![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
88 Cards in this Set
- Front
- Back
|
what is the target nerve for an inferior alveolar nerve block (IANB)? |
trigeminal nerve, V3 branch -> mandibular branch (has sensory and motor components to it) |
|
|
considerations about IANB |
-close arterial blood flow next to the nerve -> higher risk of arterial aspiration -cortical plate (hard bone) is much more pronounced -> anesthesia doesn't penetrate very well -> supraperiosteal or infiltrative techniques don't work well -wide variation of anatomy -> heigh of mandibular foramen -> higher risk of missed block |
|
|
describe the location and spread of the inferior alveolar nerve |
branch off the trigeminal nerve (V3) -> into mandibular foramen -> courses inside along mandible going through the buccal aspect -> exits the mental foramen and becomes the mental nerve (apical area between 1st and 2nd premolars) |
|
|
what innervates the buccal mucosa molars? |
long buccal nerve -> branch off V3 and courses on the buccal side of the mandible |
|
|
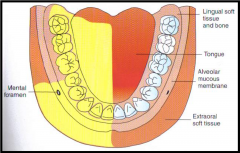
anatomic location of the branches of V3 (mandibular nerve) that innervates the mandible |
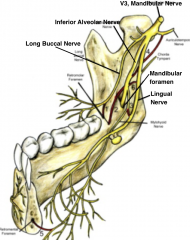
IAN: 1/2 of mandible except for buccal soft tissue adjacent to mandibular molars lingual nerve: anterior 2/3 of tongue long buccal nerve: buccal soft tissue adjacent to mandibular molars |
|
|
what does the mental nerve innervate? |
chin -> soft tissue in chin area, NOT teeth |
|
|
techniques for pupal anesthesia (for teeth) |
-InferiorAlveolar Nerve Block (IANB) -Gow-Gates -Vazirani-Akinosi -Incisive blocks |
|
|
techniques for anesthetizing soft tissue only |
-Mental Nerve Block -Long Buccal Nerve Block -Lingual Nerve Block |
|
|
adjunct techniques for anesthetizing the mandible |
-PDL -Intraosseous -Intraseptal |
|
|
anesthesia technique with the highest percentage of clinical failure |
inferior alveolar nerve block -> 20% failure |
|
|
what other anesthesia technique is usually combined with the IANB usually |
long buccal injection/block |
|
|
what is anesthetize with the IANB? |
entire half of the mandible -inferior alveolar nerve -incisive nerve -mental nerve -lingual nerve -all the teeth of one quadrant (cross innervations of incisors) -body of mandible -> inferior aspect of ramus -buccal mucosa from premolars to the midline -anterior 1/3 or of tongue and floor of mouth (lingual nerve) -lingual mucoperiosteum (lingual nerve) |
|
|
IANB Technique |
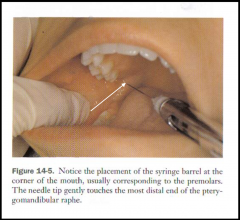
-27 or 25-gauge long needle (yellow) -target: mucous membrane on medial side of ramus -> aim where IAN start to enter into mandibular foramen (area just above entrance) -needle insertion: 3/4 up anterior-posterior, most distal end of the pterygomandibular raphe, on a line to contact the medial aspect of the ramus -penetration: must contact bone, depth between 20-25mm (2/3-3/4 of needle length) |
|
|
Alternative landmarks for IANB technique |
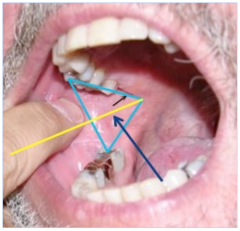
-place middle finger below the ear canal -place thumb on anterior border of ascending ramus (maximum patient opening, retract cheek slightly) -Triangle: base = thumb on anterior border of ramus, upper side = posterior maxilla, lower side = pterygomandibular raphe, bisecting line = base of triangle (thumb) to apex -insertion point: ~5mm in front of thumb on the line to hit your middle finger (in the middle of triangle)
|
|
|
IANB and lingual Nerve Block Technique |
-after bone is contacted, withdraw syringe 1mm (to avoid subperiosteal injection) -> aspirate -> slowly inject 1/2 capsule (0.9mL) -as the need is removed, continue to inject 1/4 capsule (0.45mL) -wait 20 seconds -> return patient to upright position -> 5-15 minutes for anesthetics to work *note: the lingual nerve will be anesthetized with this injection on the ipsilateral side |
|
|
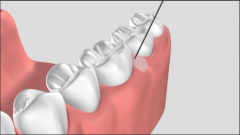
Long buccal nerve block technique |
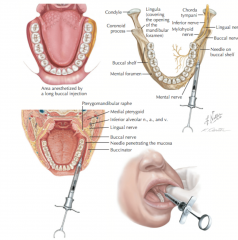
-only use when molar buccal mucosa is involved -> extraction, SRP, deep seated rubber dam clamp, removal of subgingival caries, placement of gingival retraction cord -target: buccal nerve as it passes over the anterior border of ramus -insertion: needle distal and buccal to the most distal molar tooth in arch -penetration: contact bone (2-4mm of needle) -> aspirate -> inject 1/2 capsule (0.45mL) |
|
|
mental nerve block technique |
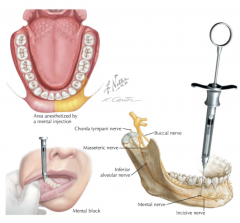
-terminal branch of IAN and provides sensory to boucle soft tissue anterior to mental foramen and soft tissue of lower lip and chin (only soft tissue -> NO pupal) -27 or 25 gauge short needle -target: mental nerve as it exits the mental foramen -insertion: mucobuccal fold at or anterior to mental foramen (can sometimes feel where the nerve exits the mental foramen) -penetration: 5-6mm (don't enter into foramen) -> aspirate -> inject 1/3 cartridge |
|
|
IANB problem -> bone contacted too soon |
-contact bone when penetrating less than 1/2 length of needle -> too car anterior on the ramus -solution: withdraw needle (don't remove completely) -> reorient needle more posteriorly (bring syringe barrel around to the front of the mouth over the canine or lateral incision of contralateral side) |
|
|
IANB problem -> bone NOT contacted |
-needle tip is located too far posterior or medially -solution: withdraw needle so that 1/4 of need still in tissue -> reorient need more anteriorly (bring syringe barrel more posteriorly over the mandibular molars) |
|
|
IANB problem -> Bell's Palsy |
-inject before bone is contacted -> possible that needle is within the tail end of the parotid gland -anesthetize of facial nerve (CN7) -> drooping face (resemble stroke) -> occurs immediately after IANB injection -> should resolve w/in hours |
|
|
IANB problem -> inadequate anesthesia AFTER IANB |
-poor injection technique -anatomic variation -accessory innervation fm nerve to mylohyoid -> need to do Gow-Gates injection -overlapping fibers of the contralateral IAN may ve innervating the central/lateral incisors -> may require supraperiosteal injection to this area -bifid inferior alveolar nerve -> may require IANB more inferior to the normal location |
|
|
solution to inadequate anesthesia |
1. provide anesthesia on the lingual surface of tooth posterior to the tooth in question -> at the apex of 2nd molar if problem tooth is 1st molar for example 2. PDL or intraosseous injection |
|
|
anatomic variation of mandible |
-mandibular flare: difficult to find correct position for an IANB (contact bone right away) -> don't hit bone when repositioning posteriorly |
|
|
complications of anesthetizing the mandible |
-trismus (common) -> from needle piercing the buccinator muscle, medial pterygoid, temoralis, lateral pterygoid (in order from most to least common) -post injection soreness is common -hematoma is rare -transient facial paralysis (Bell's palsy) is very rare |
|
|
4 components of the Armamentarium |
syringe needle cartridge preparation |
|
|
syringe traits |
-durable and withstand repeated sterilization without damage -able to accept variety of cartridge and needles -inexpensive, self-contained, lightweight, simple to use with one hand -provide aspiration so blood can be seen through the glass cartridge -prototypical: aspirating, breech loading, metallic, cartridge-type |
|
|
syringe components |
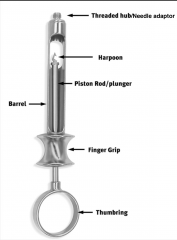
-Thumb ring: permanently attached, can be used to aspirate -Finger grip -Piston -Harpoon: sharp tip attaches to the piston -> penetrates thicker silicone rubber stopper at the other rend of the cartridge (help aspirate) -Barrel -Needle adaptor:needle attaches to barrel via threaded needle adapter -> presses back into the barrel and pierces the diaphragm of cartridge |
|
|
advantages and disadvantages of prototypical dental syringe |
pros: -visible cartridge -one-handed aspiration -autoclavable -resist rust -long lasting -minimal maintenance cons: -reuse permits potential for cross-contamination -> improper cleaning possible -weight -> heavier than plastic -typically only one size -> may be too big/small |
|
|
self-aspirating syringes |
-use elasticity of rubber diaphragm to obtain necessary negative pressure for aspiration -> apply positive pressure to rubber diaphragm when thumb ring is depressed -releasing pressure -> rebound of the cartridge -> negative pressure -> aspiration -small metal projections allows for multiple aspirations |
|
|
pressure PDL syringe (ligajet) |
-special pressure syringes -> useful for intraligamentary injections (PDL) -> used as local anesthesia adjunct and for failed block -can be used to achieve single tooth pupal anesthesia in the mandible but can be painful injection -> unlikely to replace IANB -easy to administer larger volumes of local anesthetic -> produces pain and post-operative discomfort -excessive pressure can shatter glass cartridge -expensive: >$200 |
|
|
(2000psi) pressure jet syringe (medaiet) |
-needle-less injection -> forces local anesthetic liquid through very small openings called "jets" at very high pressure that can penetrate skin or intact mucous membrane -primarily for topical anesthesia -> regional nerve block/supraperiosteal injections -patients complain of soreness in area where 2000psi hit the tissue -accepts any 1.8mL cartridge -> can deliver .05-.2mL at 2000psi -expensive: >$200 |
|
|
advantages and disadvantages of safety syringe |
pros: -protective mechanism -> front collar slides forward, making needle safe -protective plastic sheath over the needle tip locks into place -prevents needle sticks cons: -more $$$ than reusable syringe unit -made to be single use items |
|
|
automated delivery system |
the wand: -automated administration -very slow -> may be less painful -accepts dental cartridges -expensive -extra equipment to purchase/find space for |
|
|
advantages and disadvantages of plastic "medical" syringe |
pros: -cheap -multiple sizes available -disposable cons: -difficult to aspirate -doesn't permit use of dental cartridges and dental needles |
|
|
components of the needle |

-bevel: orient the needle with the bevel facing upwards -> bevel faces the bone upon insertion -shaft: hollow tube -> can bend and kink -hub: metal-plastic interface ->weakest point on needle syringe adapter: threaded to fit onto dental syringe -needle diameter = 1/needle gauge (bigger gauge = smaller diameter) -short needle = 20mm (maxillary infiltration and pediatric patients) -long needle = 32 mm (blocks, adults) |
|
|
types of needle gauge |
-25 gauge (red): ideal when positive aspiration is likely -> less dip deflection, possible increase accuracy -27 gauge long (yellow): use for blocks, most commonly used -30 gauge short (blue): maxillary infiltration, more prone to deflection, for pediatric patients *note: patients can't differentiate between the different gauges -> sizes and pain don't correlate |
|
|
components of dental cartridge |
-aluminum cap -diaphragm (latex rubber) -glass tube -stopper (plunger-silicone rubber) -volume = 1.8mL, actual = ~1.76mL |
|
|
contents inside dental cartridge |
-local anesthetic drug -vasopressor drug = epinephrine/levonordefrin (requires lower pH) -antioxidant = sodium metabisulfite -> preservative for the vasopressor -sodium chloride -> makes solution isotonic -distilled water -> dilutant, provides additional fluid volume |
|
|
contents of local anesthetic |
-concentration give as a percentage -> .05%-4% -converting percentage to mg/ml -> 2% = 20mg/mL -calculating the mg of local anesthetic administered -> concentration x volume = mg/mL x mL example: 1 cartridge of 2% lidocaine plain -concentration -> 2% = 20mg/mL -volume -> 1 cartridge = 1.8mL -mg of anesthetic -> 20mg/mL x 1.8mL = 36 mg of lidocaine |
|
|
contents of vassopresor |
-given as ration: 1:50,000 - 1:200,000 -converting from ratio to mg/mL: 1:50,000 = 0.2mg/1mL -calculating mg of vasopressor -> concentration x volume = mg/mL x mL example: 1 cartridge of 2% lidocaine w/ 1:100,000 epinephrine -concentration -> 1:100,000 = 0.1mg/mL -volumen -> 1 cartridge = 1.8mL -mg of vasopressor -> 0.01mg/mL x 1.8mL = 0.018mg epinephrine |
|
|
color-coded local anesthesia cartridge |

|
|
|
preparation |
-Discuss the procedurewith the patientfirst -Place topical anesthetics -Position the patient appropriately -> right handeddentist operatesat the 8-9:00 position -Professionalapproach-> proper infection control -eye protection is required -Use of a finger rest if needed -Recap the needle and disposeof the needle after injection -> needle AND the cartridge disposed in the sharpscontainer -Reassure the patient -> may take a few minutesto achieve profoundanesthesia |
|
|
specific agents of local anesthetics that are not available in the US |
Procaine (novocaine): withdrawn in 1996 Propoxycaine: withdrawn in 1996 Etidocaine: withdraw in 2002 |
|
|
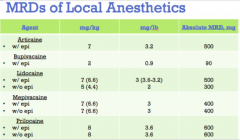
Available Anesthetics in Dental Cartridges in the US as of August2011 -> 5 |
-Articaine HCl: 4% + epinephrine 1:100,000 or 1:200,000 -> intermediate acting -Bupivacaine HCl: 0.5% + epinephrine 1:200,000 -> long lasting -Lidocaine HCl: 2% + epinephrine 1:50,000 or 1:100,000 -> intermediate acting -Mepivacaine HCl: 3% plain -> short acting or 2% + levonordefrin 1:20:000 -> intermediate acting -Prilocaine HCl: 4% plain -> short acting for infiltration or intermediate acting for block, 4% + epinephrine 1:200,000 -> intermediate acting |
|
|
factors affecting duration of action -> 5 |
-individual response to drug -> 70% normal, 15% hyper, 15% hypo -accuracy of deposition of drug -> closer to nerve provides greater duration -status of local tissues -> inflammation, infection, pain, vascularity of tissues -anatomic variation -> height of mandibular foramen, bifid IAN -type of injection administered -> block, supraperiosteal |
|
|
maximum recommended dose (MRD) |
-the point where there is is greater risk of an adverse reaction occurring -typically calculated by body weight given as Mg of drug/unit of body weight (kg or lb) -assumptions: normal body habits/reasonably healthy -should be decreased for people: medically compromised, debilitated, obese, young, elderly -factors influencing distribution and biotransformation: abnormal physiological function (liver, kidney, cardiovascular), blood volume or plasma proteins, injection site |
|
|
How do you determine the maximum recommended dose of each local anesthetic administered inclinical situations where more than one drug is necessary? |
Ensure that the total dose of both local anesthetics combined doesn’t exceedthe lower of the two MRDs for the individual agents |
|
|
MRDs of Local Anesthetics |
-Calculated MRD: weight (lbs or kg) x MRD (mg/lb or mg/kg) -converting lb to kg -> lbs x 0.45 = kg -calculate # of cartridges -> MRD (mg) / (#mg/cartridge) = # of cartridges example: healthy 110lbs patient, drug is 2% lidocaine plain (36mg/cartridge), MRD is 2mg/lb -max drug = 100lb x 2mg/lb = 220mg of drug -# of cartridge = 220mg / (36mg/cartridge) = 6.11 cartridges |
|
|
Provocaine (Novocaine) |
-ester -metabolism: hydrolyzes fast in plasma by pseudocholinesterase -> hepatic dysfunction NOT a problem b/c it's metabolized in blood plasma -excretion: >2% excreted unchanged in urine, 90% broken down into PABA (can cause allergic rxn), 8% broken down into diethylaminoethanol -pH: plain is 5-6.5, vasoconstrictor is 3.5-5.5 -pKA: 9.1 = very slow, 6-10mins to work -half-life: 6 minutes, short duration of action due to vasodilating effects -MRD: 1000mg -effective dental concentrations: 2-4% -> 2% procain plain provides NO plural anesthesia, 15-30 mins of soft tissue anesthesia *note: is the STRONGEST vasodilator of all current local anesthetics -> used to break arteriospasms |
|
|
Articane (Septocaine) |
-amide -> has thiophene and ester groups -vasodilation is equal to lidocaine -metabolism: in plasma via hydrolysis by plasma esterases and in hepatic (kidneys) via microsomal enzymes -excretion: via kidneys -> 5-19% excretion unchanged -pH: vasoconstrictor = 3.5-4 -pKa: 7.8 = faster than lidocaine, 2-3mins onset -half-lief: elimination after 1/2 hour -infiltration: ~ 60mins of pulpal -MRD: 7mg/kg, 500mg max -effective dental conc': 4% + 1:100,000 or 1:200, 000 epinephrine -allergy: very rare -not used in children less than 4 years old -not recommended for regional or mandibular blocks -> esp IAN/lingual blocks b/c prilocane and article have been associated with parasthesia (pricking sensation) |
|
|
Bupivacaine (Marcaine) |
-is an amide -metabolism: hepatic (kidneys) -> via amidases -excretion: via kidneys -> 16% excretion unchanged -pH: plain = 4.5-6, vasoconstrictor = 3-4.5 -pKa: 8.1 = slower onset than lidocaine, onset after 6-10mins -half-life: elimination after 2.7hours -strong vasodilator -potent and strong protein binding -> pulpal anesthesia last for 1.5-3hours, soft tissue for 4-9hours -MRD: 2,g/kg, 90mg max -effective dental conc': 0.5% with 1:200,000 epic -NO topical anesthetic activity -ideal use: procedures where post-operative pain is likely, pain management, initial reduction of need for oral pain meds, -RARELY used in children or mentally handicapped patients -> group have difficulty copping with numbness, may bite or chew their lip/cheek/tongue |
|
|
Lidocaine (Xylocaine) |
-is an amide -provides more rapid/profound anesthesia and longer duration/potency than procaine -metabolism: hepatic (kidney) by microsomal fixed-function oxidases -> byproducts are xylidine and monoethylglycine -excretion: via kidneys -> less than 10% excretion is unchanged -pH: plain = 6.5, vasoconstrictor = 5-5.5 -pKa: 7.9 = rapid onset -> provides anesthesia w/in 2-3 mins -half-life: ~10mins -> depends on vascularity -elimination: ~90mins -vasodilating: more than prilocaine or mepivacaine but less than procaine -MRD: plain = 300mg (5mg/kg), vasoconstrictor = 500mg (7mg/kg) -effective dental concentrations: 2% plain, 2% + 1:50,000 or 1:100,000 or 1:200,000 epinephrine => there is no difference with depth and duration of tissues but there is a difference with degree of hemostasis (stopping of blood flow) -2% + 1:50,000 epinephrine is only recommended for providing hemostasis |
|
|
Mepivacaine (Carbocaine, Polocaine) |
-is an amide -metabolism: hepatic (kidneys) via microsomal fixed-function oxidases -> hydroxylation and N-demethylation -excretion: via kidneys -> 1-16% excretion is unchanged -pH: plain = 4.5, vasoconstrictor = 3-3.5 -pKa: 7.6 = faster onset than lidocaine, onset after 1.5-2mins -very slight vasodilation -> pulpal anesthesia last for 20-40mins -MRD: 7mg/kg, 400mg total -effective concentration: 3% plain, 2% w/ vasoconstrictor -allergies to amides are rare (1 in a million) -3% plain -> indicated for patients with contraindications to vasoconstrictors (cardiac hypertensive patients), commonly used for pediatric patients (faster onset) |
|
|
Prilocaine (Citanest) |
-is an amide -less vasodilating than lidocaine -metabolism: hepatic (kidneys) hydrolyzed by amidases (orthotoludine, N-propylalanine) -excretion: via kidneys, <1% excretion unchanged -pH: plain = 6.5, vasoconstrictor = 3-4 -pKa: 7.9 = same as lidocaine, onset is 2-4mins -half-life: elimination after 1.6 hours -infiltration: 10-15mins of pulpal anesthesia, 1.5-2 hours of soft tissue anesthesia -regional block: 60 mins of pulpal, 2-4 hours of soft tissue -MRD: 8mg/kg, 600mg total -effective dental concentration: 4% olain -allergies: very rare -NO topical anesthetic activity -> EMLA cream is exception -indication: patients contraindicated for vasoconstrictors (cardiac/hypertensive, idiopathic/congenital methemoglobinemia, sickle cell, anemias and hypoxias) |
|
|
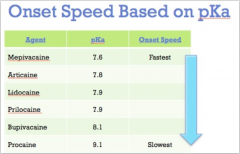
onset speed of different anesthetics (injectables) |
|
|
|
topical anesthetics |
-used prior to needle placement -penetration: 2-3mm deep only -topical conc' is GREATER than injectables -> DO NOT inject topical anesthetics -do not contain vasopressors (anti-hypertensive, reduce bp) -> absorption into blood can be fast -ex: Benzocaine, Butamben, Tetracaine HCl, Cocaine (hospitals only), Dyclonine HCl, Lidocaine (5% concentration) |
|
|
Benzocaine |
-anbesol: max strength = 20% benzocaine, regular strength = 10% benzocaine -use: soft tissue, gingiva, tongue -cons: ineffective for pulpal throbbing/aching, >$6, no toothache pain relief |
|
|
Eutectic Mixture of Local Anesthesias (EMLA) |
-Lidocaine 2.5%, Prilocaine 2.5% -topical action on intact skin -> applied 1 hour before procedure -contraindicated in patients with history of methemoglobinemia -effective for minor surgical procedures in pediatric patients -> IV starts, blood draws |
|
|
Oraqix |
-eutectic mixture of amide local anesthetics -> o Lidocaine 2.5%, Prilocaine 2.5% (single use, glass cartridge of 1.7g) -duration: 14-31mins -oil at room temp. -> administered as liquid-> solidifies at body temp into elastic gel -remains in sulcus until derided out -> doesn't get washed away by water -MRD = 8.5g or 5 cartridges -pH = 7.7 -> relatively basic -> no burning |
|
|
selection of proper local anesthetics |
1. procedure length considerations -short: 3% mepivacaine plain -intermediate: 2% lidocaine with 1:100,000 epi or 4% articain with 1:200,000 epi -long: 0.5% bupivacaine with 1:200,000 epi 2. post-op pain control 3. hemostasis: 1:50,000 epinephrine is used ONLY for hemostasis 4. contraindication |
|
|
list the supplemental injection techniques (9) |
intraosseous injections PDL injections intraseptal injections intraosseous systems intrapulpal injections palatal infiltration V‐2blocks Gow-Gates Akinosi |
|
|
intraosseous anesthesia |
-deposit anesthesia into the cancellous (spongy) bone by bypassing the cortical plate (hard bone) -> bathe nerves as it enders the apex of tooth -do NOT use concentrated epic (1:50,000) -pecking motion with perforator avoids overheating the bone -NO more than 2 cartridges/visit -shorter duration of anesthesia than blocks -avoid in children with mix dentition Pros: -NO chance for positive aspiration -excellent pulpal anesthesia in 30sec -one tooth anesthetize only -> distal to insertion of needle -no "fat lip" |
|
|
Name the three systems used in intraosseous injection and describe the technique |

1. Stabident: used at IUSD 2. X-tip: used at IUSD -> remove from sterile vial and use on slow handpiece -> mark insertion point with cotton pliers (leave small dimple) -> hold perforator perpendicular to cortical plate of bone -> advance perforator until resistance is lost (2 seconds) 3. Intraflow -technique: anesthetize soft tissue -> use perforator (solid needle) make a hole 2mm below the gingiva margin between the two teeth (be distal to the treated tooth and away from mental foramen area) -> insert a 27 gauge needle into the hole to deliver anesthetics -> inject 0.4-0.65mL into the bone when treating o1-2 teeth, inject 1.8mL with multiple teeth in a quadrant |
|
|
PDL injections |
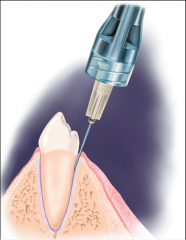
-used for the mandible -> anesthetize bone, soft tissue, and pulp of individual tooth -74% patients prefer this injection (#1 complication is pain when chewing post-op) -anesthetic soln reaches periapical tissues by diffusing apically into marrow spaces surrounding the teeth into interseptal bone -anesthetic soln does not pass through actual PDL fibers -technique: 0.2mL of soln per root (short duration) using 27 gauge short needle -> syringe parallel to long axis of tooth on medial or distal of root -> target on dept of gingival sulcus -> -indication: 1-2 mandibular teeth require numbing, avoidance of bilateral IANBs, children with permanent teeth, nerve block is contraindicated, diagnostic purposes cons: -NOT use on deciduous teeth -> risk of enamel hypoplasia of developing permanent tooth bud -soln taste terrible -needle placement on distal of some mandibular molars is difficult -special syringe may be needed -> requires ample pressure -excessive pressure -> damaged tissue -> post-injection discomforts for 2-3 days and extrusion of tooth with excessive pressure (rare) |
|
|
intraseptal injections |
-useful for soft tissue and periosteal anesthesia -> periodontal procedures (curettage, surgical flap procedure) -poor/brief pulpal anesthesia -technique: 27 gauge short needle -> insert at center of interdental papilla ~2mm below the tip, adjacent to tooth being treated -> enter gingival at 90° angle -> contact bone -> advance 1-2mm into interdental septum (needle tip penetrates bone) -> deposit 0.2-0.4mL of soln pros: -NO chance for positive aspiration |
|
|
intrapulpal injections |
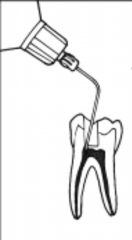
-use as and adjunct when all other technique fave failed or during endo therapy -associated with brief pain upon injection -> intense, instantaneous pain felt by patient -commonly used on mandibular molars -Technique: 25 or 27 gauge short or long needle -> place firmly into pulp chamber (may need to bend needle to gain appropriate access) -> mild/moderate pressure to deliver ~0.2-0.3mL of anesthetic soln Pros: -NO aspiration risk -begin treatment w/in 30sec -profound and immediate anesthesia |
|
|
palatal infiltration |

-anesthetizes the terminal branches of the palate -> greater palatine and nasopalatine -> numbs the soft tissue in immediate vicinity of the injection -indications: hemostasis, palatogingival pain control for rubber dam clamps, retraction cord placement, small surgical procedures *should use the greater palatine block instead |
|
|
V‐2 blocks |

-anesthetize the maxillary division of the trigeminal nerve (V2) -areas covered: pulpal nerves of all teeth of the quadrant, buccal periodontium and bone, soft tissue of bone for hard/soft palate medial to midline, skin of lower eyelid, side of nose, cheek and upper lip -indications: maxillary infection (in canine space, etc), quadrant dentistry, diagnosis for neuralgias, high anxiety patients |
|
|
V2 Nerve block high tuberosity (PSA) approach |
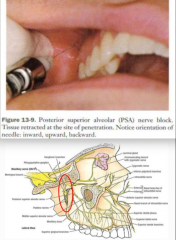
-target: maxillary nerve as it passes through the pterygopalatine fossa -> superior and medial to the target site of the PSA -technique: 25 or 27 gauge long needle -> insert to height of mucobuccal fold (distal to the 2nd molar) -> penetrate a depth of 30mm upwards, inwards and backwards direction about 45° -> needle tip should lie w/in or next to pterygopalatine fossa -> aspirate -> inject 1.8mL -complications: highly vascularized area -> positive aspiration and hematoma |
|
|
V2 Nerve block greater palatine approach |
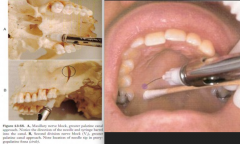
-target: V2 as it passes through the pterygopalatine fossa -> access via the greater palatine canal -technique: perform greater palatine block first with 27 gauge long needle -> find foramen with needle (probe gently) -> advance needle 30mm into canal (5-15% ppl have bony obstructions) -> needle tip in pterygopalatine fossa -> aspirate -> inject 1.8mL soln complications: -local anesthesia into orbit: periorbital swelling/proptosis, block of 6th cranial nerve -> dipole, retrohemorrhage, corneal anesthesia, optic nerve anesthesia -> loss of vision -penetration of nasal cavity (medial wall of pterygopalatine fossa is paper thin): fluid draining down to throat, aspirate large amounts of air |
|
|
Gow-Gates |

-target: medial aspect of condyle, before V3 branches (lingual n., long buccal n., IAN) -> location higher than an IANB -landmark: middle finger in ear canal, thumb on anterior border of ascending ramus (max open & retract cheek) -> triangle base = thumb, triangle upper side = posterior maxilla, triangle lower side = pterygomandibular raphe -insertion point: apex of triangle -penetration: contact bone should be at medial condyle -> aspirate -> inject -issues: may hit coronoid process instead of condyle if don't have patient opening at max |
|
|
Akinosi block |
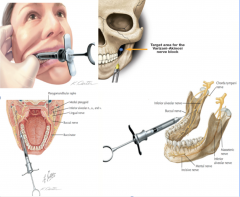
-indication: patients that can't open maximally b/c of truisms ,mandibular fracture, inter maxillary fixation, or TMD -> technique doesn't require patten to open -target: medial aspect of condyle, before V3 branches (lingual n., long buccal n., IAN) -> location higher than an IANB -> between gow-gates and the IANB -insertion: mucogingical junction of maxillary 2nd or 3rd molar -> medial to mandible -penetration: ~25mm depth -> may need to flare laterally while moving posteriorly |
|
|
name 2 injection techniques where you can bend the needle |
PDL injection and intrapulpal injection -bending is acceptable because needle can be easily retrieved if separated -only bend needle once |
|
|
which combination of injections would it require to get the same effects as a V2 nerve block> |
-PSA -ASA/MSA -Greater palatine -Nasoplatine |
|
|
anesthesia local complication: needle breakage |
-causes: sudden unexpected movement of patient -> occurs more with smaller needles and more with bent needles -problem: irretrivability -> difficult to get out when buried in soft tissue -visible needle: tell patient to remain still and remove fragment with hemostat/needle forceps -NOT visible needle: DON'T surgically explore -> refer to OMS for consult and inform malpractice carrier |
|
|
anesthesia local complication: Pain/Burning on Injection |
-causes: rapid injection, vasoconstrictor lowers pH (acidic = burning), dull/barbed needles -prevention: use proper technique and new needles (after 2-3 injections) |
|
|
anesthesia local complication: Persistent Anesthesia or Paresthesia |
-causes: trauma from needle or local anesthetic soln (the higher the conc' the more neurotoxic) -persistent anesthesia -> increase risk of self-injury (burns, biting) -perisisten paresthesia -> altered sensation (hyperesthesia/pricking, Dysesthesia/unpleasant sensation -> similar to when your leg falls asleep -prevention: proper technique, always have informed consent -> most resolve w/in 8 weeks -protocol: reassure patient and speak with them personally -> record initial findings (degree and extent) -> follow-up periodically (every 2 months for 1 year) -> refer to OMS or neurologist if still present *note: do NOT use articaine for IANB b/c of risk for permanent paresthesia |
|
|
anesthesia local complication: Trismus |
-restricted ability to maximally open mouth -causes: trauma to muscle of mastication -> edema or hemorrhage -problem: acute = muscle spasm or limitation of movements, chronic = fibrosis or scar contracture -prevention: proper technique, avoid multiple needle insertions management: palliative care -cold compress initial -> alternate hot/cold 20 mins on/20mins off) -salt water rinse -analgesics = NSAIDs -> reduce pain and inflammation -physical therapy NO improvement: -consider infection after 48 hours -> antibiotics -referral to OMS for evaluation |
|
|
anesthesia local complication: Hematoma |
-bleeding into extravascular spaces -> stop once pressure equalizes -causes: nicking of blood vessel during PSA or IANB for example -problem: rarely leads to significant problems -prevention: proper technique, minimize needle probing -management: direct pressure for 2+ mins, note findings and inform patients, palliative care as needed, time |
|
|
anesthesia local complication: facial nerve paralysis |
-accidental blockage of nerve fibers innervating muscles -causes: incorrect needle placement (at tail of parotid glad or infraorbital block) or infiltration of local anesthetics (maxillary canines) -problem: typically transient (soft tissue numb for duration of local anesthetics), unable to completely close eyelid -> corneal dryness and irritation -> take eyes closed -management: evaluate patient's motor and sensory responses (rule out CVA/stroke, common sense), reassure patients, take eye precautions (eye patch or tape eye closed) |
|
|
anesthesia local complication: soft tissue injury |
-self-inflicted trauma to lips and/or tongue -causes: inability to sense pain when biting and chewing not these tissues -prevention: remind patients not to chew or bite their lip -> avoid hot foods/liquids until sensation returns -managment: analgesics as needed, antibiotics rarely used, sutures very rarely used |
|
|
anesthesia local complication: tissue sloughing |
-ischemia of soft tissue leading to epithelial desquamation or sterile abscess -causes: palatal injection (local anesthetics with vasoconstrictor), prolonged topical application -prevention: use as recommended only (1-2mins, small does about 1/5 cartridge, avoid concentrated vasoconstrictors if possible) |
|
|
anesthesia systemic complication: adverse drug rxn -> overdose |
-absolute or relative over-administration of a drug -> excess drug levels in blood or target organs -this is the MOST COMMON type of adverse drug reaction -> ~99% -causes: slow metabolism (liver disease), slow elimination (renal disease), excessive total dose (exceed MRD), rapid absorption in to circulation (no vasoconstrictors or accidental intravascular injection) -signs: local anesthetics (CNS effects), vasoconstrictor (cardio effects i.e. increase HR and BP)-management: mild = monitor patient, palliative care, release when back to baseline. severe = activate EMS, provide basic life support till help arrives predisposing factors: 1. patient: age, weight, other meds, sex, presence of disease, genetics,, mental attitude and environment 2. durg: vasoactivity, concentration, doase, rout of administration, rate of injection, vascularity of injection site, presence f vasoconstrictors |
|
|
anesthesia systemic complication: adverse drug rxn -> allergy |
-hypersensitivity set following previous exposure to allergen -> not related to dose or drug levels -incident: ~15% rxn requiring emergent care -local anesthetic allergy: ester allergy is more common (PABA, type 4/delayed hypersensitivity more common), amide allergy extremely rare (more likely from overdose than true allergy) -vasoconstrictor allergy: epinephrine (no true allergy exist) -other allergy: methylparaben (preservative but NOT used in dentistry), metabisulfite (antioxidant with vasoconstrictors) -prevention: accurate/updated medical history and have epi pen or epi vial ready -for elective care -> postpone until clergy can be determined -for emergency care -> non-invasive treatment, general anesthesia, histamine blockers as alternative (diphenhydramine/Benadryl) |
|
|
types of allergy and it's management |
anaphylatic = IgE mediated, immediate -> massive vasodilation fm release of histamine -managment of type I anaphylaxis = avoid the offending agent, activate EMS, basic life support (epinephrine intramuscularly or IV ) cytotoxic = IgG or IgM immune complex = IgG -> 6-8hours delayed hypersensitivity -> 24-48 hours -management = avoid the offending agent, palliative care (antibiotics rarely used) |
|
|
anesthesia systemic complication: adverse drug rxn -> Idiosyncratic reactions |
-qualitatively abnormal or unexpected result -> Benadryl is normally a sedating drug but in some ppl it can make them hyper -> very unpredictable results -not dose related -not a true allergy |
|
|
preoperative necessities for medical-legal issues |
-complete and thorough review of medical history (meds, surgeries, allergies, dental, social concerns i.e. alcohol, tobacco and drugs) -document each appointment -> review med history changes, preoperative vital signs (BP, HR), treatment plan consent (verbal and written) -CHART EVERYTHING |
|
|
additional documentation |
-total does of ALL drugs administered -> administered36mg of 2% lidocaine with .018mg epinephrin -techniques used -> performing right IAN and long buccal block -how patients responded -> profound anesthesia, pt. tolerated tx well, etc. -abnormal findings -> DOCUMENT -verify documentation of assistant -additional notes -> write in PEN, spell words correctly, DON'T white-out errors |