![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
155 Cards in this Set
- Front
- Back
|
motor unit |
single lower motor neuron and all the muscle fibres that it controls - not all motor neurons are the same size |
|
|
neuromuscular junction |
a synapse or junction between an axon terminal of a motor neuron and muscle fibres |
|
|
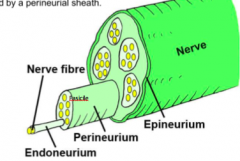
bundle of axons in the CNS- tract in the PNS - nerve |
|
|

|
8 cervical nerves (C1-C8) 12 throacic nerves (T1-T12) 5 Lumbar (L1-L5) 5 Sacral nerves (S1-S5) 1 coccygeal Nerve |
|
|
myotome dermatime |
group of muscles that a single spinal nerve inovates area of skin that is mainly supplied by a single spinal nerve |
|
|
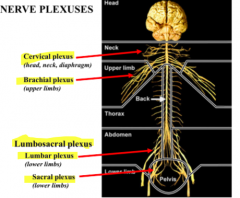
peripheral nerve often comprised of multiple spinal nerves- eg. Brachial plexus (braid like a plexus) |
|
|
|
musculocutaneous nerve |
C5 and C6 Biceps brachi Brachialis and Coraco- brachialis (anterior forearm) |
|
|
Median nerve |
c5, c6, c7, c8, t1 thumb and first 2 fingers and half of palm |
|
|
ulnar nerve |
C8, T1 two small fingers and half of palm |
|
|
Radial nerve |
C5, C6, C7, C8, T1 lower biceps and back of full arm |
|
|
axillary nerve |
C5, C6 upper arm (badge area) |
|
|
Cranial nerves |
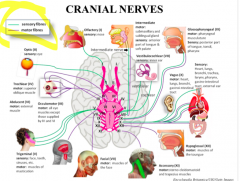
1. Olfactory 2. Optic 3. Oculomotor 4. Trochlear 5. Trigeminal 6. Abducens 7. Facial 8. Vestibulo-cochlear 9. Glossopharyngeal 10. vagus 11. Accessory 12. Hypoglossal |
|
|
sympathetic nerves come from the throacic (middle) part of the spinal cord |
parasympathetic comes from the cervical and lumbar regions of the spinal cord |
|
|

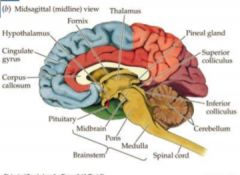
brainstem: located in the diencephalon (interbrain) and the spinal cord |
|
|
the motot homunculus (percentral gyrus) |
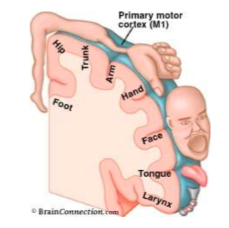
the size of the cortical surface responsible for t a part of the body is proportional to the degree of motor control needed for that part |
|
|
|
|
|
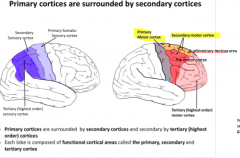
Apraxia |
'lack of practise' lesions in motor areas outside the primary motor cortex |
|
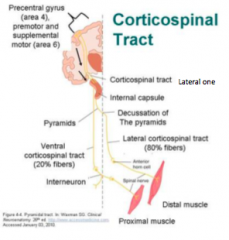
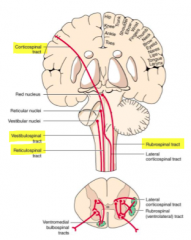
Corticospinal Tracts- Pyramidal system |
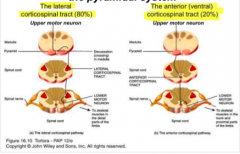
lateral corticospinal tract (80%) crosses over at the decussation in medulla Anterior (ventral) corticospinal tract (20%) crosses over in the spinal cord |
|
|
Decussation of the pyramids- cross at the medullary pryamids |
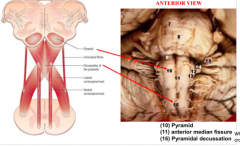
when the anterior median fissure dissapears- the fibres are crossing = decussation of the pyramids |
|
crossing over in the spinal cord |

|
|
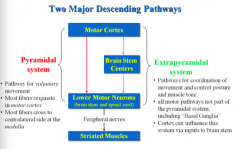
Pyramidal system - pathway for voluntary movement - most fibres originate in the motor cortex most fibres cross to the contralateral side at the medulla |
Extrapyramidal system - pathways for coordingation of movement and control posture and muscle tone - all motor pathways nto part of the pyramidal system (basal ganglia) - cortex can influence this system via inputs to brain stem |
|
|
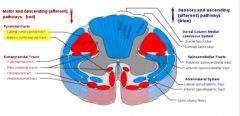
pyramidal system: - voluntary movements - direct pathways to influence lower motor neurons |
Extrapyramidal system
- control and refinement of movements - involuntary movements (posture and support) - indirect pathways to influence lower MNs - tracts found in reticular formation of pons and medulla - involvement of basal ganglia, midbrain nuclei and cerebellum |
|
|
Rubrospinal Tract |
red nucleus of midbrain to spinal cord largely terminates in the cervical spinal cord lateral column of the spinal cord |
|
|
Reticulospinal tract |
pons and medulla reticular formation travel lateral (medulla and anterior (pons) important for POSTURE |
|
|
vestibulospinal tract |
vestibular nuclei (medulla and pons) (junciton btw pons and medulla) travels anterior lower limb muscle |
|
|
tectospinal tract |
midbrain colliculi (4 bodies that define the back of the midbrain) travels anterior automatic postural movements of head in response to visual and auditory stimuli |
|
|
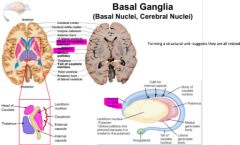
Basal Ganglia |
Cerebral nuclei - Globus Pallidus - Putamen - Caudate Nucleus = Corpus Striatum midbrain nuclei: substantia nigra subthalamic nucleu feed back via the cerebellum |
|
|

head of the cordate sitting right up against the globus palidus and the thalamus next to the internal capsual |
|

subthalamic nucleus STN- green bit beneath the thalamus sight where deep brain stimulation (parkinsons) |
- located in the diencephalon ventral to thalamus - functionally part of the basal ganglia - anatomically not because its part of the diencephalon - gluammatergic neurons (excitatory) |
|
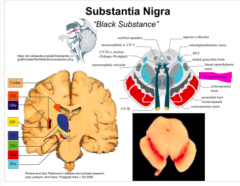
Substantia Nigra black because of pigments in the neurons in that region - important in motor control destroyed or damaged in parkinsons patients |
- located in the midbrain - motor planning and movement pars compacta - dopaminergic neurons - appears black due to neuromelanin pars reticulata - GABAergic neurons - neurons less densely packed |
|
|
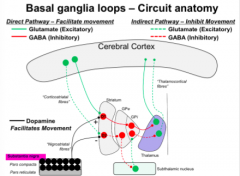
basal ganglia loops - direct pathway |
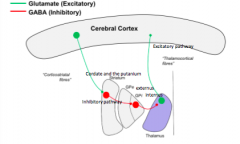
Epu gets inhibited unable to maintain inhibition of the thalamic neurons so they are allowed to be active and loop back to provide feedback direct pathway promotes motor pathway profide excitatory drive to the primary motor neurons |
|
|
basal ganglia loops- indirect pathway dotted lines |

inhibitory pathway inputs into the striatum project to the Gpe- those neurons are all inhibitory and then project down to the subthalamic nucleus glutamatergenic neurons excitatory project back into the Gpi and then rest of the pathway is the same which will then inhibit the final output (excitation of the inhibition) |
|
|
dopamageric neurons that project up to the striatum D1 is excitatory when it finds dopamine it excites D2 is an inhibitory when it finds dopamine |
|
|
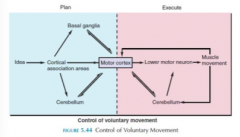
Cerebellum - essential for fine movement - regulates feedback to refine movement |
|
|
|
cervical lordosis theoracic kyphosis lumbar lordosis sacral kyphosis |
bad = HYPER lordotic or kyotic |
|
|
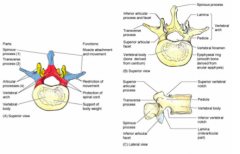
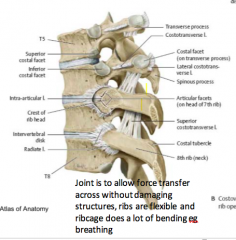
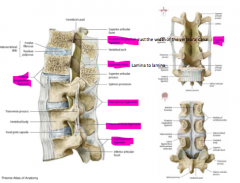
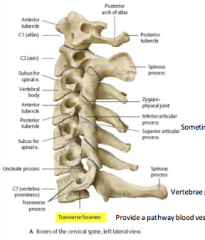
pedicle + lamina = neural arch articular facet- bit on the end that forms the joint spinous process- top of this in a persons back |
|
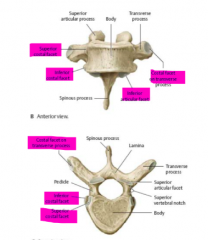
thoracic vertebae all have ribs attached very elongated spinous process lumbar process- much larger and kidney shaped - denser spinous process |
|
|

|
|
|
|
epidural veins- metasticies work their way up - convergent from other veins in the body |
not much movement in the thoracic vertebra lots in the cervicalfew in the lumbar - mostly just hips and legs |
|
|
clinical: should have two cores - if failure to fuse = spina bifida also a cause of congenital scoliosis |
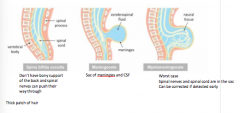
spina bifida: most common neural tube defect the neural tube forms but the supporting tissue does not |
|
|
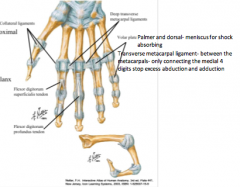
intervertebral disc: nucleus pulposus anulus fibrosus |
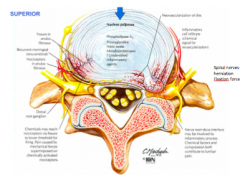
usually herniates posteriorly - spinal nerves very close by |
|
|
|
|
|
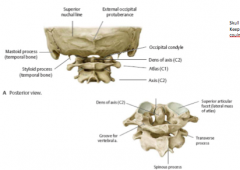
C1 and C2 ATYPICAL vertebrae sometimes a split in the spinous proccess- to make bifed shape- allows for greater muscle attachement in the suboccipital triangle |
|
|
C1 (atlas) - rotates upon the Axis vertebrae C2 (axis) |
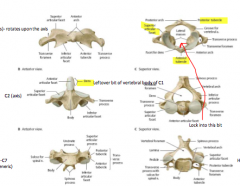
c1= doesnt have vertebral body- instead there is an anterior tubercle C2- has an anterior articular facet that locks into the space shown in the C1 |
|
|
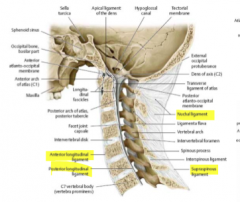
nuchalligament- evolutionary leftover- important for quadrapede- helps hold the neck up eg like cows and horses not hugely functional or supportive in humans |
|
|
skill only connected to skeleton be 2 index finger spaces between skull and atlas |
|
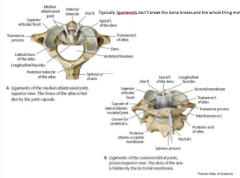
typically the ligaments dont break the bones do |

if the triangle bit is broken- skull can move freely from the spin BIG PROBLEM spinous process in C2 can puncture spinal cord = dead |
|
|
uncinate processes |
develop throughout adult life some people think that pathology of too much or too little neck movement |
|
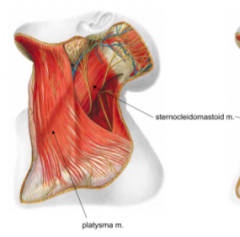
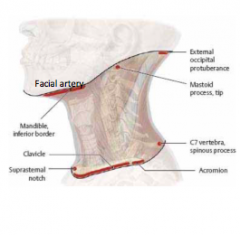
platysma m. : muslces of facial expression innovated by facial nerve contracted means that you look aggressive |
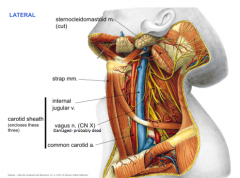
sternocleidomastoid m : divides a lot of things from sternum and clavacal --> up to mastoid process and wraps around the back of the skull use it to name jugular veins makes chin stay level by pulling on the back of the skull |
|
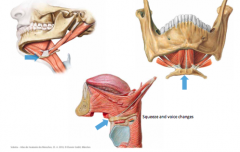
hyoid bone |
|
|
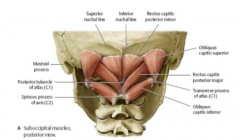
suboccipital triangle mm |
bifed spinous proccess gives greater leverage for having muscles attach this triangle- muscles that keep the head balanced from side to side |
|
|
investing fascia- wraps all around the muslces |
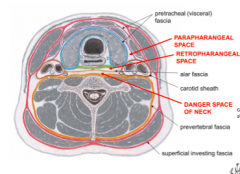
Danger space- goes from base of skull to diaphragm- infection can spread along the entire body |
|
|
X-Rays vacuum tube with current between a filament and target- shadows on film |
interact with electrons: E-density of tissues (essentially a map of electron densities) Pros: - cheap - available - excellent spacial resolution cons: - ionising radiation - rel. poor contrast resolution - planar technique 3D becomes 2D often initial exam bones chest for breathing problems etc. |
|
|
Fluoroscopy X-ray tube runs continuously can see motion |
HEAPS of ionising radiation |
|
|
CT scan X-rays constantly rotating producing multiple projections |
continuous spiral 3D data set can cut in any direction and colourise with colour pros: -x-sectional - better contrast resolution than X-ray - good spacial resolution cons: - more ionising radiation - expensive used in acute symptoms- trauma, stroke cancer |
|
|
ultrasound high frequency radio waves that distort the piezoelectric Crystal and produces an electric current - can be reversed |
pros: - NO ionising radiation - cheaper than CT - freely available - sold v cystic cons: - operator dependent - sound penetration problems , bone, fat, gas used: children and pregnancy blood vessels muscles, tendons |
|
|
Magnetic Resonance imagining MRI very strong magnet and radio wave generator need a faraday cage (copper lined room) so that FM radio waves only on magnet and not from actual radio |
good map of the water content in body pros: - NO ionising radiation - Excellent contrast resolution - reasonable spatial resolution Cons: - expensive - strong magnet - ferromagnetic materials - long scan times - claustrophobia - air/ calcification/ metal distort the magnetic field used: brain, spine |
|
|
Nuclear medicine inject radio isotope into the body labelled with a pharmaceutical uses gama rays |
signal to noise difference concept to image contrast very goot at targetting specific organ accumulation of radiopharmaceutical in the organ of intrest c/w rest of the body used: functional cardiac imaging bones for trauma or tumour renal imaging thyroid imaging |
|
|
Positron emission tomography PET using a positron emitter rather than a traditional gama ray emitter |
Uses: Glucose analogue -see what the function is Concology scanning Brain for epilepsy Cardiac for ischemia Novel positronemitters Radiopharmaceuticals PSMA (prostate- specific membrane antigen PiB (extracellular beta-amyloid binding) |
|
|
ionising radiation - dangerous non-ionising- US or MRI |
ALARA as low as reasonabily achievable |
|
|
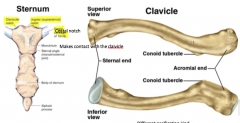
- one of first bones to start ossification --> one of the last to finish (21-25 years old) - easy to age an individual long bones doesnt have a medullary cavitiy but DOES have bone marrow S shaped bone lateral end dips doward- acromial end sits superior to sternal end inferior end has tuberosities other end is smooth |
|
|
fracture of the clavicle |
common when weight bearing breakage ususally midshaft- when broken the medial side moves upwards and lateral downwards when broken pectorals major pulls arm inwards and clibing of the medial end shifts over the lateral end |
|
|
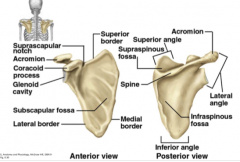
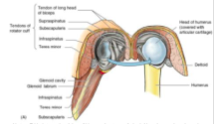
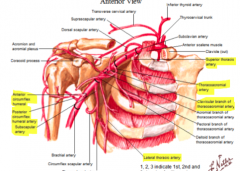
shoulder joint is unstable but EXTREMLY mobile supraglenoid cavity- short head of the biceps infraglenoid cavity- long head of the biceps Suprascapular notch-has suprascapular ligament Below ligament -suprascaular nerve Above-suprascapular artery Bits of the scapulathe get fractured easily are the bits that are pointing out |
|
|
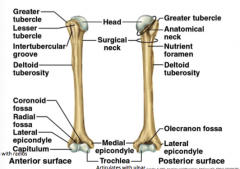
only about 1/3 of the head fits within the glenoid cavity surgical neck- part that typically gets fractured |
|
|
fracture of the humerus |
surgical neck - axillary nerve (travells with the posterior medial humoral artery midshaft- supracondylar- median nerve and brachial artery medial epicondyle- ulnar nerve |
|
|
Fascial compartments |
anterior- flexor posterior - extensor epimycium goes onto become fascia forms internusclular septer fascia encircling arm --> antibrachial fascia in the forearm--> palmer apopneurosis and connective tissue in tendons |
|
|
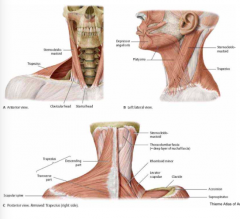
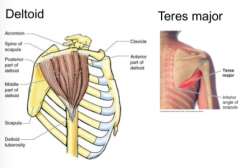
superficial back muscles: trapezius- function on limb - retract the scapula lower fibres- pull scapula downwards superior fibres- pull scapula upwards allows glenoid cavity to rotate latissimus dorsi narrows into tendon (intertubecular tube) on humours from thoracic and lumbar fascia medial rotation, adduction |
levetor scapulae: skull to scapula Rhomboid minor Rhomboid major typically minor is superior |
|
|
pectoral muscles: 2 important ones Pectorals major serratus anterior: inserts onto vertebral board of the scapula back of ribs and inserts onto anterior vertebral body of scapula |

|
|
|
Intrinsic shoulder muscles: deltoid teres major supraspinatus infraspinatus teres minor subscapularis |
|
|
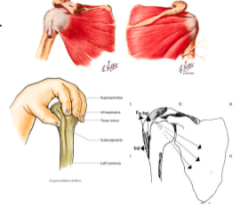
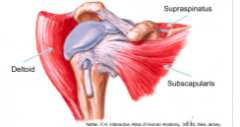
rotator cuff muslces: supraspinatus infraspinatus teres minor subscapularis |
holds the head of the humerous against the glenoid cavity work as fixators often described as dynamic ligaments |
|
|
rotator cuff injuries |
frozen shoulder- 'adhesive capsulitis' impingement of supraspinatus |
|
|
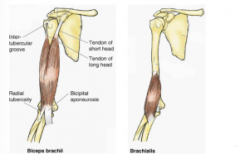
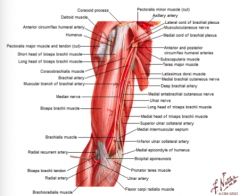
anterior compartment of the arm |
biceps coracobrachialis- inflextion of the shoulder joint brachialis - originates on the shaft of the hummerus - works on the elbow joint all supplied by musculocutaineous nerve |
|
|
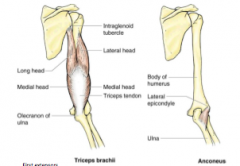
posterior compartment of arm: triceps anconeus - supplied by radial nerve - passes between medial and lateral heads - susceptible to injury in mid-shaft fractures of humerus |
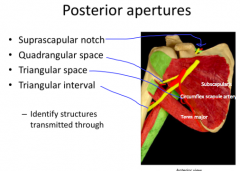
1. subscapular artery goes above the ligament and nerve goes below 2. formed between long head of the tricepts and the shaft of the humerus and teres major 3. 4. radial nerve, endangered in the midshaft fracture teres minor on the posterior side of the scapular |
|
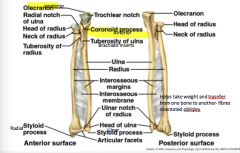
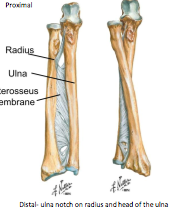
ulnar: longer of the two flat on top when flexed the coranoid process fits in the coranoid fossa distal end has disc shape- head of the ulna sharp edge- for interocious membrane |
radius: makes contact at the distal end sustains the weight when falling disc shaped head of the radius shaft has sharp edge where interocious membrane inserts wide distal end ulnar notch radial styloid process |
|
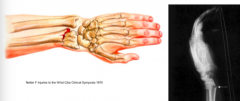
'colles' fracture of radius distal end sticks backward 'dinner fork' more likely to fracture radius |
fracture of ulna - when defending yourself- parry fracture high impact fracture- eg. fall from motocycle volkmans ischaemia |
|
|
cubital fossa: b/w medial and lateral epicondyles, pronator teres and brachioradialis roof: biceptal aponeurosis floor: Brachialis m. |
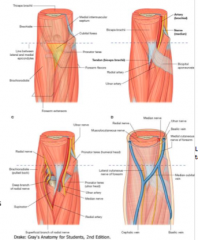
contains: median cubital vein cutaneous nerves ulnar and radial arteries medial and radial nerves |
|
|
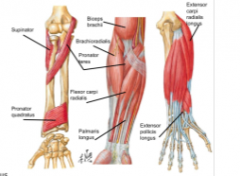
anterior flexor comptarment (forearm) -superficial PFPF - intermediate FDS deep FPL, FDP, PQ |

superficial: pronator teres flexor carpi radialis palmaris longus flexor carpi ulnaris intermediate: flexor digitorum superficialis deep: flexor policies longus flexor digitorum profundus pronator quadratus |
|
|
pronators: pronator teres pronator quadratus both pronate forearm |
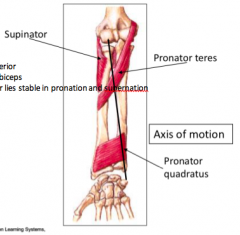
supinator supination is the more powerful action also produced by biceps supinator |
|
|
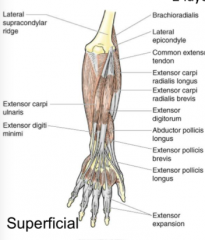
posterior extensor compartment superficial: - brachioradialis: supracondyle ridge of radius- inserts at the distal end of the radius- helps flex - extensor carpi radialis longus (ECRL) - extensor carpi radialis brevis (ECRB) - extensor digitorum communis (EDC) - extensor digiti minimi (EDM) - extensor carpi unlaris (ECU) - anconeus |
|
|
|
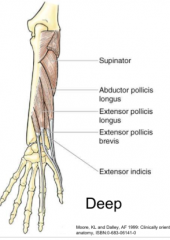
deep: - supinator - abductor pollicis longus (APL) - extensor pollicies brevis (EPB) - entensor pollicies longus (EPL) - extensor indicis (EI) |
|
|
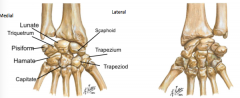
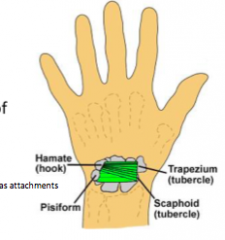
Carpal bones two rows 8 bones scaphoid most fragile |
scaphoid- boat shaped- constriction (waist, gets fractured) lunate: moon shaped triquetrum pisiform- sesimoid bone SLTRIP trapezium- contact with first metacarpal (saddle joint- allows opposition) trapezoid capitate: proximal end has a head- distal end has artciular facet hamate: has a hook (hook of hamate) TRACH |
|
|
scaphoid fracture blood supply to the proximal half compromised - becomes necrotic |
hook of hamate fracture: or compression when holding things (eg raquet sports) ulna nerve and uln artery nearby - important in the intrinsic muscles of the hand |
|
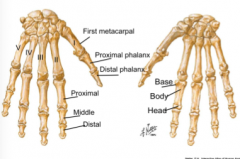
Metacarpals |
long bones- base, shaft and head first one- shortest and most robust(thumb) distal- thickening on distal end for fingernails |
|
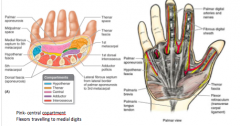
infection in synovial sheets can be contained - if in bursa it may or may not spread infection in little finger- can go to the ulna bursa |
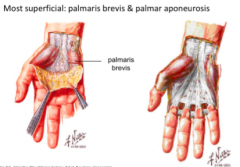
palmer aponeurosis divides palm into three compartments contracture of palmar fascia- (dupuytrens) thickening and shrinking- two littlest fingers contract |
|
flexor retinaculcum (band retainer) - OR transverse carpal ligament holds tendons in place forms roof of carpal tunnel |
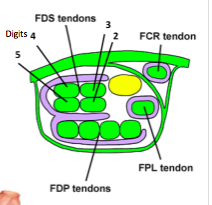
carpal tunnel flexor retinaculum = roof proximal end identified by distal wrist crease contents: - flexor tendons - synovial sheaths - median nerve |
|
|
superficial to flexor retinaculum -PL tendon - ulnar artery and nerve - superficial branch of radial artery - palmar cutaneous branch of median nerve - FCU tendon - wellll medial |
|
|
|
deep to flexor retinaculum - FDS (x4 tendons) - FDP (x 4 tendons) - FPL - Median nerve ( recurrent thenar branch, lateral & medial branches) - FCR (within roof of carpal tunnel) - synovial sheaths |
superficialis - tendons split insert on the distal phalanges |
|
|
extensor retinaculum attachments: - radius laterally - triquetrum, pisiform, FCU tendon medially |
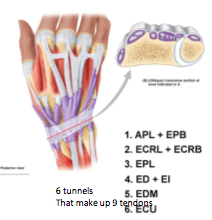
contents: 6 tunnels 9 tendons synovial sheaths |
|
|
snuff box: boundaries anteriorly tendons: APL, EPB posteriorly: EPL tendon roof: skin, subcutaneous tissue, cephalic vein, radial nerve, superficial br. Floor: scaphoid, trapezium |

contents: radial artery - digs itself deeper to the tendons of the APL and EPB and deeper to the tendon of the EPL - deepest strucutre in that space - travels onto the palmer side |
|
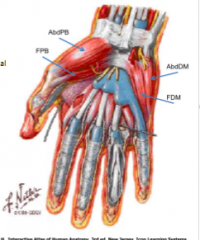
intrinsic muscles of the hand: layer 1 thenar muscles: - abductor pollicies brevis (abdPB) - flexor pollicis brevis (FPB) hypothenar muscles - abductor difiti minimi (abdDM) - flexor digiti minimi (FDM) --> arise from edges of flexor retinaculum --> insert into base of proximal phalanx |

layer 2: lumbricals (x4): - arise from FDP tendons - pass to lateral side of digit - insert (dorsally) into ext expansion (2-5) flex the metacarpal phalgeal jonts extent the interphalangeal joints |
|
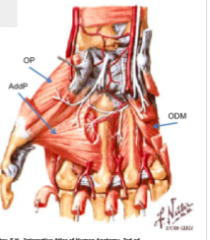
layer 3: thenar muscles: - opponens pollicies (OP)- innovated by the recurrent branch of the medial nerve - adductor pollicies (addP) (fan shapped muscle in 1st web space - starts from 3rd metacarple- innovated by the ulnar nerve Hypothenar muscles - opponens digiti minimi (ODM) --> arise from edges of flexor retinaculum --> inserts along borders of MC |
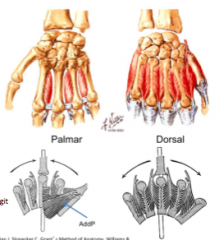
layer 4: interoissei - 3 palmer (adduct; pAd) - 4 dorsal (abduct; dAb) arise from MCs pass to lateral side of digit insert into extensor expansion digits 1-4 |
|

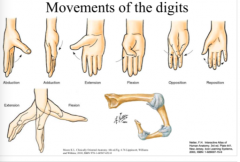
nerve supply |
|
|
|
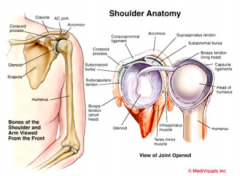
shoulder complex pectoral girdle - manubrium of sternum - clavicle - scapula humerus highly mobile joint |
joints of the shoulder three TRUE bi-articular (synovial joints) - sternoclavicular - acromioclavicular - glenohumeral two physiolofical (functional) joints - subdeltoid - scapulotheoracic |
|
|
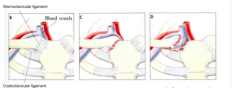
sternoclavicular (SC) joint - saddle joint - articular disc -dislocation uncommon blood supply: - internal thoracic - suprascapular nerve supply - nerve to subclavius |
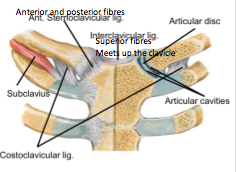
ligaments - sternoclavicular: sternum and clavicle - interclavicular- superior fibres, meet up the clavicle costoclavicular- from rib to the base of the clavicle- extrinsic to joint but still provides support allow elevation and depression - protraction of the scapula and retraction |
|
sternoclaviclar subluxation usually direct trauma to front of chest if clavicle depressed against rib cage- artery and blood vessels - life threatening |
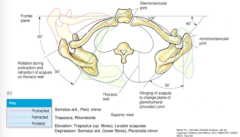
clavicular movements at the SC and AC joints elevation- trapesius when scapular spine goes upwards glenoid cavity goes downwards serates anterior- call pull away the scapula from the midline- spine is facing upwards |
|
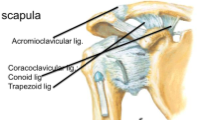
Acromioclavicular (AC) joint - connects acromial end of clavicle with scapula - plane joint intrinsic ligament - acromioclavicular joint extrinsic ligament - caracoclaviclar conoid: inserts at the base of the clavicle (wider here)- sagital plane- vertially orientated, stops upward migration of the clavicle trapezoid: horizontally orientated- clavicle doesn't deviate too far away with protraction and retraction |
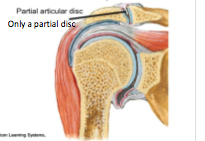
- partial articular disc shoulder separation in contact sports blood supply: - suprascapular - throacoacromial nerve supply: - suprasclaviclar - lateral pectorial - axillary |
|
|
scromioclavicular dislocation: shoulder separation: grade 1- A-C legaments stretched but NOT torn coracoclaviclar ligaments intact grade 2 - A-C ligaments torn and distrupted. coracoclaviclar ligaments remin intant joint mobility still possible grade 3 - A-C & coracoclaviclar ligaments ruptured wide separation of joint |
|
|
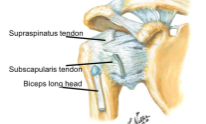
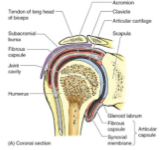
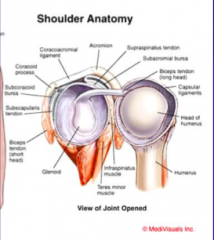
Glenohumeral (GH) joint - glenoid cavity and head of humerus - synovial ball-and-socket joint - poor congruence b/w articular surfaces- glenoid cavity only takes in 1/3 of the sphere- gets deeper with help of fibrocartilagenous disc - tendon of long head of biceps has intrascapula origin- takes with it a wrapping of synocial membrane allowing fluid action |
blood supply: circumflex humeral arteries nerve supply: suprascapular, axillary, lateral pectoral |
|
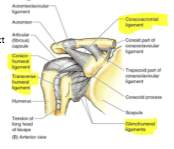
ligaments of the GH joint intrinsic: - coracohumeral- provides support from posterior aspect - glenohumeral- between regions- slight openings allow place for synovial fluid to make contact with bursa |
extrinsic ligaments - coracoacromial- superior support - transverse humeral - keeps tendon of biceps in place rotator cuff muscles as dynamic ligaments deficiencies - anterior glenohumeral ligaments - inferior articular capsule - anterolateral long head of biceps |
|
|
mobility at GH joint: HIGH mobility reduced stability rotator cuff muscles act as fixator ligaments greatest stability during abduction and external rotation - also position for dislocation |

|
|
|
physiological joints subdeltoid: b/w supraspinatus and GH joint supacromial bursa painful arc syndrome scapulothoracic b/w serratus and thorax b/w serratus and scapula glenohumeral rhythm: scapula and humerus 1:2 ratio (scapula moves 30 degrees then humerus does 60) |
subacromial bursa located under acromion process of the scapula susceptible to irritation during shoulder abduction |
|
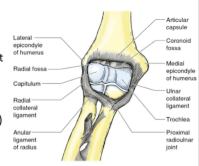
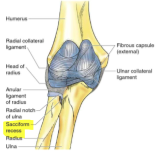
Elbow joint: compound joint b/w humerus, ulna and radius hinge joint capsule houses two distinct joints: - elbow - proximal radioulnar only in complete flexion do you have contact with radius and humerus |
no articular disc (meniscus) blood supply: branches of brachial artery nerve supply: musculocutaneous, radio, ulnar |
|
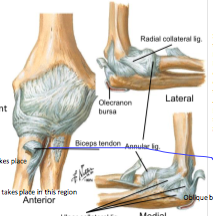
ligaments of elbow joint: ulnar collateral ligament 3 bands - anterior - posterior - oblique radial collateral ligament - blends with annular ligament |
articular capsule lax anteriorly and posteriorly fat pads: - olecranon, radial, coronoid olecranon bursa starts at the lateral epicondyl of the humreus, blends with the lateral colateral ligament does NOT blend with the band of the radius- just blends with the annular ligament - allows pivot if blended would stop pronation and supranation |
|
|
movements at elbow joint: flexion mostly between hummerus and ulna radial contact at close-packed position |
extions oblique angle of trochlea carrying angle adults> children females > males- possibly due to wider hips |
|
flexion muscles at elbow joint help with supernation- most effective when elbow is flexed |
extension muscles at elbow joint: |
|
|
Radioulnar joints at each end of radius proximal: b/w radial notch on ulna and head of the radius distal: ulna notch on radius and head of the ulna pronation and supination |
interosseous membrane transmits forces - at proximal end only 20% through radius - at distal end 80% force placed on teh radius are transmitted to the ulna fraction at one end may lead to dislocation at the other end |
|
proximal radioulnar joint b/w head of radius and radial notch of ulna pivot, synovial joint within elbow joint capsule |
sacciform recess- gets tight so that the joint is stable- but when supine then the recess will be lax nerve supply: musculocutaneous, radial blood supply: branches of deep radial and radial arteries |
|
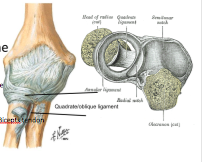
ligaments of proximal radioulnar joint - annular ligament- part of the lateral/colateral ligament - quadrate ligament - interosseous membrane - extrinsic support ring ligament on the lateral end of the ulna loose enought to allow the head of the radius to rotate |
movements at radioulnar joints pronation/ supination flexion/ extension midprone position most stable |
|
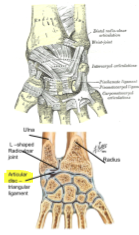
distal radioulnar joint between head of ulna and ulnar notch on radius pivot, synovial ligaments: anterior and posterior |
articular disc- triangular ligament sacciform recess nerve supply: median and radial interosseous nerves blood supply: anterior, posterior interosseous arteries |
|
|
muscles moving radioulnar joints: pronation: - pronator teres - pronator quadratus - assisted by flexor carpi radiallis palmaris longus brachioradialis |
supination - supinator - biceps brachii - assisted by: extensor pollicis longus extensor carpi radialis longus |
|
|
dislocating proximal radioulnar joint - annula ligament lax in children - radial head displaced - muscle pulls radial head superiorly reduction supinate forearm, push proximally, joint in flexion |
clinical considerations - bursitis - epicondylitis (lateral = tennis elbow, medial = golfers elbow) - avulsion fractures supracondylar fracture of humerus |
|
|
glenohumeral joint: multi-directional joint, mobile, prone to wear and tear (also hips and knees) prone to instability ball and socket joint |
|
|
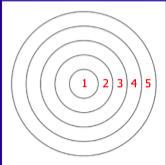
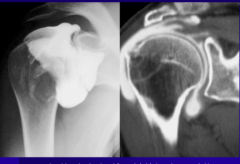
radiographic anatomy 1. bones 2. labrum - deepens the socket 3. capsule- ligamentous thickenings 4. tendons - rotator cuff 5. bones (others) |
|
|
|
GH joint pathology fracture arthritis- destruction of articular cartilage frozen shoulder (adhesive capsulitis) rotator cuff tears |

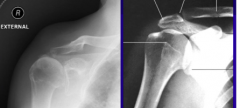
1.head of clavicle 2. acromium 3. greater tuberosity 4. lesser tuberosity 5. surgical neck of the humerus 6. shaft of the humerus 7. coracoid proccess of the scapula 8. blade of scapula 9. rib |
|
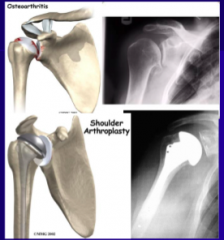
osteoarthritis- wear and tear lose articular cartilage and then secondary change in the bone thickens up and beoce osteophites |
instability: joint extended beyond its normal range traumatic or spontaneous problem in labrum and capsule |
|
|
dislocation complete displacement of the joint articular surfaces subluxation incomplete displacement of the joint articular surfaces usually anterior- fall rarely posterior- seizure |
anterior dislocation - rips the anterior capsule from its attachent to the glenoid rim - rips inferior GH ligament attachement to the labrum - CT/MRI best to see damage |
|
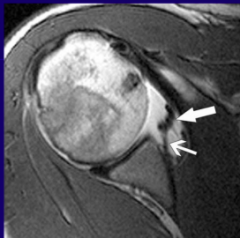
contrast injected into the joint CT- better for bones MRI- better for the soft tissue |
joint capsule - capsule is a sac that encloses the joint - though, fibrous outer membrane - inner synovial membrane (w synovial fluid) - shoulder joint capsule is loose enough to allow a wide range of motion |
|
|
adhesive capsulitis (frozen shoulder) adhesions grow across the joint surfaces capsule contracts problem in capsule restricting motion - takes physio therapy |
try and blow the capsule up like a balloon to allow movement - doesnt work if capsule is fully torn (distension arthrogram) |
|
|
rotator cuff wear and tear older age leads to tendinopathy |
tendinopath (tendinosis) - rarely inflammatory degeneration of fibres micro-tears results in: upward movement of the humerus impingement of rotator cuff against bone can cause irritation to bursa and acromion (can wear away) damage depends on the shape of the acromium |
|
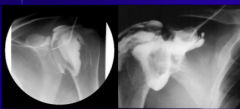
arthrogram - way to see tears (as well as US) inject contrast into the joint see if it leaks from the joint into the subacromial bursa |
tendinosis can cause the Geyser phenomenon where movement of upwards humerus causes fluid to form a lump on the top of the shoulder |
|
|
radiocarpal joint between distal radius and scaphoid, lunate, triquetrum |
|
|
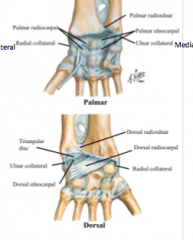
ligaments: medial collateral lateral collateral palmer and dorsal radiocarpal palmerand dorsal radioulnar |
tricangular fibrocartilaginous disc blood supply: branches of palmer and dorsal carpal arches innervation: anterior: branch of median nerve posterior: branch of radial nerve |
|
|
flexion: FCR, FCU, FDS, FDP, FPL, PL, APL extension ECRL, ECRB, ECU, ED, EI, EDM, EPL, EPB |
radial deviation (abduction) APL, FCR, ECRL ulnar deviation (adduction) ECU, FCU |
|
|
intercarpal joints between carpal bones proximal and distal row joint capsule same as CMC joints ligaments: anterior, posterior, interosseous (strengthening ligaments) Blood: palmer and dorsal carpal arches Nerve: anterior interosseous, deep branch of ulna |
midcarpal joint: functional joint convex-concave condyloid type movement - flexion/extension radial deviation> ulnar deviation |
|
|
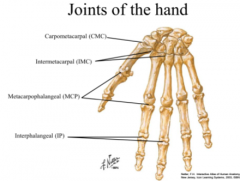
CMC and IMC (carpals and metacarpals) all synovial CMC 2nd, 3rd plane (immobile)- trapazoid and capitate 4th, 5th hinge (ring and little finger) - allows to make a fist 1st saddle (own synovial cavity) IMC= plane joints |
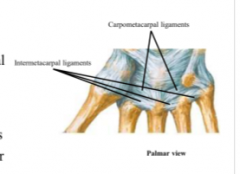
CMC and IMC ligaments - interosseous and collateral |
|
|
MCP bw head of metacarpal, bas of proximal phalanx condyloid ligaments: collateral ligaments transverse metacarpal ligaments palmer plate dorsal plate modified hinge |
interphalangeal (IP) bw head of proximally placed phalanx and base of distal hinges |
|

finger injuries: skiers thumb- rupture of medial collateral ligament from forced abduction and extension |
|
|
|
common flexor sheath - tendons of FDS - tendons of FDP - tendons of FPL digital synovial sheaths fibrous digital sheaths NO little finger sheath no sheath where lumbricles are attached (threat of spreading infection) |
fibrous flexor sheats annular fibres cruciform fibres spread of infection in synovial sheath |
|

median nerve (C5-T1) supplies most muscles of anterior compartment of forearm hand of benediction |
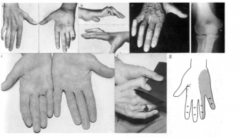
ulnar nerce (C8, T1) supplies muslces in anterior compartment of forearma nd head except for thumb susceptible to compression against handlebar of bike |
|
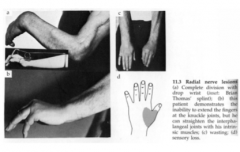
radial nerve (C5-T1) extensor muscles of arm and forearm |
|
|
|
torque capacity of a muscle is determined by its moment arm |
moment arm = distance of the muscle force from the joint centre of rotation |
|
|
torque = force X motor arm |
muscle shortens and generates torque- muscle has to have a lever arm muscles that have larger motor arms have larger levers and are more effective GH has the largest lever arm |
|
|
tendon excursion method- measure motor arm tendon excursion vs joint angle = instantaneous moment arm (gradient) |
if can measure the vertical translation of the weight = tendon excursion tendon excursion vs joint angle = tendon excursion |
|
|
greatest lever is the supraspinatus - good initiatory of abduction and deltoid |
neg motor arm - latissimus dorsi - depressor of the shoulder or extensor opposite of deltoid adduction |
|
|
about 70% of over 70 years old have rotator cuff tear means shoulder is not stable- good chance of shoulder joint will dislocate - very painful as well |
try to take tendon and stitch it back to the bone (via anchors which sit in the bone permanently2 (dingle row) or 4 (double row) anchors) double row provides best repair if tear--> wont use shoulder --> arthritis (cartilage dies) --> osteoarthritis = cuff tear arthropath |
|
|
cuff tear arthropathy - reverse shoulder arthroplasty ball becomes the socket and the socket becomes the ball - reverse the anatomy of the joint joint centre changes and can double the moment arm = half the effort by the deltoid to rotate the arm |
creates a lot of superior sheer (undesirable) can provide a risk factor irreparable tear = left it too long and the muscle has gone fatty |
|
|
limb buds from the lateral aspect of the cavity takes budding ventral rami |
usually C5-T1 prefix brachial plexus C4-C8 postfix C6-T2 |
|

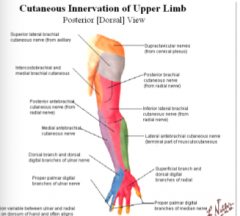
anterior division fibre- flexor muscles of the upper limb (anterior) and skin overlying them |
posterior divisionsfibres- extensor muscles and the skin overlyng them |
|
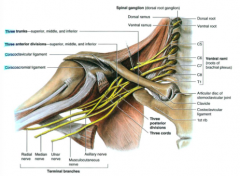
upper, middle and lower trunk formed above the clavicle divisions- happens behind the clavicle cords- develop inferior to the clavicle |
lateral and medial cord visible. (according to relationship with artery) M shape- makes up terminal branches from the medial and lateral cord lateral M- pericing coracobrachialis - musculocutaneous nerve (lateral cord) middle M- median nerve (medial and lateral cord) lateral M- ulnar nerve arises from medial cord - continues down medial side of the arm and epicondyle |
|
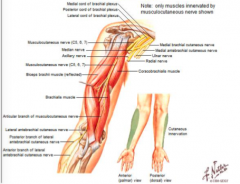
Musculocutaneous nerve |
- perices coracobrachilais becomes cutaneous at elbow- lateral to tendon of biceps --> lateral cutaneous nerve of forearm motor supply to anterior part of the arm cutaneous distal to the anterior compartment of the arm |
|
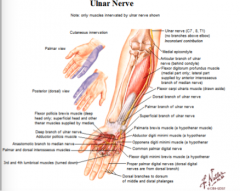
Ulnar nerve |
medial limb of M sometimes gets contribution from C7 (cant predict with drawing) medial to axillary artery- goes behind the medial epicondyl--> goes through 2 heads of FCU--> down ulnar on medial side under FCU between FDP --> superior to flexor retinaculum (near psiform) supplies: intrinsic muscles of hand, some hypthenar, medial 2 lumbricles, interoissei and adductor policies (shares thenar muscle supply with median nerve) and FCU and FDP (medial half) |
|
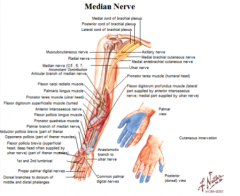
Median nerve |
all ventral rami- medial and lateral cords starts on top of the artery- crosses the arty and comes to lie medial to the artery --> between two heads of pronator teres --> runs down middle with FDS above and FDP below--> goes through carpal tunnel--> gives cutaneous supply before flexor retinaculum (goes above) --> goes past thenar muscles- recurrent branch of meidan nerve
supplies every muscle in anterior forearm except FCU and half of FDP , lateral 2 lumbricles shares supply of thenar Cutaneous supply-thumb- sencond, thrid and lateral side of 4th Dorsal of hand- onlydoes the nailbeds |
|
|
only one posterior cord- all division fibres in it sits deep to the artery |
Axillary nerve- penetrates above teres major radial nerve- comes out below |
|
|
Axillary nerve C5, C6 above teres major- main nerve supply to deltoid and teres minor |
passes beneath shoulder joint- very vulnerable in dislocation (lose abduction because loss of deltoid) cutaneous supply over deltoid |
|
|
radial nerve- biggest nerve in the upper limb all roots of brachial plexus beneath teres major (triangular space) b/w long head of biceps and shaft of humerus gives off braches early- tricept branches VERY early nerve is vulnerable becuase near bone (fracture or compression) |

main motor branch to the extensor compartment of the forearm--> posterior interosseous nerve
enters posterior interosseous membrane through 2 heads of the suppernator and settles onto the back of the interosseous membrane supplies: all muscles in the extensor compartment superficial branch of the radial nerve- slips lateral before elbow to supply lateral side of the forearm through anatomical snuff box from under the tendon of brachio radialus SKIN supplies cutaneous: 3 lateral fingers on palmer and dorsal but NOT the nail beds |
|

|
|
|
proximal C5,6 supply proximal parts of the limb c8,T1 supply distal parts |
damaging the neck- can damage the brachial plexus figure out weather the brachial plexus is damaged or terminal nerves etc. |
|
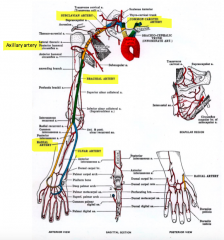
single stem artery- feeding into the limb at or below the middle point divides into 2 main branches |
always runs down the flexor aspect (anterior upper limb) always a rich anastamoses around the joints to compromise for any kinks around the joint area |
|
Axillary artery: supplies axillary walls- branches related to anterior and posterior axillar walls |
changes name at the inferior boarder of the teres major goes beneath pec minor important relationship to brachial plexus M shape for nerves arranged over the anterior of the artery |
|
|
Brachial artery: ends at cubital fossa directly anterior to distal head of hummerus starts medial to humerus and ends directly anterior--> goes onto become lateral |
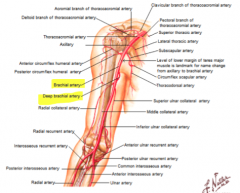
contributes to anastamoses around elbow and shoulder joint brachial artery branch = profunda deep brachial artery--> posterior compartment of the arm (tricepts) runs with the radial nerve in neurovascular bundle |
|
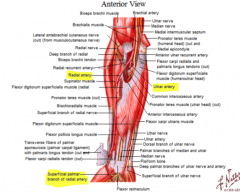
radial nerve: runs down with the radial nerve under the cover of brachio radialus- lateral to the humerus runs over the back of the hand goes through the anatomical snuff box - gives off superficial palmer arch |
radial NERVE- turns onto back of hand near the snuff box to supply the skin to the back of the hand |
|
ulna artery: medial side of the anterior forearm runs with ulnar nerve under the cover of FCU OVER the FR- next to psiform bone and forms superficial palmer arch |
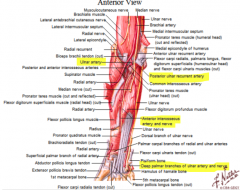
gives off (ver soon after origin) common interosseous artery --> splits into two gives rise to anterior and posterior interossius membrane and goes either side additional blood supply to deep and central structures posterior interosseous artery goes with posterior interosseus nerve (branch of radial nerve) |
|

ulnar- superficial palmer arch can be a hockey stick (just stop) or join with the radius gives rise to digital arteries |
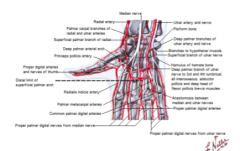
radial artery = deep palmer arch gives rise to metacarpal arteries |
|
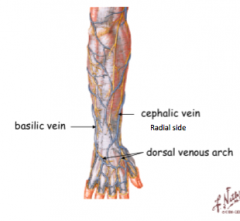
superficial and deep veins anastamose freely with each other deep veins run with arteries both have valvues venus arch- bulk blood from the palm of the hand from gripping |

basilic vein and cephalic vein = superficial cephalic- runs all the way up through pectoral groove and then joins the axillary vein basilic vein - goes halfway up the arm- perices the deep fascia and joins deep brachial veins and join the axillary vein |
|
|
deep veins follow the arteries- beneath the middle joint its not a single vein is pared vena comentanties- distal veins- pared proximal to joint = single vein |
lymph- drains into axillary lymph nodes inlcudes all arm and upper quadrant of chest including brest (breast cancer) also drains axillary wall |