![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
170 Cards in this Set
- Front
- Back
|
Diseases caused by pneumococcus? |
Otitis otitis media and bronchitis serious illnesses - pneumonia, meningitis and septicaemia |
|
|
How does invasive pneumococcal disease present in children vs adults? |
Invasive pneumococcal disease in adults usually occurs as pneumonia, vs children who usually get bacteraemia. |
|
|
T/F Invasive pneumococcal disease is a notifiable disease? |
True since 2001 |
|
|
What is the most common communicable disease contributing to premature death in ATSI populations? |
Pneumonia Hospitalisation is 4-8 x more common in ATSI populations |
|
|
Who is funded for pneumococcal vaccination (outside childhood vaccinations)? What are the recommendations? |
ATSI > 50 (2 vaccinations) ATSI 15-49 with high risk condition (3 vaccinations) - Current smoker, ETOH related disease, chronic disease such as CHF, CKD, COPD, diabetes 23cPPV Single vaccination --> revaccination @ 5 yrs --> 2nd revaccination @ further 5 yrs or 50yrs whichever is later |
|
|
Who is recommended to have the influenza vaccination? Funding? Guidelines |
Recommendation - ALL >15 yrs, or >6 months with chronic illness (although the immunisation website says all > 6 months) Funding - Free vaccine - >65 yrs - All > 6 months with chronic disease - Pregnant women - All ATSI > 15 yrs; ATSI 6 month - 5 yrs - Health workers - Annual vaccination prior to winter |
|
|
Effect of influenza on ATSI populations? |
High risk group 4 times more likely to be admitted to hospital Accounted for 13% of deaths |
|
|
Effect of influenza vaccination? |
Protects against disease and its complications in up to 70% of those vaccinated |
|
|
Treatment of influenza? |
Neuraminidase inhibitors - NIs - Oseltamivir (oral) - tamiflu + Zanamivir (inhaled - Both approved for use in AUS for the treatment/prevention** Flu A/B - Needs to be started within the first 24-30hrs, no effect following 2 days. - Effect - shortens symptoms by 1-3 days **Prevention in high risk patients during pandemics |
|
|
Vaccinations for ATSI Children by Age group (in addition to the normal schedule)? |
0-5 - Pneumococcal - additional booster 12-18 months - high risk areas - Hep A - 2 doses 6 months apart over 12 months - high risk areas - Influenza 10-15 - Routine only 15+ - Pneumococcal - if high risk - Influenza |
|
|
Vaccinations for older Australians ? |
Over 65 - Annual Influenza - Pneumococcal - Also advised to have dTpa if not had one in the last 10 yrs but this is not funded ATSI > 50 - Annual Influenza - Pneumococcal 71-79 yr - Varicella catch up program - Zostavax single vaccination until 2021 |
|
|
Vaccination/s due at birth? |
Hep B only - Greatest benefit within 24 hrs, must be within 7 days Infants also get Vit K to prevent ICH |
|
|
Vaccination/s due at 2 months? |
3 VACCINATIONS 1. hepB-DTPa-Hib-IPV - Hep b - dTpa - diptheria, tetnus, acellular pertussis (whooping cough) - Hib - type b - Haemophilus influenzae - Inactivated polio 2. Pneumococcal conjugate - 13vPCV 3. Rotavirus - oral |
|
|
Vaccination/s due at 4 months ? |
3 VACCINATIONS 1. hepB-DTPa-Hib-IPV - Hep b - dTpa - diptheria, tetnus, acellular pertussis (whooping cough) - Hib - type b - Haemophilus influenzae - Inactivated polio 2. Pneumococcal conjugate - 13vPCV 3. Rotavirus - oral |
|
|
Vaccination/s due at 6 months? |
3 VACCINATIONS 1. hepB-DTPa-Hib-IPV - Hep b - dTpa - diptheria, tetnus, acellular pertussis (whooping cough) - Hib - type b - Haemophilus influenzae - Inactivated polio 2. Pneumococcal conjugate - 13vPCV 3. Rotavirus - oral |
|
|
Vaccination/s due at 12 months? |
2 VACCINATIONS 1. Hib - MenC - Haemophilus Influenzae B + Meningococcal B 2. MMR - Measles, mumps rubella |
|
|
Vaccination/s due at 18 months? |
2 VACCINATIONS 1. DTPa - Diptheria, tetnus, acellular pertussis 2. MMRV - Measles, mumps, rubella, varicella |
|
|
Vaccination/s due at 4 years? |
1 VACCINATION + Catch up if required 1. DTPa-IPV - Diptheria, tetnus, acellular pertussis, inactivated poliomyelitis Catch up - MMRV - if not given at 18 months (MMR + varicella combo) |
|
|
Vaccinations covered by school programs? |
10-15 yrs of age Varicella HPV - all adolescents 12-13 yrs DTPa |
|
|
Who receives additional pneumococcal vaccinations as children? |
Medically at risk children at 12 month + 4 years - 13vPCV booster ATSI - 12-18 months (13vPCV) in high risk areas - >15 yrs (23vPPV) - medically at risk |
|
|
Define CKD. |
Kidney damage = pathological abnormality - blood tests, urine tests, imaging or GFR < 60 Persisting for > 3 months |
|
|
What are the stages of CKD? |
6 Stages 1 - Kidney damage with normal or increased GFR > 89 2 - Kidney damage with mildly reduced GFR 60-89 3 - Moderately reduced eGFR - 3A - 45-59 - 3B - 30-44 4 - Severely reduced GFR 15-29 5 - Kidney failure - < 15 or dialysis |
|
|
What is the rate of CKD in ATSI vs non-ATSI? |
10x increased CKD |
|
|
Which of the following are T/F? 1. Reduced GFR and raise albumin excretion are independent risk factors for mortality. 2. Mortality from CKD is from the cardiovascular risks. 3. People with CKD are more likely to die from IHD or CVA than develop end stage CKD. 4. Low levels of microalbuminuria are not associated with increased stroke morbidity. |
1.True 2. True 3. True 4. False - increased cardiovascular and stroke risk |
|
|
Which of the following are true/false? 1. eGFR calculations are validated for ATSI populations. 2. eGFR varies with illness, diet, extremes of weight 3. Patients should be tested for proteinuria instead of albuminuria as this is more sensitive 4. Albumin is the main protein excreted in all forms of renal failure |
1. False 2. True 3. False - albuminuria is more sensitive and the recommended screening test 4. False - this is not true in causes of tubulointerstitial disease or myeloma |
|
|
Define Microalbuminuria + Macroalbuminuria |
Microalbuminuria - 30-300mg/24hr Macroalbuminuria - >300mg /24hr |
|
|
A urinary dipstick rules out microalbuminuria T/f? |
False - rules out macroalbuminuria only and positive tests should be confirmed with laboratory methods |
|
|
What is a convenient method for assessing urinary protein? |
First morning urine - stop sample ACR - albumin creatinine ratio Or PCR - protein creatinine ratio |
|
|
What are normal ACR levels? |
Males <2.5mg/mmol Females <3.5 mg/mmol Above these levels --> micro/macroalbuminuria |
|
|
What factors may increase albumin excretion in the urine and hence make ACR/24 urinary albumin inaccurate? |
Urinary tract infections Acute febrile illness High dietary protein Heart failure Recent heavy exercise Some drugs Menstruation or vaginal discharge |
|
|
Define an abnormal ACR measurement. |
At least 2 elevated levels in a 3 month period >2.5 Males; >3.5 Females Ie a single test should be repeated |
|
|
When is primary screening for CKD recommended? Which tests? |
1. 18-29 years - without RFs -->Screen for CKD RFs - Obesity, DM, HTN, Smoking, F.Hx @ annual health assessment 2. 18-29 years w/ risk factors --> eGFR + Urine ACR (if high - repeat 1-2x over the next 3 months) 3. All > 30 years --> eGFR + ACR Frequency --> 2. + 3. --> 2nd yearly screening (more frequently if high CVD risk) |
|
|
What are primary prevention strategies to reduced CKD? |
Weight loss/healthy weight/healthy diet Regular exercise Diabetes screening and management HTN screening and management Smoking cessation Limit salt intake Maternal health promotion strategies Prevention of streptococcal infections in childhood |
|
|
Secondary prevention strategies for CKD? |
Patients with ACTIVE CKD 1. Quit smoking 2. Reduced excess weight 3. Regular exercise 4. Restrict Na intake 100mmol/day (6g salt) THERAPY - ACEI/ARB - for BP management and protein excretion - Statin - reduce CVD endpoints |
|
|
What are the goals of secondary prevention of CKD? |
Slow progression of disease Reduced CVD endpoints |
|
|
T/F Combination of an ACEI + ARB may enhance BP lowering effects but may worsen kidney outcomes. |
True |
|
|
When to refer patients with CKD? |
Referral to a NEPHROLOGIST - Stage 4/5 - Persisting albuminuria ACR>30 - Declining eGFR > 5 in 6 months (average of at least 3 measurements) - CKD + Elevated BP that is not at target despite at least 3 agents - Unexplained anaemia <100 + eGFR<60 |
|
|
Advise patients taking ACEI/ARB + diuretic to avoid which meds? |
NSAIDS - except low dose aspirin |
|
|
When should an ACEI or ARB be started in patients with CKD? |
CKD + Albuminuria - regardless of BP CKD + DM - " " target <140/90 but lower <130/80 if albuminuria present A statin should also be considered |
|
|
Diagnosis of osteoporosis? |
DEXA (dual energy x ray aborptiometry) - bone mineral density testing. T score - compare to 30 yo T <-2.5 = osteoporosis T -1.5 to -2.5 = osteopaenia |
|
|
Prevalence of osteoporosis in over 60's ? |
Very common Females 27% Males 11% |
|
|
Life time risk for females and males for a minimal trauma fracture > 60 yrs? |
Females 56% Males 26% |
|
|
Risk factors for Osteoporotic fractures ? |
Female double the lifetime risk of males Previous fracture Worse DEXA score Falls history doubles risk |
|
|
Risk factors for developing glaucoma? |
INCREASED RISK - Family history - first degree relatives - Caucasian and asian patients >50 yrs - African patients >40 yrs HIGH RISK >50yrs + - Diabetes - Myopia - Long term steroid use - Migraine and peripheral vasospasm - Abnormal BP - History of eye trauma |
|
|
Steps to take for prevention of glaucoma in increased risk and high risk patients? |
Refer for opthalmoscopy (exam of optic nerve head), measurement of IOP (tonometry), assessment of visual fields (perimetry - automated) - Either by opthalmologist or optometrist Refer 5-10 yrs prior to age of relative's onset |
|
|
What is the RACGP standpoint for prostate cancer screening? |
1. No PR exam - DRE insufficiently sensitive 2. No Screening 3. No PSA testing - due to over treatment and complications of treatment and does not save lives. Happy for patient to have PSA testing if the patient is happy with the risks. Have a guideline about how to talk to patients about this. http://www.racgp.org.au/download/Documents/Guidelines/prostate-cancer-screening-infosheetpdf.pdf |
|
|
Risk factors for prostate cancer? |
Men with 1 or more 1st degree relatives with prostate Ca Men with first degree relative with familial breast cancer - BRCA1 or BRCA2 |
|
|
Complications of a prostatectomy? |
Erectile dysfunction Urinary incontinence Urinary irritation Bowel symptoms |
|
|
Risks following diagnosis with prostate cancer? |
Enormous spike in cardiovascular disease and suicide (11x and 8x increase respectively) in the week following diagnosis. |
|
|
Which of the following are true/false? 1. Prostate screening saves lives. 2. Sepsis requiring ICU occurs in 1% of patients following prostate biopsy. 3. Urinary incontinence following prostatectomy returns to normal in 75-90% of patients. |
1. False - meta-analysis results 2. True - Australian data (NPS) 3. True - after 2 years |
|
|
Which of the following are true/false? 1. Biennial faecal occult blood test can reduce colorectal cancer mortality by 16%. 2. FOBT is based on guaiac based testing. 3. Age of FOBT testing is from 50 yrs to 75 yrs in asymptomatic individuals. 4. CT colonography is routinely used for colorectal Ca screening now |
1. True 2. False - Now done by a more specific immunochemical test 3. True 4. False - insufficient evidence |
|
|
Complications following colonoscopy? |
1. Death - rare 1/10,000-14,000 2. Bowel prep - dehydration, electrolyte disturbance 3. Sedation - cardiac events 4. Procedure - infection, colonic perforation, bleeding |
|
|
What is the standard screening for an average risk patient for colorectal cancer? WHO, TEST, FREQUENCY? |
WHO - Asymptomatic people or one 1st or 2nd degree relative with CRC >55 yrs old TEST - FOBT FREQUENCY - every 2 years 50 yrs-74 yrs |
|
|
What is the standard screening for a MODERATELY INCREASED risk patient for colorectal cancer? WHO, TEST, FREQUENCY? |
WHO - Asymptomatic with - one 1st degree relative with Dx <55yrs or - two 2nd or one 1st and one 2nd degree relatives on the same side of the family with diagnosis at any age. TEST - Colonoscopy first line; if contraindicated --> sigmoidostomy + double contrast barium enema or CT colonography. ** FREQUENCY - every 5 yrs from 50 or 10 yrs younger than the age of first diagnosis ** Consider FOBT in intervening years |
|
|
What is the standard screening for a HIGH risk patient for colorectal cancer? WHO, TEST, FREQUENCY? |
WHO - Asymptomatic with - 3 or more 1st or 2nd degree relatives on the same side - suspected Lynch syndrome/NHPCC or - 2 or more 1st or 2nd degree relatives on the same side with high risk features - multiple CRC in one person, CRC <50yrs, Family member with Lynch syndrome - 1 with a large number of adenomas throughout the large bowel - suspected FAP - familial adenomatous polyposis - Family member with APC (adenomatous polyposis coli) mutation TEST - Referral to bowel cancer specialist for appropriate surveillance + affected members for genetic screening FAP - sigmoidoscopy; HNPCC - colonoscopy Consider FOBT FREQUENCY - As per specialist FAP - yrly from 12-15 until 30-35 then 3 yrly HNPCC / Lynch - 1-2yrly from 25yrs or 5yrs prior to first Dx |
|
|
Aspirin 100mg/day is effective prophylaxis for Lynch syndrome / HNPCC cancer formation. True/false? |
TRUE Reduces cancer for 50% More effective with higher doses ~600mg |
|
|
What is FAP and what is it caused by? What % of CRC is due to FAP? |
Autosomal dominant caused by a germline mutation in APC gene. Manifestation - Colorectal cancer - 100% of untreated subjects by 50yrs Only accounts for 1% of CRC |
|
|
Inheritance of HNPCC is ? Lifetime risk of Ca? |
Autosomal dominant Same as Familial adenomatous polyposis (CRC only) Lifetime risk of CANCER (CRC and other cancers) - 70-90% |
|
|
Frequency of screening in patients with FAP - familial adenomatous polyposis ? |
Every 12 months from 12-15 yrs until 30-35yrs then every 3 yrs after 35 |
|
|
Frequency of screening in patients with Lynch syndrome? |
one to two yearly from 25 years of age or five years earlier than the youngest affected member of the family (whichever is earliest) |
|
|
Appropriate management of + FOBT? |
Referral for colonoscopy These patients are 12x more likely to have CRC than those with a negative FOBT |
|
|
When should a patient have a repeat colonoscopy following polypectomy? |
Depends on the type and number of polyps SEE the below guideline http://www.racgp.org.au/your-practice/guidelines/redbook/9-early-detection-of-cancers/92-colorectal-cancer/ |
|
|
When should a patient have a repeat colonoscopy following polypectomy for a large sessile adenoma removed piecemeal? |
3-6 months and again at 12 months to ensure complete removal |
|
|
Screening for patients >75 yrs old with previous negative FOBT or colonoscopies? |
No further screening Due to lead time 10-20yrs for progression to cancer |
|
|
When should a patient have a repeat colonoscopy following polypectomy for multiple adensomas >5 or >10? |
>5 - 12 months >10 - Sooner than 12 months due to risk of missed polyps |
|
|
When should a patient have a repeat colonoscopy following polypectomy for 1-2 small tubular adenomas? |
5 yrs If next normal then repeat 10 yrs with 2nd yrly FOBT |
|
|
When should a patient have a repeat colonoscopy following polypectomy for >3 high risk adenomas?? |
High risk = >10mm, tubulovillous or villous histology, or high grade dysplasia 3 yrly colonoscopy |
|
|
Age for breast cancer screening? |
50-75 |
|
|
Risk factors for breast cancer? |
Age Hx atypical hyperplasia, lobular carcinoma insitu Strong family history Previous radiotherapy Hormonal - age of menarche age at first birth, obesity, osteoporosis |
|
|
Factors associated with reduced risk of breast cancer in observational studies? |
Physical activity Adequate folate Mediterranean diet Normal BMI (post menopausal women) Decreased EtOH consumption |
|
|
Tool to assess a womens risk of breast cancer? |
International breast cancer intervention study tool (IBIS) https://www.cancer.gov/bcrisktool/ |
|
|
Recommended screening for breast cancer in asymptomatic low risk women? |
Mammograms 2nd yearly aged 50-74 |
|
|
Which of the following are true/false? 1. Breast cancer screening is effective at reducing mortality associated with breast cancer. 2. Breast cancer screening if generally safe without major negatives. 3. Screening in women < 50yrs is not recommended due to the worse benefits/risk profile. |
1. True - Saves 1 in 2000 screened. 2. False - 30% over diagnosis of breast cancer and hence subsequent treatment for people. 10 in 2000 with have unnecessary treatment. 3. True - less lives saved and more false positives |
|
|
Which patients may benefit from earlier screening - ie 40-49 yrs for breast cancer? |
Those with a family relative with breast cancer Cancer Australia recommends annual mammograms from 40 yr if + 1st degree relative with breast cancer 50yrs. |
|
|
What is the rational for ceasing mammograms at 75? |
Insufficient evidence to support benefits/harms as this age group were not included in the studies. Observational studies do support extended screening for older women who have a life expectancy >10 years. |
|
|
What is the evidence for self-examination in screening for breast cancer? |
Insufficient evidence to recommend this screening. Although it is recommended women are familiar with their breasts and monitor for any lumps, discharge, skin changes or pain and notify their GP if any changes occur. |
|
|
What percentage of the population are average, moderate or high risk for breast cancer? |
Average - 95% Moderate - 4% High Risk - 1% |
|
|
What are the factors that make a woman HIGH risk for developing breast cancer? Approach to screening? |
High Risk --> 1in2 to 1in4 chance of developing Ca - High risk for ovarian cancer - Two 1st/2nd ' relatives on one side w/ breast or ovarian cancer PLUS additional relatives with B/O Ca, B Ca <40 yrs, Bilateral B Ca, B+O Ca in the same woman, Ashkenazi jews, B Ca in male. - One 1st/2nd B Ca <45yrs + another with a sarcoma (bone/soft tissue) <45yrs - Family member with + high risk breast cancer gene mutation SCREENING - Referral to cancer specialist, ?genetic testing, +/- prophylactic chemoprevention or mastectomy/salpingoopherectomy |
|
|
Breast cancer prevention options in high risk patients? (<1% of the population) What is their risk of developing breast cancer? |
Risk 1in2 --> 1in4 --- VERY HIGH Prevention - Chemoprevention - SERMS (seletive oestrogen receptor modulators) - Tamoxifen or Raloxifene or Aromatase inhibitors - exemestane and anatrozole. - Surgery - Mastectomy or salpingoopherectomy Screening will be personalised and may include clinical breast exams, imaging - mammography, MRI or USS |
|
|
Which of the following are true/false regarding breast cancer? 1. Salpingo-oophorectomy reduces the risk of breast cancer. 2. Screening test of choice for moderate risk patients is mammography. 3. Breast cancer screening in high risk groups is standardised, routine yearly Mammograms and USS. |
1. True 2. True 3. False - individualised screening plan with breast checks and imaging mammogram, USS and MRI |
|
|
Factors that make a woman moderate risk for breast cancer? Screening? |
Moderate risk - One 1st ' relo with B Ca <50 without other factors - Two 1st ' relos on same side with Breast Ca - Two 2nd ' relos on same side with breast Ca, at least one <50 Screening - Mammogram 2nd yrly 50-74; Annual from 40 if 1st ' relative < 50 with breast Ca |
|
|
Features consistent with average or only slightly high risk of developing breast cancer ? |
Average Risk or slightly higher - One 1st ' relative >50yrs (if younger moderate risk) - One 2nd ' relative at any age - Two 2nd ' relative on same side > 50 yrs (<50 = moderate risk) - Two 1st/2nd ' relatives >50 yrs on different sides of the family SCREENING - 2nd yearly mammograms 50-74 yrs |
|
|
Risk factors for melanoma? |
Age + sex Prior melanom or NMSC Number of naevi F. Hx of melanoma Skin and hair pigmentation Response to sun exposure Evidence of actinic skin damage |
|
|
How frequent should high risk individuals self screen and have a clinical examination to assess for skin cancer? |
Self exam 3 monthly Clinical exam 6 monthly |
|
|
Factors that make a patient high risk for developing melanoma? What to do with these patients? |
1. Previous Melanoma - RR >10 2. >5 Atypical (dysplastic naevi) RR = 6 Management - Preventative advise (all patients) - Examination of skin (Moderate + high risk) - Advise on self examination Self exam 3 monthly; Clinical exam 6-12 monthly |
|
|
Factors that make a patient moderate risk for developing melanoma vs high or average risk? What should be done for these patients? |
Moderate Risk - Family history of melanoma - 1st degree RR=1.7 - Fair complexion, tendency to burn rather than tan, presence of freckles, high naevus count >100, light eye colour, red hair - Presence of actinic damage RR=2 - History of NMSC - High exposure to UV as a child and episodes of childhood burn RR=2 PREVENTION - Prevention advise - Skin exam - opportunistic |
|
|
Which of the following are true/false regarding skin cancer? 1. Patients with moderate risk of melanoma should have 1-2 yrly skin checks. 2. A patient with blonde hair and blue eyes has a moderate risk of melanoma. 3. The presence of dysplastic naevi is a risk factor for melanoma |
1. False - opportunistic screening for exams and advise 2. True - light hair and eye colour is a RF 3. True - high risk if >5 |
|
|
ABCD if melanoma refers to? Other features of suspicious lesions? |
Asymmetry Border irregularity Variable colour Diameter > 6mm Other - Ugly duckling - a naevi that stands out - Nodular melanoma - elevated, firm and fast growing - 7 point checklist (validated) --> 2 pts - change in size, irregular shape, irregular colour, 1 pt - largest diameter >7mm, inflammation, oozing, change in sensation --> score >3 = increased risk of melanoma |
|
|
Management of lesions where there is clear suspicion of melanoma? |
Excision biopsy or referral |
|
|
At what level of UV is skin protection recommended? |
greater than or equal to 3 |
|
|
T/F Daily application of sunscreen reduces the incidence of melanoma and SCC in adults with a prior history of skin cancer. |
True. - study in QLD - RCT |
|
|
Screening recommendations for NMSC? |
Preventative advice for all patients Education regarding presenting to the GP if changes to a skin lesion occur Advise on self examination All opportunistic except for examination of the skin 12 monthly in high risk patients |
|
|
NMSC "high risk" category risk factors? |
HIGH Risk - Previous NMSC - 60% will grow another in 3 yrs - Immunosuppressed - Past exposure to arsenic |
|
|
What are the preventative intervention for cervical cancer? |
1. HPV Vaccination - all 12-13 yr olds - 16/18 (cancer), 6/11 (genital warts), 3 doses -0/2/6 months 2. PAP smear |
|
|
HPV vaccine prevents what % of cervical cancer, % of male related HPV cancers , and % genital warts? |
PREVENTS Subtype 16/18 --> which cause 70% of cervical cancer Subtype 16/18 --> which cause 90% of all HPV related cancers in men Subtype 6/11 --> which cause 90% of genital warts |
|
|
How many doses of HPV vaccine? At what age? At what intervals? |
3 doses 0, 2, 6 months 12-13 yrs - At school at 7 |
|
|
What are the new changes to the cervical screening program in May 2017? |
Asymptomatic women 25-74 --> HPV test every 5 yrs Symptomatic --> Clinical exam which may include cervical cytology + HPV test Women > 70-74 who have had regular screening may have an EXIT HPV test, and exit the screening program |
|
|
What is the current recommendations for cervical cancer screening (until May 2017) ? |
Pap smear 2 yearly for women 18-20 who have had sex or up to 2 years following fist intercourse (which ever is later) Until 70 yrs (with 2 normal Pap tests in the last 5 yrs). Women who are > 70 who have never had a pap test, who request screening should be screened. |
|
|
Which of the following are True/False? 1. Lesbians are not at risk for cervical cancer. 2. Risk factors for cervical cancer include persistent infection with high risk HPV, immunosuppression, smoking, prolonged COCP use. 3. In a pap smear the brush collects ectocervical cells and the spatula collects endocervical cells. |
1. False 2. True 3. False, other way around |
|
|
Does the RACGP recommend pelvic examinations in asymptomatic, non-pregnant women? |
No - There is no evidence of benefit |
|
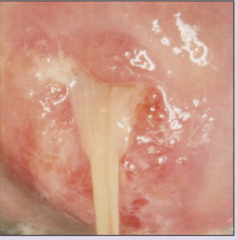
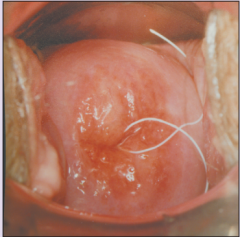
What does this appearance on pap smear indicate? |
Mucoplurulent discharge |
|

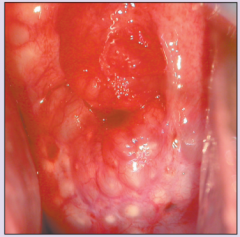
What does this appearance on pap smear indicate? |
Cancer |
|
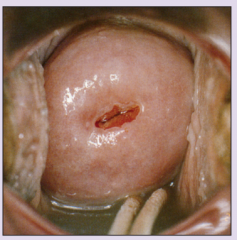
What does this appearance on pap smear indicate? |
Normal cervix in a nulliparous woman |
|

What does this appearance on pap smear indicate? |
Ectropion |
|

What does this appearance on pap smear indicate? |
Normal mulitparous cervix |
|
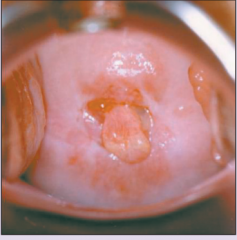
What does this appearance on pap smear indicate? |
Cervical polyp |
|
What does this appearance on pap smear indicate? |
Nabothian Follicles |
|
What does this appearance on pap smear indicate? |
IUD |
|

What does this appearance on pap smear indicate? |
Cervical wart |
|
|
What is the current recommendation for ovarian cancer screening? |
No screening - due to limited evidence to support CA125 / Transvaginal USS surveillance but in patients with BRCA1/2 or multiple 1st degree relatives with ovarian cancer --> consider increased frequency of screening for Breast cancer and Colorectal cancer |
|
|
The current recommendation for ovarian screening is no screening. When may this change? |
With reporting of the most recent european trial which started in 2005. |
|
|
What is the current recommendation for screening for testicular cancer? |
No preventative screening due to insufficient evidence to routinely screen for testicular cancer using clinical or self examination. |
|
|
Risk factors for testicular cancer? |
History of Cryptorchidism RR = 3.5-17 Orchidopexy Testicular atrophy Previous testicular cancer RR =25-28 If high risk - testicular examination - opportunistic |
|
|
Who is recommended to have a BCG vaccination? Age? |
NOT FUNDED - ATSI in northern Australia - Infants born to migrants from high risk countries for TB Given soon after birth to infants |
|
|
Who is recommended to have the meningococcal B vaccine? |
NOT FUNDED <2 yrs and between 15-18yrs (highest incidence age groups) |
|
|
Which vaccinations are recommended to certain groups by the RACGP but are not funded? |
BCG - infants Meningococcal B - <2; 15-18yr olds dTPA - parents and carers of infants < 6months old; Travellers of any age VZV - > 60 yrs to prevent shingles All health workers - dTpa, Hep B, Influenza, MMR, Varicella MSM + IVDU - Hep A+B covered by some state programs |
|
|
VZV vaccination is recommended for which patients? |
18 months - part of MMRV Second shot from 18 months - gives better protection (NOT FUNDED) >60yr - single shot - shingles prevention (NOT FUNDED) |
|
|
Questions to ask as part of a sexual history? |
Sexual activity Gender Number of partners Contraception (inc condom use) Travel history Immunisation status Also ask about HIV/HepC/HepB risk --> IDVU, tattoos and piercings |
|
|
Who's responsibility is contact tracing for STI's or HIV? |
The diagnosing clinician. This may be done via the patient notifying contacts or via online partner notification tools. Ie - www.letthemknow.org.au |
|
|
Which of the following are true/false? 1. 80% of chlamydia infections occur in people <29 yr 2. Screening for chlamydia is recommended in all sexually active people under 29 yrs 3. The overall absolute risk for chlamydia is 20% and for gonorrhoea is 5% for sexually active people under 29% |
1. True 2. True 3. False - Chlamydia 5% absolute risk; Gonorrhoea 0.5% absolute risk |
|
|
Which is the most common STI? |
Chlamydia (both the general population and ATSI) ATSI have 4 x the rate of infection |
|
|
Rank the following STIs in order of prevalence. Chlamydia, HIV, Syphilis, Hep b, Gonorrhoea |
1. Chlamydia -- 371//100 000 (ATSI 1341) 2. Gonorrhoea -- 49/100 000 (ATSI 858) 3. Hepatitis B -- 23/100 000 (ATSI 50) 4. Syphilis -- 8/100 000 (ATSI 32) 5. HIV -- 4/100 000 (ATSI 6) |
|
|
What is the risk of infertility with untreated chlamydia? |
2-8% |
|
|
Screening for MSM for STIs? |
Screen for gonorrhoea, chlamydia, syphilis, HIV Every 12 months |
|
|
ATSI screening for STIs? |
Screening Swabs - PCR gonorrhoea, chlamydia Serology - Syphilis, HIV, Hep A/B if not vaccinated 12 monthly / Opportunistic Offer vaccination for Hep A + B |
|
|
STI screen in pregnant women? |
HIV, syphilis, HepB + HepC If < 29 - also chlamydia and gonorrhoea if high risk |
|
|
Who to screen for HepC? |
IVDU HIV+ |
|
|
How to manage contact tracing with regards to treatment and testing? |
Test for all and treat contacts presumptively |
|
|
Which people have the highest risk for STIs? Investigations? |
MSM - 12 monthly; 3-6 monthly with higher risk. Highest risk features - Unprotected anal sex - > 10 partners in the past 6 months - Participate in group sex or use recreational drugs during sex Investigations - Chlamydia PCR - urine/throat/rectal - Gonorrhoea PCR - Throat/rectal - Serology - HIV, syphilis; if not vaccinated - Hep A+B - Offer Hep A+B vaccinations |
|
|
STI screening for patients who are IVDUs or sex workers? |
Swabs - Chlamydia, gonorrhoea Serology - HIV, Syphilis, Hep A/B Hep C if IVDU 12 monthly |
|
|
Test to be done if clinical suspicion for gonorrhoea ? |
MCS of bodily fluid/swab Otherwise PCR |
|
|
Screening as per RED BOOK - frequency, how, age?
Smoking ? |
Opportunistically
Ask about habits - Ask, assess, advise, assist, arrange |
|
|
Screening as per RED BOOK - frequency, how, age?
Smoking ? |
Opportunistically
Ask about habits - Ask, assess, advise, assist, arrange |
|
|
Screening as per RED BOOK - frequency, how, age?
Nutrition |
2 Years - 6 monthly for as risk populations - over weight, high CVD risk, ATSI
Ask about fruit, vegetable portions, size, salts, saturated fats
All ages |
|
|
Screening as per RED BOOK - frequency, how, age?
Alcohol? |
Every 2-4 yrs (more frequent if risk factors)
Ask about quantity and frequency - advise <2 daily, and no more than 4 in one occasion
All people > 15 yrs |
|
|
Screening as per RED BOOK - frequency, how, age?
Weight ? |
Every 2 years -- annual for DM, CVD, stroke, gout, liver, gallbladder disease, ATSI
Assess BMI, waist circumference (>18 yrs)
All ages |
|
|
Screening as per RED BOOK - frequency, how, age?
Physical activity ? |
2 yearly
Ask about frequency of moderate physical activity - Advise 30 minutes moderate most days (at least >2.5 hrs /week)
All ages |
|
|
Screening as per RED BOOK - frequency, how, age?
Depression? |
Opportunistically
Ask - feelings of hopelessness, depression, loss of interest in activities - always ask about suicide risk if you suspect depression
> 12 years |
|
|
Screening as per RED BOOK - frequency, how, age?
Weight ? |
Every 2 years -- annual for DM, CVD, stroke, gout, liver, gallbladder disease, ATSI
Assess BMI, waist circumference (>18 yrs)
All ages |
|
|
Screening as per RED BOOK - frequency, how, age?
Physical activity ? |
2 yearly
Ask about frequency of moderate physical activity - Advise 30 minutes moderate most days (at least >2.5 hrs /week)
All ages |
|
|
Screening as per RED BOOK - frequency, how, age?
Depression? |
Opportunistically
Ask - feelings of hopelessness, depression, loss of interest in activities - always ask about suicide risk if you suspect depression
> 12 years |
|
|
Screening as per RED BOOK - frequency, how, age?
Chlamydia |
Opportunistic- 12 monthly
Urine/swab PCR
Advise - process, results, treatment, contact tracing
15-29 yrs |
|
|
Screening as per RED BOOK - frequency, how, age?
Skin cancer exam |
Opportunistic - 3/12 for high risk
Skin exam +/- dermoscopy
> 30 yrs (earlier if high risk)
Advise - sun protection |
|
|
Screening as per RED BOOK - frequency, how, age?
Skin cancer exam |
Opportunistic - 3/12 for high risk
Skin exam +/- dermoscopy
> 30 yrs (earlier if high risk)
Advise - sun protection |
|
|
Screening as per RED BOOK - frequency, how, age?
Colorectal cancer |
2 yrs
FOBT
ALL - 50-75 yrs - earlier if high risk (10yrs prior to 1st degree relative if <55yrs) |
|
|
Screening as per RED BOOK - frequency, how, age?
Skin cancer exam |
Opportunistic - 3/12 for high risk
Skin exam +/- dermoscopy
> 30 yrs (earlier if high risk)
Advise - sun protection |
|
|
Screening as per RED BOOK - frequency, how, age?
Colorectal cancer |
2 yrs
FOBT
ALL - 50-75 yrs - earlier if high risk (10yrs prior to 1st degree relative if <55yrs) |
|
|
Screening as per RED BOOK - frequency, how, age?
Absolute CVD risk? |
2 yrly
Online calculator more often if treatment changed
> 45 yrs (>35 ATSI) |
|
|
Screening as per RED BOOK - frequency, how, age?
BP |
Every 2 yrs (12 month if moderate risk, 6/12 if high risk)
Measure
> 18 yrs old
Advise lifestyle changes - consider pharmacotherapy |
|
|
Screening as per RED BOOK - frequency, how, age?
Lipids |
5 yrly (2 yrly moderate risk; 1yr if Hugh risk or chronic disease)
Fasting cholesterol, trigs, HDL
45-65 (ATSI >35)
|
|
|
Screening as per RED BOOK - frequency, how, age?
Lipids |
5 yrly (2 yrly moderate risk; 1yr if Hugh risk or chronic disease)
Fasting cholesterol, trigs, HDL
45-65 (ATSI >35)
|
|
|
Screening as per RED BOOK - frequency, how, age?
T2DM |
3 yrly
Fasting BSL - consider OGTT if borderline
40-65+ - ATSI > 18
Advise - lifestyle and dietary changes |
|
|
Screening as per RED BOOK - frequency, how, age?
Stroke risk |
Annually with high absolute risk /AF/AMI/CKD
Ask - symptoms of TIA
> 45+ |
|
|
Screening as per RED BOOK - frequency, how, age?
Stroke risk |
Annually with high absolute risk /AF/AMI/CKD
Ask - symptoms of TIA
> 45+ |
|
|
Screening as per RED BOOK - frequency, how, age?
Kidney disease? |
1-2 yrs in high risk
BP, urine ACR, eGFR - if urine ACR HIGH - repeat 2x for albuminuria over 2 months
>30+
High risk = smokers>40, f.hx, HTN, obesity, DM, ATSI >30 |
|
|
Screening as per RED BOOK - frequency, how, age?
Stroke risk |
Annually with high absolute risk /AF/AMI/CKD
Ask - symptoms of TIA
> 45+ |
|
|
Screening as per RED BOOK - frequency, how, age?
Kidney disease? |
1-2 yrs in high risk
BP, urine ACR, eGFR - if urine ACR HIGH - repeat 2x for albuminuria over 2 months
>30+
High risk = smokers>40, f.hx, HTN, obesity, DM, ATSI >30 |
|
|
Screening as per RED BOOK - frequency, how, age?
Osteoporosis |
Annual
Assess fracture risk factors, BMD
Women > 45+, men >50+
BMD - if indicated but not more than 2 yrly |
|
|
Screening as per RED BOOK - frequency, how, age?
Falls risk |
Annual
Ask - Falls risk factors and falls
All > 65 +
6/13 if high risk - consider OT home review if recent falls |
|
|
Screening as per RED BOOK - frequency, how, age?
Falls risk |
Annual
Ask - Falls risk factors and falls
All > 65 +
6/13 if high risk - consider OT home review if recent falls |
|
|
Screening as per RED BOOK - frequency, how, age?
Hearing and vision |
Annual
Snellen chart, visual fields, hearing test
All >65 yrs
Consider glaucoma assessment if high risk |
|
|
Risk factors for glaucoma ? |
high internal eye pressure > 60 black or Hispanic F.Hx DM, heart disease, HTN + sickle cell eye conditions- nearsightedness eye injury or eye surgery Early estrogen deficiency- before age 43 corticosteroid medications, especially eyedrops, for a long time |
|
|
Screening as per RED BOOK - frequency, how, age?
Falls risk |
Annual
Ask - Falls risk factors and falls
All > 65 +
6/13 if high risk - consider OT home review if recent falls |
|
|
Screening as per RED BOOK - frequency, how, age?
Hearing and vision |
Annual
Snellen chart, visual fields, hearing test
All >65 yrs
Consider glaucoma assessment if high risk |
|
|
Risk factors for glaucoma ? |
high internal eye pressure > 60 black or Hispanic F.Hx DM, heart disease, HTN + sickle cell eye conditions- nearsightedness eye injury or eye surgery Early estrogen deficiency- before age 43 corticosteroid medications, especially eyedrops, for a long time |
|
|
Screening as per red book- age, frequency, how?
Breast cancer |
Mammogram
2 yrly
50-74 (earlier if high risk) |
|
|
Extra immunisations that ATSIs get? |
12-18 months (high risk areas) = Pneumococcal 13vPCV 12-24 months (high risk areas) = Hep A 6/12 - 5 yrs = influenza (All) >15 yrs = influenza (All) >15 yrs = pneumococcal 23vPPV (medically at risk) > 50 yrs Pneumococcal 23PPV |
|
|
People who get government influenza? |
ASTI 6 month-5 yrs ATSI > 15 yrs all Pregnant > 65 yrs old > 6 months with serious medical conditions at risk from complications of influenza |
|
|
Outside the routine schedule - indications for pneumococcal? |
At risk medical conditions 12 months - 13 conjugate (PCV) 4 yrs - 23 polysaccharide (PPV) Oldies > 65 with booster at 5 yrs if medically at risk ATSI - High risk areas - 12-18 months 12vPCV - > 15 medically at risk 23vPPV - > 50 yrs 23vPPV |
|
|
Age for shingles immunisations? |
70 yrs current catch up program until 2021 |