Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
26 Cards in this Set
- Front
- Back
|
Chronic Lymphoid Leukemia is a __-cell malignancy.
|
B-cell
|
|
|
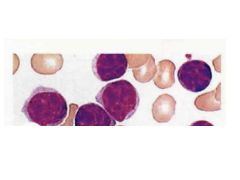
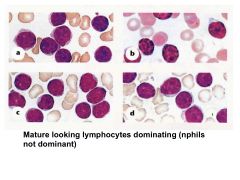
Characteristics of CLL cells.
|
Mature appearing, functionally incompetent lymphocytes in BM, blood, organs.
|
|
|
What is the most common form of leukemia in adults in western countries?
|
CLL
EXTREMELY RARE IN CHILDREN, median age 72 |
|
|
CLL:
Clinical Presentation |
>50% asyx
If do have syx, they're non-specific: fatigue, weight loss, anorexia |
|
|
What's a normal WBC?
WBC in CLL? |
Normal WBC: 5-10K
CLL WBC: 300K!! |
|
|
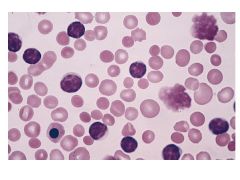
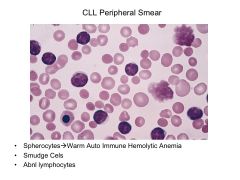
Hallmark of CLL.
|
Marked lymphocytosis (~300K in blood)
|
|
|
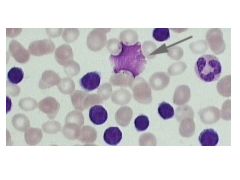
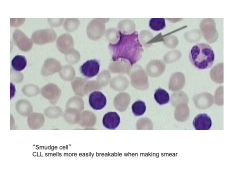
What is a smudge cell and what is it indicative of?
|
Smudge cell = cell that ruptured when performing peripheral smear.
Patients with CLL have more fragile cells and are more likely to have smudge cells on smears. |
|
|
CLL:
Chains expressed in flow cytometry CD Markers |
Express either kappa or lambda light chains
CD Markers: CD19+ CD23+ CD5+ *** (normally a T cell marker, but expressed in small subset of B cells) (some CD20+ too) High numbers = B Cell |
|
|
CD5+ is associated with ______.
|
CLL or Mantle Cell Lymphoma
|
|
|
What disease does CLL overlap with? Describe the overlap.
|
CLL: older pts w/tons of WBCs in blood/organs, LAD
SLL: same presentation but with more nodal distribution |
|
|
Does CLL result in LAD and hepatosplenomegaly?
Why or why not? |
Yes, with disease progression, small WBCs accumulate in BM, spleen, LNs, and liver; thus, resulting in generalized LAD and hepatosplenomegaly.
|
|
|
Clinical consequences of CLL:
Immune System Bone Marrow |
1) immune fn disrupted:
-hypogammaglobulinemia (inc'd risk infection-->death) -autoab's developed against RBC/platelets-->autoimmune hemolytic anemia or thrombocytopenia 2) BM replaced by malignant lymphocytes-->anemia & thrombocytopenia |
|
|
List findings associated with CLL that are associated with decreased median survival (in order of severity).
|
Lymphocytosis in blood and BM (12.5 years)
Lymphocytosis and LAD (8.4 years) Lymphocytosis + splenomeg/hepatomeg (5.9 years) Lymphocytosis and anemia (1.6 years) Lymphocytosis and thrombocytopenia (1.6 years) |
|
|
CLL has tendency to transform into ________. Provide 2 examples.
|
CLL has tendency to transform into more aggressive lymphoid neoplasms.
Ex: Prolymphocytic transformation (nastier than CLL) Richter's Syndrome (Diffuse Large Cell Lymphoma)--aggressive |
|
|
CLL:
Median Age of Survival Prognostic Factors |
Median survival >20 years; tx: WW
But 50% of early stage CLL pts exhibit rapidly progressive dz Prog Factors: Cytogenetics! Ex: 17p deletion (p53)--5 year survival |
|
|
Sequencing of Ig Heavy Chain Variable Region reveals what about CLL prognosis?
|
Mutated IgVH (cells have passed through germinal center)-->good prognosis (25 year median survival)
Unmutated IgVH: more aggressive form of CLL (9.75 years median survival) |
|
|
How is ZAP-70 useful in determining CLL prognosis?
|
ZAP-70 = key signal transduction molecule for molecules, but for some reason is expressed in CLL cells with UNmutated IgVH genes (poor prognosis).
Thus, people with LOW ZAP (LOW CD38) do really well (correlated with mutated IgVH). |
|
|
How is CD38 useful in determining CLL prognosis?
|
CLL = ZAP
Low CD38-->Low ZAP-->good prognosis High CD38-->High ZAP-->poor prognosis |
|
|
CLL:
Treatment |
Asyx: WW
Syx: Alkylating agents: -Chloambucil (oral single agent) -Cyclophosphamide -Benadmustine Steroids Nucleoside analogues: -Fludarabine (can use alone or with other agents) Monoclonal Abs: Rituximab (anti-CD20)--not very good by itself bc only small populn of CLL is CD20+ Mnemonic: use FCR (fludarabine, cyclophosphamide, rituximab)*** |
|
|
CLL vs CML:
Median Age Symptoms Defects Treatment |
CLL:
Median age 70s Largely Asyx Defect in mature B cell CML: Median age 50s Often syx w/fatigue, weight loss t(9,22) defect; pluripotential HSC Imatinib = tx |
|
|
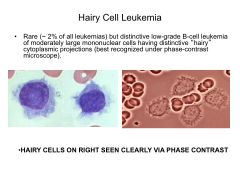
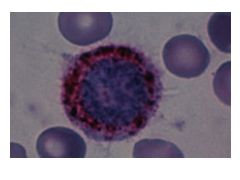
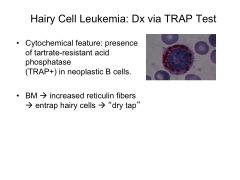
Hairy Cell Leukemia:
What category of leukemia is it?Typical clinical presentation Diagnostics Treatment |
Hairy Cell Leukemia = Rare, low-grade, chronic B cell leukemia
Classic presentation: Middle aged white man with pancytopenia, splenomegaly, no LAD. Diagnostics: TRAP test! If positive, treat with Cladribine--purine analogue (very responsive to this drug; normal age-matched life expectancy) |
|
|
|
|
|
|
|
|
|
|

|
|
|
|
|