![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
94 Cards in this Set
- Front
- Back
|
When are screening exams performed? |
when the patient's primary subjective complaint is related to an extremity or a part of the spine Think "spine - screen" |
|
|
what should be examined if there is an UE complaint? What if there is a LE complaint? |
if UE complaint: cervical and thoracic spine should be examined if LE complaint: lumbar spine and pelvis should be examined |
|
|
what are components of the lower quarter screening exam in standing? |

1. postural assessment 2. active forward, backward, and lateral bending of lumbar spine 3. standing flexion test/ Gillet's test 4. Toe Raises (S1, tibial nn) 5. heel walking (L4, L5 deep fibular nerve) |
|
|
what are the components of the lower quarter screening exam in sitting? |
1. sitting flexion test 2. active rotation of the lumbar spine 3. passive OP if symptom free 4. resisted hip flexion (L1, L2, femoral nn) 5. resisted knee ext (L3, L4, femoral nn) 6. Resisted ankle DF (L4, L5 deep fibular nn) 7. resisted big toe ext (L5 deep fibular nn) 8. resisted ankle eversion (L5, S1 superficial peroneal nn) 9. DTR: patellar (L3, L4) and Achilles tendon (S1, S2) |
|
|
What are the components of the lower quarter screening exam in supine? |
1. dermatome sensory testing 2. SLR (L4, L5; S1) 3. Passive ROM of hip 4. Sciatic nn tension test |
|
|
What are the components of the lower quarter screening exam in prone? |
1. Femoral nn tension test
2. Babinski reflex test (UMN) |
|
|
What are the components of the upper quarter screening exam? |
1. Postural assessment 2. AROM cervical spine 3. Passive OP if symptom free 4. Vertebral artery test 5. Quadrant test 6. resisted mm tests cervical spine rotation (C1) 7. Resisted shoulder elevation (C2, C3, C4) 8. Resisted shoulder abduction (C5) 9. Active shoulder flexion, abduction, IR, ER 10. Resisted elbow flexion (C6) 11. Resisted elbow ext (C7) 12. AROM of elbow 13. Resisted wrist flexion (C7) 14. Resisted wrist ext (C6) 15. Resisted thumb ext (C8) 16. Resisted finger abduction (T1) 17. Babinski Reflex test (UMN) |
|
|
What is the accessory mobility scale? |
-complete joint play/ testing of joint mobility when the joint capsule is most relaxed or in the loose packed position 0 Ankylosed joint 1 considerable limitation/hypomobility 2 slight limitation/hypomobility 3 Normal 4 slight hypermobility 5 considerable hypermobility 6 Pathologically Unstable |
|
|
What are the 4 possible findings of resisted mm testing? and what does each indicate? |
1. strong and painless: no pathology in contractile tissue 2. Strong and painful: minor structural lesion of the muscle-tendon unit 3. Weak and painless: complete rupture of muscle-tendon unit or neuro deficit present. Further testing is needed 4. WEak and painful: partial disruption of muscle-tendon unit. Pain response due to serious pathology or concurrent neurological deficit |
|
|
How can you differentiate the action of a one-joint muscle from that of a multi-joint muscle? |
place the multi-joint mm at a disadvantage -if a muscle that crosses two or more joints produces simultaneous movement at all of the joints it crosses, it soon reaches a length at which it cannot generate full mm force = active insufficiency |
|
|
What is active insufficiency? |
Decrease in torque produced by a muscle when the full ROM is attempted simultaneously at all joints crossed by the multi-joint mm ex: hand grasp with wrist in full flexion |
|
|
What is passive insufficiency? |
-when 2-joint or multi-joint muscles are of insufficient extensibility to allow full ROM to be produced simultaneously at all joints crossed by these muscles. -passive tension developed in these stretched muscles is sufficient to either cause motion or to limit motion: ex: cause motion: full wrist flexion causes fingers to extend due to insufficient length of finger extensors stretched over flexed wrist ex: limit motion: finger flexion with wrist flexion is limited by length of finger extensors; or -rectus femoris limits active knee flexion with hip extended -HS limits active knee ext if hip in position of flexion |
|
|
what are the MMT grades? |
Normal = 5/5 can move into test position against gravity with maximal resistance Good = 4/5 Same as normal but can only resist moderate pressure Fair + = 3+/5 Same as Good but can resist only mild pressure Fair = 3/5 full range against gravity, no resistance Fair - = 3-/5 Same as fair but gradual release against gravity Poor + = 2+/5 Moves against gravity in small ROM Poor = 2/5 Full ROM in gravity eliminated position Poor - = 2-/5 can only initiate ROM with gravity eliminated Trace = 1/5 Fasciculation or palpable mm contraction but unable to move Zero= 0 No visible or palpable mm contraction |
|
|
What are components of the Neurological examination? |
1. resisted muscle testing 2. sensory testing 3. DTRs 4. Neural tension tests 5. UMN testing (babinski and ankle clonus) |
|
|
Describe signs and symptoms that differentiate UMN vs LMN lesions |

|
|
|
When is further testing required during the sensory testing portion of the neurological exam? |
-if light touch is different between sides or there is a decr in LT over a specific area then further testing is required -such as pin prick (superficial pain), vibration, two-point discrimination, or proprioception |
|
|
What is the grading scale for DTRs? |
4+ = Hyperactive reflex with clonus (indicates UMN disorder) 3+ = Hyperreflexia (brisk): palpable (mod-strong) contraction with exaggerated joint movement (still within normal variation) 2+ = Normal = palpable ctx with visible extremity movement 1+ = hyporeflexia (sluggish) palpable mm ctx with no extremity movement (indicative of LMN disorder) 0 = Areflexia (absent) no visible or palpable mm ctx |
|
|
What is the purpose of neural tension tests? |
by stretching the peripheral nerves with specific body movements, the mobility of the spinal dura and nerve roots can be tested |
|
|
What (in general) nerve does the SLR test bias? What are the variations? |
sciatic nerve 1. Passive SLR with DF and eversion = tibial nn 2. Passive SLR with PF and inversion = peroneal nn 3. Passive SLR with DF and inversion = sural nn DET PIP DIS
|
|
|
What neural tension test biases the femoral nerve/ |
Prone knee bend |
|
|
What neural tension test biases the spinal dura? |
passive neck flexion |
|
|
How is ankle clonus test performed? |
Position leg in slight knee flexion and rapidly DF ankle (+) test if series of involuntary mm contractions |
|
|
how is the babinski test performed? |
stroke the plantar aspect of the foot from the lateral side of the heel to the base of the great toe with a blunt instrument (+) great toe DFs and other toes fan out |
|
|
What test should be performed before any manual treatment of the cervical spine? |
vertebral artery test and must be repeated as ROM increases |
|
|
What is the vertebral artery test? |
-assesses integrity of the vertebrobasilar vascular system -pt in supine and progress as below 1. extend head and neck for 30 secs. if no change progress to next step 2. extend head and neck with rotation left the for 30 sec then repeat with right rot for 30 sec (+) test provokes referring symptoms (Right rot will decr contralat artery and reproduce L symptoms and vice versa) - pt should report tinnitus, dizziness, nausea, throbbing, confusion, or unsual sensation. and Clinician obesrves for pupillary constriction or dilation and nystagmus which indicate VA compression |
|
|
What should be done if the Vertebral artery test is positive? |
avoid mobilization and cervical spine movements into ext and rot at ranges that produce symptoms -notify physician of test findings |
|
|
What cervical motions test intervertebral foramen vs VA and vice versa? |
IVF: decreased space with extension (blood flow normal with isolated ext) VA: ext + rot = bilat decr with > decr on contral side aa. (IVF > decr on ipsilat side) pg. 193 of McGee |
|
|
What is the quadrant test for the cervical spine? |
= spurling's test/foraminal compression (identifies compression of cervical nerve roots) -perform if pt c/o nerve root symptoms which are diminished or absent at time of exam (i.e. UE symptoms)
|
|
|
Quadrant test and alternatives |
Maximum cervical compression test = (ext + rot + SB + compression) spurling's = foraminal compression (SB head to uninvolved side and add compression straight down. repeat on opposite side) |
|
|
How is Spurling's test performed and positive results? |
SB head to uninvolved side and add compression straight down. -repeat on opposite side (+) test = pain radiates into arm toward which head is side flexed which indicates pressure on a nerve root (cervical radiculitis) (-) = neck pain with no radiating pain |
|
|
How is the maximum cervical compression test performed? |
aka maximum cervical compression test -identifies compression of neural structures at IVF and/or facet dysfunction - patient in sitting -passively move head into SB and rot toward non painful and add ext then compression -repeat on painful side (+) = pain and/or paresthesia in dermatomal pattern on same side as SB and rot or localized pain in neck if facet dysfunction |
|
|
When is the distraction test indicated? |
when pt c/o radicular symptoms in hx and presents with radicular sx during the exam -indicates compression of neural structures at the IVF or facet joint dysfunction |
|
|
How to perform the distraction test? |
supine hold pt under chin and occiput and flex neck whiled distraction force of about 14 pounds applied (+) = decr in symptoms in neck (facet condition) or decr in UE pain (indicating nerve root compression) |
|
|
What is the purpose of Hautant's test? |
-to differentiate vascular vs vestibular causes of dizziness/vertigo |
|
|
Describe positive Hautant's test. |
2 steps 1. sitting with shoulders flexed to 90 and pulms up. Have pt close eyes for 30 sec. If arms lose position = (+) vestibular condition 2. sitting with shoulders flexed to 90 and palms up. close eyes and have pt extend head and neck with R Rot and then L Rot holding in each for 30 sec. (+) for vascular cause if arms lose position |
|
|
What is the purpose of the transverse ligament stress test? |
test integrity of tranverse ligament of C-spine -prevents anterior movement of atlas on axis and posterior movement of axis on atlas |
|
|
What is a positive test for transverse ligament stress test? |
-supine -head on table -glide C1 anterior Normal end feel = firm (+) = soft end-feel, dizziness, nystagmus, lump sensation in throat, nausea |
|
|
What is the purpose of the anterior shear test? |
assess integrity of upper c-spine ligaments and capsule |
|
|
how is anterior shear test performed and positive test? |
-supine with head on table -glide C2-C7 anterior normal end-feel = firm (+) = ligament laxity, dizziness, nystagmus, lump sensation in throat, nausea |
|
|
What is positive Shoulder abduction test? |
(+) = decr in UE symptoms when pt places one hand on top of head Indicates compression of neural structures in IVF |
|
|
What is Lhermitte's sign? |
identifies dysfunction of SC and/or UMN lesion -long sitting -passively flex head and one hip while keeping knee in ext, repeat with other hip (+) pain down the spine and into upper or lower limb = indicates dural or meningeal irritation in spine or possible cervical myelopathy |
|
|
What is the Romberg Test? |
standing close eyes for 30 seconds (+) for UMN lesion if excessive sway or lose of balance |
|
|
What is the standing flexion test? |
-tests iliosacral motion to determine joint dysfunction (motion restriction of innominate) -palpate both PSIS and ask pt to bend forward Normal = both PSIS move superior and anteriorly (+) side with motion restriction is the one that move furthers or first cranially and is considered blocked |
|
|
What is the slump test? |
- sitting on edge of table with knees flexed and hands behind back -pt slump sits while maintaining neutral head and neck. then add progressions below 1. passively flex pt head and neck. if no symptoms then 2. passively extend one of pt knees. If no sx then 3. Passively DF ankle of LE with extended knee Repeat on other side. if positioning reproduces patients symptoms and cervical ext relieves symptoms = (+) for increased tension in the neuromeningeal tract |
|
|
What is the Laseque's test? |
aka SLR supine, passively flex hip of one LE with knee ext until pt complain of shooting pain into LE -slowly lower until pain subsides, then DF ankle -also can add neck flexion (+) = reproduction of pathological neurological symptoms when foot is DF and when neck flexed (+)= asymmetry between sides (+) = reproduction of sx between 35-70 deg hip flexion biases the sciatic and tibial nerves |
|
|
What is Cross (Well Leg) SLR? |
SLR on uninvolved reproduces patient's symptoms -one leg is lifted and pt c/o pain in opposite LE = indication of space-occupying lesion (e.g. herniated disc, large IV disc protrusion) -stretches ipsilateral and contralateral nerve root. |
|
|
What is the femoral nerve traction test? |
-identifies compression of femoral nerve anywhere along its course -sidelying on nonpainful side with unaffected knee and hip slightly flexed (painful side is up) -head/neck slighlty flexed -with affected knee in ext, extend the hip approx 15 deg -if no sx then flex knee (+) = neurological pain radiate down anterior thigh |
|
|
What is the lumbar quadrant test? |
identifies compression of neural structures at IVF and facet dysfunction 1. in standing, for IVF test: SB L, Rot L, and Ext = max closing of IVF on L 2. in standing for Facet dysfunction SB L, Rot R, and Ext = max compression of facets on L (+) = localized pain for facet dysfunciton pain &/or paresthesia in dermatomal pattern for the involved nerve root |
|
|
What is the Prone knee bend test? |
aka femoral nerve stretch -used to identify L1-L3 nerve root lesion (also stretches femoral nn) -prone + passive knee flex + hip ex (+) for nerve root involvement = unilat pain in lateral or posterior aspect of hip, into lumbar spine, or into anterior thigh |
|
|
What is Stork standing test? |
-identifies spondylolisthesis -stand on one leg + lumbar ext and repeat on opp leg (+) = LBP with ipsilateral LE on ground = unilat stress fracture of pars interarticularis |
|
|
What is the Bicycle test of van Gelderen? |
-identifies neurogenic claudication (spinal stenosis) vs intermittent claudication -ride stationary bike sitting erect and time how long can ride at set pace -repeat with slumped posture and time how long -spinal stenosis (+) if can ride longer in slumped posture or if reproduces sx in erect posture which are relieved with slumped posture |
|
|
What is Gillet's test? |
-used to identify SI joint dysfunction -thumb on PSIS and other thumb on sacrum at same level -pt standing then asked to flex hip and knee on side you are palpating -PSIS should move inferiorly (+) = PSIS does not move or moves cranially which indicates ipsilateral motion restriction
If palpate PSIS on WBing side -innominate should rotate posteriorly (PSIS move inferiorly) (+) if PSIS on stance side moves cranially (ant rot) = decr motor control of lumbopelvic stabilizers |
|
|
What is Long-sitting test? |
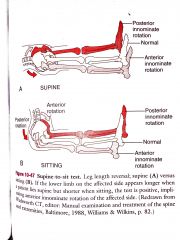
-measures functional leg length -determines if there is a posteriorly or anteriorly rotated innominate based on apparent leg length differences -if LE longer in supine but shorter in sitting = (+) anterior innominate rotation on affected side -if LE shorter in supine and appears longer in sitting = posterior innominate rotation |
|
|
What are the five test that indicate SIJ pain and how many have to be positive? |
3 out of 5 to indicate SIJ pain with high spec and sensitivity 1. Distraction/Gapping 2. Thigh thrust 3. Gaenslen's test 4. Sacral thrust 5. Compression |
|
|
What is the distraction/gapping test? |
SIJ dysfunction (1 of 5 cluster of tests) -supine -cross arm pressure to bilat ASIS in down outward direction (+) = symptoms reproduced or increase in unilat gluteal or in posterior leg |
|
|
What is the thigh thrust test? |
SIJ dysfunction (1 of 5 cluster of tests) supine with hiop flexed to 90 -push posteriorly directed force through femur (+) = Pain incr or reproduced on thrusting |
|
|
What is Gaenslen's test? |
SIJ dysfunction (1 of 5 cluster of tests) supine near edge of the table with affected leg hanging over edge of table -other leg is flexed toward pt's chest -firm pressure is applied to both the hanging leg and the leg flexed toward the chest (+) = pain in the SIJ is reproduced or increased |
|
|
What is the sacral thrust test? |
SIJ dysfunction (1 of 5 cluster of tests) in prone, examiner applies a force vertically downward to the apex of the sacrum (+) = SIJ pain incr or is reproduced |
|
|
What is the compression test? |
SIJ dysfunction (1 of 5 cluster of tests) sidelying with affected side up hips are flexed approx 45 and knees flexed to 90 -vertically force applied downward on ASIS (+) = SIJ pain increases or is reproduced |
|
|
What is the sitting flexion test? |
-identifies SIJ dysfunction -Thumbs on PSIS in sitting -pt crosses arms over chest with feet on floor and bends forward bringing elbows between knees (+) = blocked joint moves first or further cranially |
|
|
What are the tests for impingement in shoulder? |
1. Neer's 2. Hawkins-Kennedy 3. Painful arc |
|
|
What are the tests for RC dysfunction/pathology? |
1. Supraspinatus muscle test 2. Infraspinatus Muscle test 3. Drop Arm Test 4. ER Lag Sign 5. IR Lag Sign 6. Lift off test 7. Belly Press test |
|
|
What are the special tests for AC joint dysfunction/ pathology? |
1. Horizontal Adduction test 2. Resisted Horizontal Extension test 3. O'Brien's Sign 4. Paxinos Sign 5. Palpation of the AC joint |
|
|
What are tests for the GH labrum? |
1. Crank Test 2. Biceps Load I Test 3. Biceps Load II Test 4. Pain Provocation Test 5. Compression Rotation Test 6. O'Brien's Active Compression Test 7. Resisted supination ER test |
|
|
What are special test for cubital tunnel syndrome? |
1. Pressure provocative test 2. Flexion Test 3. Tinel's sign |
|
|
What are special tests for MCL tears at the elbow? |
1. Valgus stress at 30, 60, 70, 90 deg of elbow flexion 2. Moving Valgus Stress Test |
|
|
What are special tests for lateral epicondylitis? |
1. Tennis Elbow Test 2. Mill's Test |
|
|
What are special tests for wrist and hand ligamentous instability? |
1. Thumb Ulnar Collateral Ligament Test 2. Test for Tight Retinacular Ligaments 3. Lunatetriquetral ballottement test
|
|
|
What are special tests for integrity of wrist and hand tendons and muscles? |
1. Finkelstein's Test 2. Sweater finger sign for rupture of the FDP tendon 3. Bunnel-Littler Test |
|
|
What are tests for neurological dysfunction in the wrist and/or hand? |
1. Tinel's sign 2. Phalen's test 3. Reverse Phalen's Test 4. Carpal Compression Test 5. Froment's Sign |
|
|
What are special tests for circulation in the wrist and hand? |
1. Allen's test 2. digit blood flow (nail bed compression) |
|
|
What are special tests of hip pathology? |
1. Patrick's (FABER) test 2. Flexion Adduction IR (FADIR) Impingement Test 3. Scour Test 4. Trendelenberg Sign |
|
|
What are Ligamentous test of the knee? |
1. Lachman's Test 2. Anterior Drawer Test 3. Pivot-Shift Test 4. Valgus Stress Test 5. Varus Stress TEst 6. Posterior Drawer |
|
|
What are tests for Meniscus in the knee? |
1. McMurray's Test 2. Apley Test 3. Thessaly Test 4. Bounce Home Test 5. Joint Line Tenderness |
|
|
What are tests for patellar instability? |
Patellar apprehension test |
|
|
What are tests for Patellofemoral syndrome? |
1. McConnell Test 2. Passive Patellar Tilt Test 3. Clarke's Sign (Patellar compression test) |
|
|
What are tests for IT band friction syndrome? |
Noble compression test |
|
|
What are tests for ligamentous instability at the ankle? |
1. anterior drawer test 2. Talar tilt 3. Squeeze test for syndesmosis injury |
|
|
What is the the test for Achilles rupture? |
Thompson's test |
|
|
What are the movement tests, postural analysis findings and example for an anterior innominate rotation - pelvic girdle dysfunction/ |
Direction of motion restriction = posterior rotation Movement test: Standing flexion test Long sitting test Posture Analysis: -Iliac Crest/PSIS high, ASIS low in standing -ASIS low in supine -supine length length longer -sitting length length shorter example: L anterior innominate (+) standing flexion and long sitting tests on the L L PSIS high, L ASIS low in standing L leg longer in supine L leg shorter in long sitting |
|
|
What are the movement tests, postural analysis findings and example for an posterior innominate rotation - pelvic girdle dysfunction/ |
Motion Restriction = Anterior rotation Movement Test: Standing flexion test Long sitting test Postural Analysis: ASIS higher, PSIS lower in standing Supine leg length shorter Long sitting leg length longer Example: Left Posterior Innominate (+) standing flexion and long sitting tests on L = L ASIS high, PSIS low in standing L leg shorter in supine L leg longer in long sitting |
|
|
What is innominate upslip definition? |
vertical shear of an entire innominate in which the ASIS and iliac crest are up in comparison to the opposite side innominate (ASIS and PSIS on one side will be higher than opposite side) |
|
|
What are the movement tests, postural analysis findings and example for an upslip of innominate - pelvic girdle dysfunction/ |
Movement Test: Standing Flexion Test Postural analysis: -ASIS and PSIS higher than contral side in standing supine and long sitting leg length shorter than other side Example: Left upslip innominate L PSIS and ASIS higher in standing L leg shorter in supine and long sitting |
|
|
What are the movement tests, postural analysis findings and example for a forward or backward sacral torsion - pelvic girdle dysfunction/ |
Movement Test: Sitting flexion test Postural Analysis: -Sacral sulcus (base of sacrum and ilium) deep (in prone) & sacral inferior lateral angle (near apex) (ILA) posterior and down (shallow) on opposite side example: forward or backward torsion Sitting flexion test (+) on Right Sacral sulcus deep on R and ILA posterior on L = L rotation of sacrum on R oblique axis (see notes and print out) |
|
|
How are sacral torsions named? |
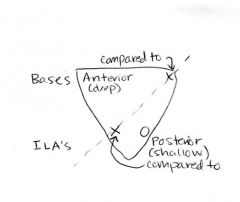
Sitting flexion test: the (+) side is the hypomobile side. Opposite side is considered axis (so if L side is (+) then axis is R -draw the upside down triangle put (+) for the ILA or sulcus that is palpated as more deep/anterior and negative for the opposite side that is more posterior/shallow -if the (+) is at the base/sulcus of sacrum then rotation is the same as the axis so, for example, it would be R rotation on R axis. -if the (-) is at the base/sulcus, then rot is opposite to axis so would (-) on L base would be L rot on R axis |
|
|
What is Yergason's special test? |
-test for biceps muscle pathology (tendonosis/tendonopathy)/integrity of transverse ligament which holds biceps tendon in the bicepital groove -sitting with shoulder in neutral and elbow flexed to 90 and stabilized against trunk with forearme pronated -examiner resists supination with ER -tendon of long head of biceps will pop out of groove if transverse humeral ligament is torn -tenderness/pain without dislocation indicates bicipital tendionpathy |
|
|
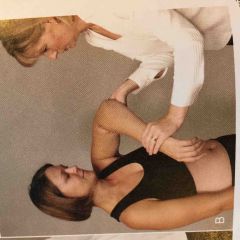
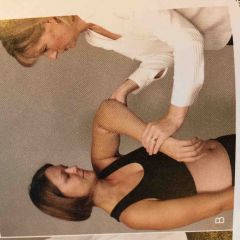
What is Speed's Test? |
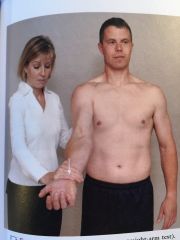
-identifies bicipital tendonosis/tendonopathy -sitting or standing -UE full ext and forearm supination resist shoulder flexion. Repeat with forearm in pronation -can also do with shoulder at 90 deg flexion and push into ext -->eccentric biceps contraction -do in supination and pronation (+) = increased tenderness in bicipital groove/long head of biceps tendon esp with supination position |
|
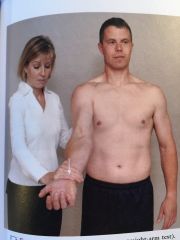
What test is this ? |
Speed's Test for biceps tendinopathy |
|
|
What is the Neer's Test? |

-to identify impingement of long head of biceps and supraspinatus tendon under the acromion -sitting -shoulder passively IR then fully abducted (+) reproduces pain in shoulder |
|
What test is this? |
Neer's test for impingement of Biceps tendon and supraspinatus |
|
|
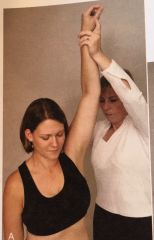
What is the Hawkins-Kennedy Test? |
-identify impingement of supraspinatus -standing -passive forward shoulder flexion to 90 deg -then forcibuly IR the shoulder (+) = pain indicating supraspinatus tendinosis/tendinopathy |
|
What test is this? |
Hawkins-Kennedy Test for shoulder impingement |
|
|
LE MM Innervations |

|
|
|
UE MM Innervations |

|