed can have monocytosis (don't know why) |
|
|
How should we think about MDS?
|
zerox, or a zerox, of a zerox.... and eventually (when you're old) you can't tell a c from an a, etc.
In the case of MDS, we have cells, but they're not quite right. |
|
|
What are some features of the marrow in MDS?
|
Megaloblastic erythropoeisis
Ringed sideroblasts Abnormal nucleus of RBC precursors (dyserythropoiesis) Small megakaryocytes with abnormally hypolobate nuclei Blast cells should account for <20% of marrow cells |
|
|
In which disorder should blast cells account for <20%?
>20%? |
MDS.
Acute leukemia. |
|
|
Where are ringed sideroblast seen?
|
in MDS.
|
|
|
___ - - - progression ---- -- -- > Acute Leukemia?
|
MDS
|
|
|
Tx of MDS?
Once the patient develops AML, the chacnes of achieving remission is _____, and their duration of any remission is ______. |
usually supportive: transfustions of RBCs and platelets, Growth Factors
decreased, shorter. |
|
|
If you're gonna get AML, whould you rather get it as a young person de novo, or as an old person as the end of a progression of MDS? Why?
|
young person, because they kid's other stem cells are probably ok. those old people with progressive MDS probably have corrupted their other cells as well.
|
|
|
What is a clonal stem cell disorder that affects primarily megakaryocytes?
|
Myelofibrosis (MF)
|
|
|
The spent phase of all myeloproliferative disorders can be difficult to distinguish from...
|
...primary MF
|
|

What type of cell is shown here? What is it characteristic of and why?
|

Ringed sideroblast. Myelodysplastic Syndrome (MDS).
The body has iron available but cannot incorporate it into hemoglobin. |