Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
109 Cards in this Set
- Front
- Back
|
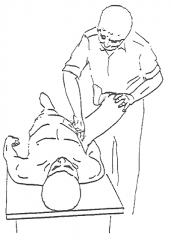
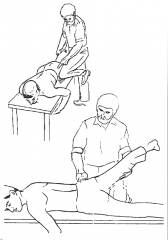
Ober Test
|
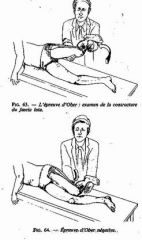
Indication: Tight ITB
Pt lies on side, with dysfunctional-side on top. Dr: Slight hip EXTENSION (allows ITB to pass behind greater trochanter), ABDUCT thigh, FLEX knee. Slowly release knee while supporting the ankle, allowing thigh to adduct. +: Thigh remains AB-Ducted (Polio, Meningomyelocele, Tight ITB) |
|
|
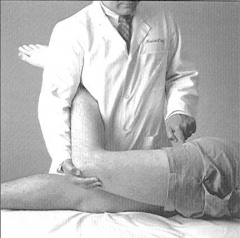
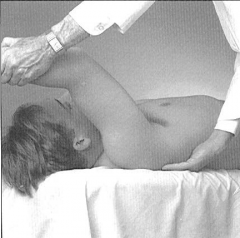
Thomas
|
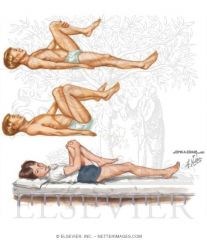
Indication: Tight Iliopsoas muscle (Tight hip flexor)
Pt supine, flattens lordotic curve by flexing both hips and knees. Pt then holds one knee, releasing one leg to table without allowing lordosis. Dr. examine distance knee is above table top, comparing bilaterally. +: Unable extend leg (Kidney stones, pancreatitis, iliopsoas contracture) |
|
|
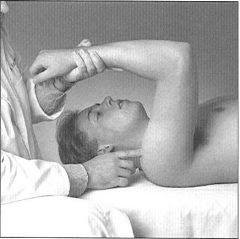
Patrick
|
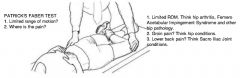
FAbErE Test: SI & Hip Dysfunction (motion restriction)
Pt Supine Dr FLEXES, ABDUCTS, EXTERNALLY ROTATES, EXTENDS leg. Dr gently presses knee toward table while stabilizing the contralateral ASIS, stressing ipsilateral SI joint. + (inguinal pain): hip pathology (arthritis) + (SI joint): SI joint pathology |
|
|
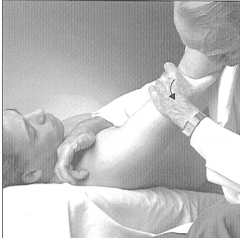
Hip Compression
|

Hip Scour: Hip joint arthritis or SI joint arthritis
Pt supine Dr flexes knee and hip (~Patrick), press against knee to add compressive force through femur, into hip joint. +(groin pain): Hip arthritis +(SI joint pain): SI joint pathology |
|
|
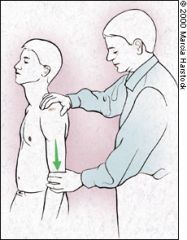
Trendelenburg
|
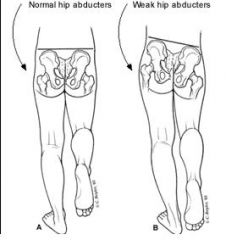
Indication: Gluteus Medius (hip abductors) weakness
Pt stands on one leg, then the other Normal: Hip abductors are normal on weight-bearing side, opposite hip should rise. +: Weak hip abductors cause opposite hip to drop (the non-weighbearing side). L5 radiculopathies, superior gluteal n. lesions, muscle atrophy. |
|
|
SCS Anterior Trochanter (AT)
|
Location: 1-2" caudad, slightly medial to ASIS, near tendinous origin of sartorius mm.
Pt supine Dr. on TP side F-Ab-Er (Can also tx piriformis) |
|
|
SCS PMT (Posteromedial Trochanter)
|
Posteromedial surface of femur; 4cm caudad to trochanter
Pt prone Dr. opposite TP E-Ad-Er Ishiogluteal bursitis |
|
|
SCS LT (Lateral Trochanter)
|
Lateral femur
Pt prone Dr. on TP side Ab-Er Trochanteric bursitis, ITB |
|
|
SCS PIR (Piriformis)
|

Belly of piriformis
Pt prone, LE off table Dr. on TP side F-Ab-Er |
|
|
SCS GM (Gluteus Medius)
|
3-4cm arc below iliac crest
Pt prone Dr. on TP side, knee supports pt leg E-Ab-Ir |
|
|
SCS PLT (Posterolateral Trochanter)
|
Posterolateral superior trochanter, near trochanteric bursa
Pt prone Dr. on TP side; Pt's thigh "slides down" across knee E-Ab-Er Trochanteric bursitis |
|
|
Which 2 SCS sites treat trochanteric bursitis?
|
PLT, LT
|
|
|
Drawer Test (Knee)
|
Indication: ACL/PCL tears
Pt. supine, knees flexed to 90, feet flat on table. Dr. sits on feet. Cup hands around patient's knee with fingers on area of insertion of medial and lateral hamstrings. Thumbs on medial and lateral joint lines. +Anterior: Tibia moves anteriorly (ACL) +Posterior: Tibia moves posteriorly (PCL) |
|
|
Lachman
|
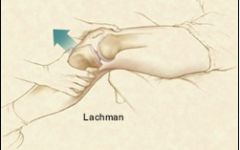
Indication: ACL integrity (best test b/c joint capsule is relaxed)
Pt supine, knee flexed 30 Dr. stabilizes femur with one hand, using other hand to draw proximal end of tibia anteriorly. +Lachman: "Mushy" or softened feeling when tibia moves anteriorly. |
|
|
Apley’s distraction/compression
|

Lateral & Medial Collateral Ligament tears: performed immediately AFTER Compression test. Pt prone. Dr. on TP side, stabilizing thigh with knee (if desired). Both hands grasp dorsal and posterior portions of patient's foot. Apply TRACTION on leg, while rotating tibia on femur. +Pain = ligament damage dependent on localization (Medial v. Lateral)
Lateral & Medial Meniscal tears: Pt prone, Dr. on TP side (same setup). COMPRESS menisci between tibia and femur, then rotate tibia on femur as you maintain firm compression. +Pain = Meniscal damage. |
|
|
Childress Squat Test
|
Indication: Meniscal injury associated with torn ACL (most sensitive test)
Pt squats and walks like a duck. +: Pain, unable to squat, may or may not be snap/click from joint. |
|
|
McMurray’s
|
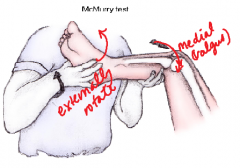
Indication: Meniscal tears & MCL
Pt supine Dr. holds patient's ankle. Flexes leg fully. Place other hand over knee with thumb and thenar eminence over lateral joint line. Contact medial joint line with remaining fingers. Apply a MEDIAL/VALGUS stress to knee with hand, while rotating leg externally with other hand. Slowly EXTEND knee. +: Palpable/Audible click = Torn Medial Meniscus (posteriorly) |
|
|
Joint effusion test
|
Pt supine, knee extended
Dr attempts to "milk" fluid from suprapatellar pouch and lateral side of knee into medial side of knee. When fluid has been forced to medial side, gently tap the medial side of the knee and palpate the lateral side for fullness. |
|
|
Patello-Femoral Grind
|
Indication: Quality of articulating surfaces of patella and trochlear groove of femur
Pt supine, legs relaxed. Dr stands opposite TP. Grasp superior border of patella, using thumb and index finger of cephalad hand. Grasp inferior border of patella with thumb and index finger of caudad hand. Push patella distally. Instruct pt to tighten quadriceps. Offer resistance to patella as it moves under fingers. + Pain or discomfort as patella moves. |
|
|
Patellar Apprehension
|

Indication: Patella is prone to lateral dislocation
Pt supine. Quadriceps relaxed. Dr. opposite TP. Press laterally against medial border of patella with thumb. Watch patient's face. If patient begins to dislocate, pt will look apprehensive or distressed. |
|
|
Myofascial release (indirect) of the knee
|

Indication: acute conditions.
Pt supine, leg relaxed. Place one hand on femur, above patella to stabilize knee, and one hand on tibia, below patella to motion test knee. Hold in DIRECTION OF EASE until release occurs. Re-evaluate! |
|
|
HVLA Anterior Fibular Head
|
Indication: Anterior Fibular Head
Pt supine, knee flexed Dr. on TP side. Place heel of cephalad hand over anterior aspect of fibular head, fingers project downward under knee joint. Grasp patient's dysfunctional leg with caudad hand, positioned superior to malleoli (thumb projects downward above lateral malleolus, fingers project down above medial malleolus) Mvt: Apply DOWNWARD pressure against fibular head with heel of cephalad hand in conjunction with INTERNAL ROTATION of tibia with caudad hand. This moves head of fibula POSTERIORLY on tibia. |
|
|
HVLA Posterior Fibular Head
|
Indication: Posterior fibular head
Pt supine. Dr. opposite TP. Place lateral portion of proximal end of cephalad index finger directly behind the head of the fibular head with thumb projecting over the anterior surface of the tibia. Grasp the patient's leg with your caudad hand, positioned superior to malleoli (thumb projects downward above lateral malleolus, fingers project downward above medial malleolus). Mvt: Apply FORWARD pressure against fibular head with index finger of cephalad hand in conjunction with further FLEXION and EXTERNAL ROTATION of tibia with caudad hand. This moves fibular head ANTERIORLY on tibia. |
|
|
Anterior Drawer Test (Foot/Ankle)
|

Indication: Anterior Talofibular (ATF) Ligament
+: Pain, swelling, echymosis = ATF Tear |
|
|
Squeeze test
|

Indication: High Ankle Sprain; tests ATF ligament/Tibiofibular syndesmosis injury
|
|
|
Thompson test
|

Indication: Achilles Tendon Tear/Rupture
Compress gastrocnemius |
|
|
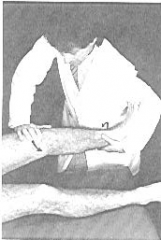
Talotibial Joint ME & HVLA – plantarflexed talus
|

Dorsiflexion of the talus = Restriction
Pt sits on edge of table, feet dangling. ME - Dr. sits in front of dysfunctional talus. Place medial hand under plantar surface of forefoot with web of lateral hand overlying neck of talus. DORSIFLEXION BARRIER engaged through dorsiflexion movement + posterior force on talar neck. Patient performs plantar flexion muscle effort against equal and opposite resistance 3-5s, 3-5reps. After each patient effort, additional dorsiflexion is introduced against barrier. HVLA-Pt supine with Dr at foot of table. Dr.'s hands encircle patient's foot with middle fingers overlapping superior aspect of the TALAR neck and thumbs on sole of the foot. Dr. engages dorsiflexion barrier and LONG-AXIS TRACTION. Mobilization with IMPULSE THURST (LONG-AXIS EXTENSION). RETEST. |
|
|
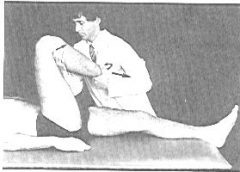
Subtalar Joint HVLA – posterolateral or anteromedial Talus
|
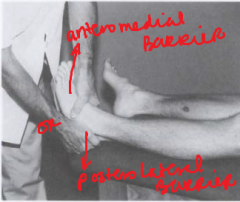
Indication: Posterolateral/Anteromedial Glide of Talus Restricted
Pt supine. Dr. grasps calcaneus, takes calcaneus into barrier. Traction of calcaneus is applied to take up slack. TRACTION TUG through barrier applied at subtalar joint. |
|
|
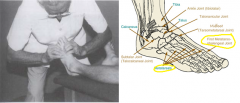
Navicular/Cuboid J-stroke (Hiss Whip) HVLA
|

Pt prone. Dysfunctional leg off side of table.
Dr. grasps pt's foot with both hands and places thumb in a "V" shape over the plantar surface of the navicular (medial) or cuboid (lateral, 5th MT) -- whichever is dropped. Dr exerts DOWNWARD THRUST through thumbs, while inducing a WHIP-LIKE MOTION at pt's ankle and knee. |
|
|
Metatarsal Head Joint Articulation
|
Dx: Restriction of joint play at metatarsal heads
Pt supine Dr's medial hand grasps shaft of 2nd metatarsal, while lateral hand grasps shaft of 3rd metatarsal. While stabilizing second metatarsal, Dr.'s lateral hand dorsal and plantar moves the metatarsal head seeking resistance to motion, and provides JOINT PLAY ROTARY MOVEMENT if restricted. |
|
|
Metatarsophalangeal/Interphalangeal Joints Articulation
|

Dx: Restriction at MTP/Interphalangeal joints
Pt supine. Dr. stabilizes proximal bone with thumb and fingers (first metatarsal). Dr. grasps distal bone (proximal phalanx of first toe). Flex-Extend, Anterior-Posterior Glide, Medial-Lateral Rotation, Medial-Lateral Tilt, testing for restriction. Sequential joint play motions performed to restore all joint play movements. All other interphalangeal joints can be treated in similar fashion by stabilizing the proximal bone and moving the distal upon it. Can give a traction tug as an articulatory technique at end. |
|
|
SCS MAN (Medial Ankle)
|
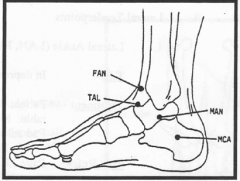
Tibialis Anterior
Inferior to MEDIAL MALLEOLUS, 1" arc, or in tibialis anterior muscle Pt lies on side, opposite dysfunction, with foot off table. Place rolled up towel beneath distal tibia. INVERSION with force from lateral ankle. Fine tune with slight INTERNAL ROTATION. |
|
|
SCS MCA (Medial Calcaneus)
|
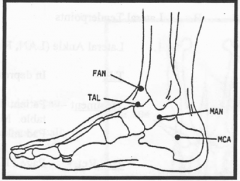
Abductor Hallucis
1" postero-inferior to MEDIAL MALLEOLUS, MEDIAL CALCANEUS. Pt lies on side, opposite dysfunction, with foot off table. Apply MEDIAL PRESSURE at heel to INVERT CALCANEUS. EVERT distal foot. |
|
|
SCS LAN (Lateral Ankle)
|
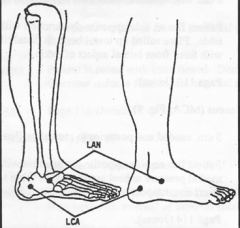
Peroneus Longus & Brevis
Anteroinferior to LATERAL MALLEOLUS. Pt prone on TP side with ankle off table. Lateral malleolus rests on rolled towel. EVERT from medial foot. Up to 50# of force. Fine tune with external rotation. |
|
|
SCS LCA (Lateral Calcaneus)
|
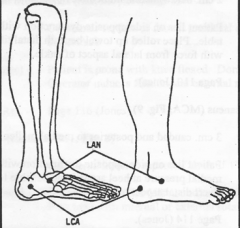
1" Postero-inferior to LATERAL MALLEOLUS
Pt on side of dysfunction with ankle off table. Lateral malleolus rests on rolled towel. EVERT at HEEL and COUNTER-ROTATE DISTAL FOOT. |
|
|
SCS NAV (Navicular)
|
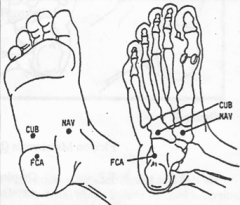
Tibialis posterior
Plantar foot of navicular bone (medial). Pt prone with knee flexed. Medially rotate foot into INVERSION (internally rotate). Support your second finger with your third finger, and use pressure from other hand to accomplish this. |
|
|
SCS CUB (cuboid)
|
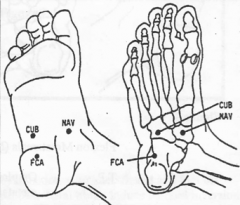
Extensor Digitorum Brevis
Dorsum of the foot over the cuboid bone. Pt prone with knee flexed. Dr. grasps lateral side of metatarsals and presses DOWNWARD on the plantar surface overlying the 5th metatarsal. Exerts pressure toward the knee, creating DORSIFLEXION of the foot. This induces EVERSION and some extension of the cuboid in relation to rest of foot and shortens the extensor digitorum brevis |
|
|
SCS FCA (Flexion Calcaneus)
|
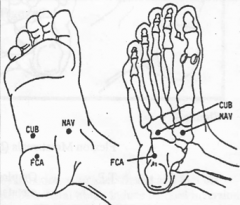
Quadratus Plantae
Plantar foot on anterior calcaneus, in PLANTAR FASCIA. Pt is Prone Flex knee, grasp calcaneus and FLEX (COMPRESS); force dorsum against thigh, wrap around point. |
|
|
Jobe’s
|

Indication: Supraspinatus tendinitis
Pt standing, abducts arms to 90 degrees at the shoulder with elbows extended. Then the shoulder is maximally internally rotated and forward flexed to 30 degrees (empty beer can maneuver). Dr. places DOWNWARD force on patient's arms and patient resists this motion. +: pain AND/OR weakness |
|
|
Drop Arm
|
Indication: Rotator cuff tear (Supraspinatus)
Pt's arm is passively ABDUCTED to 90 degrees. Pt is asked to SLOWLY LOWER arm to side. +: Arm drops quickly. |
|
|
Scapular Winging
|
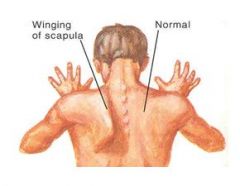
Indication: Weakness of serratus anterior muscle or dysfunction of long thoracic nerve (C5-7)
|
|
|
Apprehension
|

Indication: Anterior shoulder dislocation
Pt supine ABduct, Externally Rotate patient's arm. If shoulder is unstable, pt will have a look of apprehension/alarm. A posteriorly directed force on the anterior aspect of the shoulder will stabilize the joint, decrease pain and apprehension. |
|
|
Speed’s
|
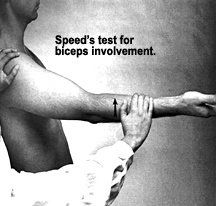
Indication: Biceps tendinitis
Pt seated/standing. Dr asks pt to slightly flex his shoulders, extend elbows, fully SUPINATE forearms. Pt is then asked to RAISE ARMS upward as Dr resists motion with DOWNWARD force. +: Pain along course of long head of biceps with weakness |
|
|
Crossover
|
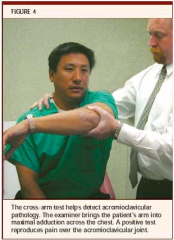
Indication: AC Joint pathology
ADDUCT patient's arm across chest to touch opposite shoulder. +: Pain over AC joint |
|
|
Impingement tests: Hawkin's & Neer's
|
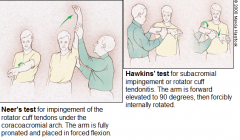
Impingement = Symptom, often of subacromial bursitis or supraspinatus tendinitis or a tear.
Impingement (Humeral head into acromion): ABduct arm 180. (+: cannot abduct past 90) Hawkin's: Flex and internally rotate shoulder, while placing downward pressure on patient's wrist. Neer's: Flex with internal rotation |
|
|
Sulcus test
|
Indication: Glenohumeral instability, possible AC joint separation
Pt seated/standing, shoulder neutral. Dr. grasps arm proximal to elbow, looking for dimpling of the skin below the acromion. Palpation reveals widening of the subacromial space between the acromion and the humeral head. |
|
|
SCS Subdeltoid
|
Under the acromion high on anterolateral humerus
"Statue of Liberty": ABDUCT arm 90°, forward FLEXION (horizontal plane) 30°. Internal/External arm rotation to fine tune Indication: Shoulder bursitis |
|
|
SCS Coracoid
|

Coracoid process of the scapula.
ADDUCT arm across chest so that hand is touching opposite shoulder; fold in the wrist. Indication: Tendinitis/Strains of biceps |
|
|
SCS Long Head Biceps
|

Bicipital groove
“Woe is me” position: Abduct arm with wrist resting over the patient’s forehead to about 160°. Indication: Biceps tendonitis/Strains |
|
|
SCS Infraspinatus
|
1-2” below spine of scapula (T3) and ½” lateral to medial margin of scapula
160-180° of flexion of arm or 180 abduction |
|
|
SCS Supraspinatus
|
Supraspinatus fossa
Pt supine; 45° of flex/abduct/external rotation arm. (45-45-45: F-Ab-Er). If this does not relieve the TP, try 180° of abduction. |
|
|
SCS Trapezius
|

Middle of upper trapezius behind the first rib pressing anteriorly.
Pt supine. Sidebend Pt’s head TOWARD t.p. side. Rotate AWAY. ABDUCT shoulder to approximately 180°. |
|
|
SCS Subscapularis
|

Anterior surface of scapula in the posterior axillary fold.
Pt supine. Extension 30°, Abduction 30°, Internal rotation of shoulder (E-Ab-Ir) |
|
|
SCS Pectoralis Minor
|

3cm inferior and medial to coracoid (anterior AC joint) Patient supine.
ADDUCT Pt’s arm obliquely across the body and add CAUDAL TRACTION. |
|
|
SCS Levator Scapula
|

At the superior medial angle of the scapula Patient prone.
Pt’s head turned away from t.p. Extend and internally rotate shoulder by grasping patient’s wrist. Add caudal traction. Alternate: Patient supine and neck sidebent to the side of the t.p. With the elbow flexed, apply a cephalad force through the shaft of the humerus to elevate the scapula. |
|
|
Scapular Release MFR
|

Pt lies on side with affected side up. Patient's hips and knees are flexed (for stability) and a pillow is placed under his head for comfort.
Dr. stands along side the table facing the patient. Drape patient’s arm over your caudad forearm. Introduce the fingertips of both hands under the medial border of the scapula. Control the scapula with both hands and gently assess its full range of motion. Keep in mind the muscular restrictions that would cause a loss of motion. Restrictions in motion can be relieved by:Holding against a barrier with traction.\ (Direct Myofascial Release). Holding in a position of ease. (Indirect Myofascial Release) Follow the unwind. Range of motion / stretching or vibrating against the barrier. (Articulatory Technique) Reassess the S-T motion and treat remaining restrictions |
|
|
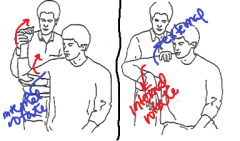
Spencer Technique (all stages)
|
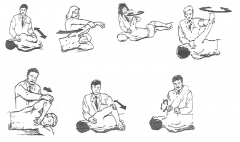
The Spencer Technique can be used for evaluation of passive range of motion and then for subsequent treatment (useful for adhesive capsulitis ie. frozen shoulder, restricted ROM from fibrosis). The patient is lying on side with the involved shoulder up. Physician is facing patient stabilizing clavicle and scapula.
1. GH joint EXTENDED, Elbow FLEXED "Hi" 2. GH joint FLEXED, Elbow EXTENDED. "Ice cream" 3. Shoulder ABDUCTION cw/ccw CIRCUMDUCTION, slight COMPRESSION downward through elbow. "Little cone." 4. Shoulder ABDUCTION cw/ccw CIRCUMDUCTION w/ gentle TRACTION. "I'll have the BIG cone 5. Shoulder ABDUCTION, Elbow FLEXED. GH joint ABDUCTION ("big cone is mine." 6. Shoulder ABDUCTION, Elbow FLEXED, Hand behind back. "Fight for it." 7. Elbow EXTENDED, wrist supported on physician's shoulder. Dr grasps deltoid area just distal to GH joints. "Let's be friends" |
|
|
ME AC/ GH joint (internal/external rotation)
|
External rotation: 1. Externally rotate the shoulder of the affected side to the barrier by grasping the elbow and the distal arm with one hand (to stabilize shoulder) and grasping the raised wrist and distal forearm with the other hand.
2. Have the patient internally rotate the humerus against your unyielding counterforce 3-5 times (for 3-5 seconds) using muscle energy principles. 3. Adding 30° of forward flexion of the arm will isolate treatment to the AC joint. 4. Alternative: Support the patient’s forearm by grasping the patient’s wrist with your right hand and placing your forearm in front of the patient’s forearm. Use the left hand to support the shoulder. INTERNAL ROTATION: 1. Internally rotate the shoulder of the affected side to barrier by grasping the acromioclavicular area with one hand (to stabilize the shoulder) and reaching under the arm and grasping the dorsum of the wrist with the other hand. 2. Have the patient externally rotate the humerus against your unyielding counterforce 3-5 times (for 3-5 seconds), using muscle energy principles. 3. Adding 30° of forward flexion of the arm will isolate treatment to the AC joint. |
|
|
Posterior Capsule ME Stretch (Greenman)
|
A. Hypertonic: (Treat these muscles using counterstrain or muscle energy).
- Levator scapula - Latissimus dorsi B. Inhibited: (Treat using ME/HVLA) - Serratus anterior (from alternating stacked ERS’s in mid scapular area) - Middle & Lower Trapezius (from FRS’s in lower T-spine). Useful for frozen shoulder. 2. Patient in lateral recumbent position with involved should down. 3. Physician flexes the elbow and abducts the shoulder to 90 degrees. 4. Physician internally rotates arm to barrier by pushing down on wrist. 5. Holding the arm at the barrier, roll the patient’s body forward and then backward repeatedly. |
|
|
SCS - ME (medial epicondyle / pronator)
|
Medial epicondyle Pt supine
Flex, Pronate, Abduct F-Pro-AB |
|
|
SCS - LE (lateral epicondyle / radial head)
|
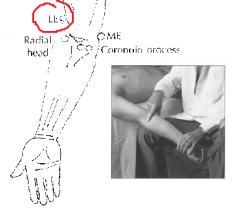
Between radial head and lateral epicondyle? Pt supine
Extend, Supinate, Abduct E-Sup-AB |
|
|
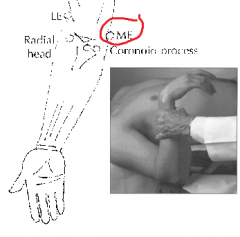
SCS - Biceps/coronoid
|
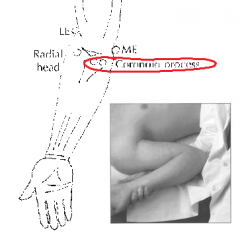
Coronoid process Pt supine
Pull forearm out to side a bit, with palm facing forward, then marked flexion F-Ab |
|
|
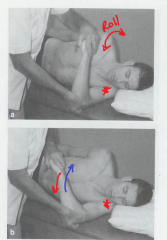
ME: Pronation/supination
|
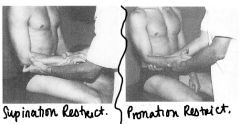
RESTRICTED SUPINATION (likes to pronate = posterior radial head): Dr's lateral hand stabilizes flexed elbow and monitors radial head, while medial hand SUPINATES the forearm to the barrier. Pt performs 3-5 muscle contractions in the pronation direction for 3-5 seconds each against resistance offered by the physician’s medial hand. Dr. engages a new SUPINATION BARRIER after each patient effort.
RESTRICTED PRONATION (likes to supinate = anterior radial head): Dr's hands in the same location but engaging the PRONATION BARRIER, as Pt contracts muscles in the supination direction. Dr engages a new PRONATION barrier after each patient effort. |
|
|
HVLA Anterior Radial Head
|

Anterior radial head (Pronation restriction): Dr PRONATES, FLEXES patient’s forearm while thumb holds the radial head POSTERIORLY (in a dorsal position) to engage barrier. Then an increasing elbow FLEXION THRUST is performed.
|
|
|
HVLA Posterior Radial Head
|
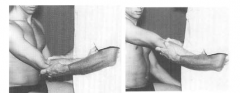
Posterior Radial Head (Supination Restriction, most common): Dr grasps proximal forearm with index finger of lateral hand overlying posterior (dorsal) aspect of radial head. Then Dr engages barrier: EXTENSION, SUPINATION, ADDUCTION. Thrust in a LATERAL-ANTERIOR(volar) direction.
|
|
|
MFR: compression of intraosseous membrane
|

1. Direct & Indirect MFR-between and across joints of arm/forearm (rope burn)
2. Dynamic Functional-seek ease, avoid bind-compress or distract whichever eases more-follow till it stops at a new balance point. 3. Facilitated Positional Release(FPR)-a modified indirect MFR enhanced by placing the region in neutral position and adding compression or torsion to cause neuro-reflexive RELEASE at the GAMMA SPINDLE LOOP, lengthening the short hypertonic muscles maintaining joint somatic dysfunction. |
|
|
Articulatory “joint play”: Wrist joints (Distal Radioulnar Joint, Ulna-Meniscal-Triquetral Joint)
|
Distal Radioulnar Joint: Dr stabilizes patient’s hand and radial-carpal region by reaching index finger through web of patient’s thumb and wrapping rest of hand around distal radius and proximal carpals (fig 1). With other hand grasp distal ulna between thumb & finger pads. The doctor grasps the distal ulna between the thumb and pads of the fingers (fig 2). Now the doctor does a “HOLD ONE, MOVE ONE” using A-P glide and medial and lateral joint play motion of the DISTAL ULNA.
Ulna-Meniscal-Triquetral Joint: Using same hand hold as above, place thumb over the dorsum of the distal ulna and the PIP of the index finger over the volar aspect of the pisiform (fig 3). Now the doctor squeezes index and thumb together to increase joint play. Repeat the squeeze-release process through the doctor’s right hand to aid in dysfunction at the ulna-meniscal-triquetral articulation region. Retest and compare to the unaffected side. |
|
|
Tinel
|
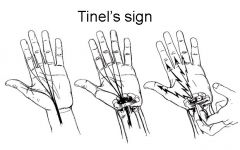
With your index finger, strike the median nerve where it passes through the carpal tunnel, under the flexor retinaculum and volar carpal ligaments.
+: Tingling sensation radiating from wrist to hand, along median nerve distribution, +CTS |
|
|
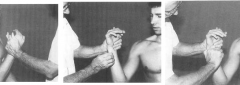
Phalen
|
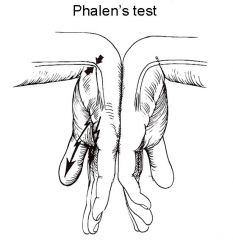
CTS symptoms are reproduced by having the patient hold his wrists in maximum flexion for upwards of 1MINUTE.
|
|
|
Reverse Phalen
|
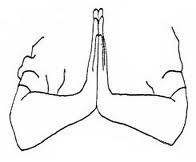
CTS symptoms reproduced by having the patient hold their wrists in maximum extension (praying hands). This test could be helpful in determining the degree of CTS.
|
|
|
Compression Test
|
Most sensitive test for CTS.
Dr. supports Pt's SUPINATED WRIST with one hand and presses firmly with the opposite thumb/finger over the space between the flexor carpi radialis and palmaris longus tendons at the distal flexion crease. (where the MEDIAN N. enters carpal tunnel) Hold for 1 MINUTE or more. +: Numb/Tingle in median N. distribution. |
|
|
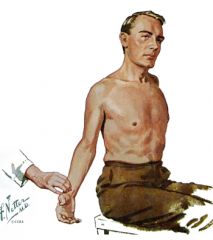
Allen
|

Assess vascular competence PRIOR to ARTERIAL BLOOD GAS.
Have patient open and close fist several times and then squeeze fist tightly. The physician then occludes both the radial and ulnar arterial pulses with digital pressure applied to the wrist. Have patient open their hand. The palm should be PALE. The physician then releases one artery and observes the return of the vascular blush. If the hand remains pale or flushes very slowly, the artery is partially or completely occluded. Repeat the maneuver with the other artery. |
|
|
SCS PWR (Palmar Wrist Retinaculum)
|
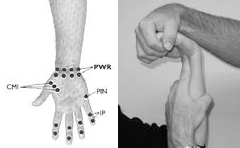
Palmar surface of the carpals
PALMAR FLEX wrist over tender point. Fine tune with pronation or supination and radial/ulnar deviation. |
|
|
SCS CM1 (First Carpometacarpal)
|
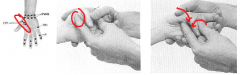
Thenar eminence of the palmar surface of the first metacarpal Flex or oppose thumb over tender point. Fine tune with abduction/adduction, internal/external rotation
|
|
|
SCS PIN (Interosseous Joints)
|
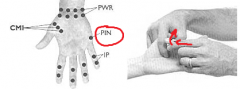
Palm of hand, medial and lateral sides of shafts of metacarpals Flex fingers over tender points. Fine tune with lateral flexion toward tender point and rotation.
|
|
|
Flexor Retinaculum Stretch (AT Still Tx)
|

Purpose: Stretch flexor tendons of the wrist, stretch the Flexor Retinaculum, causing a decreased pressure on the contents of the carpal tunnel.
Dr interlaces fingers of both hands and encircles the patient’s wrist. Dr's thenar eminence should contact the patient’s wrist over the Flexor Retinaculum.As firm compression is provided by the physician, the patient actively opens and closes hand 5-10 times. |
|
|
Opponen’s Roll (Sucher Technique)
|

Purpose: Stretch muscles and ligamentous attachments of wrist, which releases pressure on the Median nerve.
Pt's hand is held palmar side up. Grasp Pt's hand by placing your thumbs over the hypothenar and thenar eminences. Simultaneously, abduct, extend and laterally rotate (supinate) the thumb, while adducting, extending and internally rotating (pronate) the fifth digit along the axis of the first metacarpal bone. Begin gently and increase pressure to patient’s tolerance. |
|
|
Wrist ME: Adduction, Abduction, Flexion, Extension
|
As in muscle energy techniques for treating dysfunctions of other joints, the wrist is moved into the barrier of motion and the patient is asked to push isometrically back toward the freedom of motion. The technique described below is used for wrist restriction in the direction of ulnar deviation (adduction).Technique:The joint is moved into ulnar deviation to the barrier to motion.The patient is asked to push toward the radial aspect as the physician provides resistance.This position is held for approx. 4 seconds, then released.The joint is moved to its new barrier.The maneuver is repeated 3-4 times
|
|
|
Wrist HVLA– radiocarpal / carpal dysfunctions
|

Dr grasps the patient’s hand on the side of the dysfunction and localizes the DORSAL RADIOCARPAL JOINT with thumbs.
Dr exerts a WHIP-LIKE THRUST on the hand, moving it into rapid HYPEREXTENSION while exerting a DOWNWARD counterforce through the carpal bone somatic dysfunction. Contraindicated if the patient has significant pain with normal range of motion. Always use with caution. |
|
|
Adson’s
|

Arm is EXTENDED POSTERIORLY with head turned away from the affected side while monitoring the RADIAL pulse. Then monitor with the head turned toward the affected side.
+: Diminished radial pulse or reproduction of neurologic symptom indicates HYPERTONIC ANTERIOR/MIDDLE SCALENES, nerve root IMPINGEMENT PROXIMAL to BRACHIAL PLEXUS |
|
|
Hyperabduction
|
Arm is extended behind and raised up to 90 degrees.
+: Diminished radial pulse or reproduction of neurologic symptom; HYPERTONIC PEC-MINOR and HUMERAL ATTACHMENT. |
|
|
Axial Compression
|
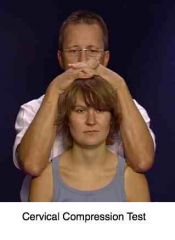
Assess spinal nerve impingement at spine level.
+Induces pain or numbness in nerve distribution at spinal level of the pathology. Degenerative disk (young patients) or spinal stenosis (older patients). |
|
|
Jackson
|
Nerve Root Impingement
Pure Sidebending of cervical spine TO affected side, then apply AXIAL COMPRESSION. Repeat to the unaffected side to compare. |
|
|
Spurling
|

Extend, Rotate neck toward affected side + Axial load.
This decreases dimensions of foramen through which nerve root exits spine. Older pts: Foraminal stenosis Younger pts: Intervertebral disk prolapse |
|
|
SCS P1R (Posterior Rib 1)
|
Elevated rib 1, tender on superior surface close to attachment to spine at base of neck Pt seated, t.p. side arm over Dr.’s knee
Dr. moves knee laterally, causing elevation of 1st rib. Dr. SIDEBENDS cervical spine TOWARD SD. Fine tune: rotate away/toward with extension/flexion – whichever gives maximal softening. |
|
|
SCS A1R (Anterior Rib 1)
|

Lateral to sternum, below sternoclavicular joint Pt seated, arm draped over Dr.’s knee, OPPOSITE t.p.
Dr. standing behind patient. Pt’s head is slightly flexed, rotated and side-bent toward the tenderpoint. F-Rt-St |
|
|
SCS A2R
|

MIdclavicular line, level of the second rib interspace Slightly more flexion is required for the second rib than for the first. (See above)
↑F-Rt-St |
|
|
ME Rib 1-2 exhaled
|

EXHALED RIB 1: Pt supine. Dr may stand on either side of the patient. Dr grasps the key rib (top rib) posteriorly at the rib angle.
Rib 1: Forearm flexed on patient’s forehead Rib 2: Pt's head is rotated AWAY from rib. Pt INHALES as Dr puts ANTERIOR, CAUDAL traction to key rib (top rib) posteriorly: Pt holds breath 2-3 seconds. Rib 1: Patient raises head straight up toward the ceiling. Rib 2:Patient turns head away from dysfunctional side 30°, then lifts head toward the ceiling. Engage the barrier by repositioning the arm, usually with more abduction.Repeat isometric contractions 3-5 times. |
|
|
ME Superior Clavicular Head
|

atient Position: supine.2.Physician position: standing at the side of the table, next to the affected shoulder.3.Technique: The physician places one hand on the superior aspect of the proximal clavicularhead. With the other hand the physician grasps the patient’s wrist and holds the arm extended and internally rotated. The patient is instructed to flex shoulder against the physician’s hand 3-5 seconds. The barrier is engaged after each isometric contraction by extending the arm slightly further each time (+/-increasing internal rotation to fine tune). The technique is repeated twice more. This engages the clavicle head of the Pect. Maj. (a 2ndary shoulder flexor).4.Re-assessTx
|
|
|
ME Anterior Clavicular Head
|

HeadPatient position: supine, with their ipsilateral hand on the doctor’s shoulder.Physician position: standing at the side of the table, next to the affected shoulder.Technique: The physician places one hand on the anterior aspect of the proximal clavicular head on the restricted side and with the other reaches behind the axilla to cover the scapula. The patient holds the physician’s shoulder with the hand of the affected side. The physician flexes the clavicle toward the manubrium until movement is palpated in the sternoclavicular joint.To accomplish this, the physician straightens his/her body and pulls the scapula anteriorly. The patient is instructed to pull down on the physician’s shoulder, hold for 2 to 3 seconds, and then relax. The maneuver is repeated twice more.Re-assess.
|
|
|
Chin Pivot HVLA
|

FLEXED T1-T4 dysfunctions ONLY
Pt position: PRone Procedure: Stand at head of table. Place pt's chin on table, pillow under chest. SIDEBEND AWAY, to level of dysfunctional joint space. ROTATE TOWARD. Place hand (opposite of dysfunction) on side of patient's head. Place pisiform region, hypothenar eminence (same side of dysfunction) over transverse process. Have Pt breathe in and exhale several times as you take up the tissue slack, localizing your forces. Use a HVLA thrust through PISIFORM in a lateral, posteroanterior (toward floor) and caudad direction. This side-bends the patient in a direction opposite the dysfunctional side-bending. Use the hand on the head to stabilize it as your force is transmitted. The posteroanterior force on the left transverse process of T1 induces right rotation while the stabilizing hand on the head effects a slight relative rotation in an opposite direction.RETEST the range of motion. VERY IMPORTANT: 99% of the force is directed to the transverse process with one hand and approx. 1% is used to stabilize the head with the other hand. If 50/50 force is used, or any other increased force on the head –heads will roll! (i.e. It would be very painful!) |
|
|
Upper Quarter (Greenman): cervical flexion test
|

Inhibited: Longus colli, deep neck flexors
Hypertonic: SCM & Scalenes Pt supine Instruct Pt to “Look down at your feet.” Observe for lifting head instead of tucking chin & rolling due to inappropriate muscle substitution. |
|
|
Upper Quarter (Greenman): bilateral shoulder abduction maneuver test
|

Inhibited: Serratus anterior, Mid/Lower Trapezius, Rhomboids, Supraspinatus
Hypertonic: Upper trapezius, Levator scapulae Assess for asymmetry of gliding motion of scapula on trunk. Inferior scapula go laterally. Scapular winging. |
|
|
Upper Quarter (Greenman): scapular stabilization test
|
Assess for winging of scapula during a wall push-up
Inhibited: Serratus anterior, Lower trapezius, Rhomboids |
|
|
Upper Quarter (Greenman): scapular depression test
|

Inhibited lower trapezius
Hypertonic levator scapulae & upper trapezius Instruct Pt to “Pull shoulder blade down and back” Note: hand position isolates Lower Trap motion. Monitor contraction of the lower Trapezius. |
|
|
Upper Quarter (Greenman): bilateral shoulder flexion test
|

Pt supine knees bent
Operator introduces bilateral upper extremity flexion. Observe for asymmetric arm elevation (as shown). Indication of hypertonic Latissimus dorsi on side of restricted flexion |
|
|
Upper Quarter (Greenman): anterior shoulder position test
|

TestHypertonic: Posterior Shoulder CapsuleLevator scapulaeUpper Trapezius Inhibited: Middle/Lower Trapezius Serratus anterior RhomboidsSubstitutes: Pectoralis minorResult: Shoulder Impingement Syndrome-impinges on Rotator cuff, esp. Supraspinatus tendon
TestWith Pt supine, assess position and symmetry of shoulder girdleAsk: Which shoulder is moreanterior?Dysfunctional PatternIncreased anterior shoulder positionTight Posterior shoulder capsuleTight Pectoralis minor |
|
|
Self-Stretch Levator Scapula
|

FSaRa, Lean away
Only major long cervical restrictor to SB/Rotate to SAME SIDE. |
|
|
Self-Stretch Upper Trapezius/SCM
|

FSaRt, tuck chin, lean away
|
|
|
Self-Stretch Scalenes
|

Grasp trapezius (stabilize Rib 1-2)
SaRa/t, Tuck chin. Hold 3-5 sec, repositioning 3-5x. |
|
|
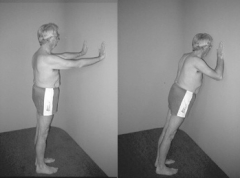
Self-Stretch Pectoralis Major/Minor
|

Feet parallel to wall. Front arm stabilizes. Stretch shoulder of the back arm-3 ways: Middle fibers, Lower fibers, Upper fibers. Lead stretch with shoulder, not hip. Stretch with exhalation
|
|
|
Self-Stretch Posterior Capsule Stretch
|

Lay dysfunction side down.
With elbow at 90°, upper arm on table, push wrist towards floor until tightness is felt, “roll on, roll off, drop arm further”(roll on/off shoulder & drop arm to the table) |
|
|
Self-Stretch Latissimus Dorsi
|

Elbows Together. Hold 12 o’clock (Post Pelvic Tilt). Sit back to Heels. Drop Chest to the Floor. Elongate Trunk. Do at start & end of routine
|
|
|
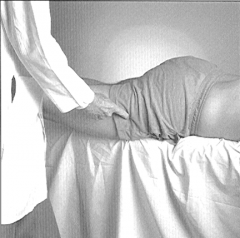
Hip/Pelvis ME: Adduction Dysfunction, Abduction Dysfunction
|

Pt supine.
Dr. takes pt into barrier. |
|
|
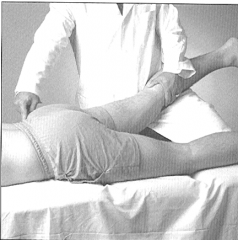
Hip/Pelvis ME: Extension Dysfunction, Flexion Dysfunction
|

Hamstring Restriction (Restricted in Hip Flexion)
Iliopsoas Restriction (Restricted in Hip Extension) |
|
|
Hip/Pelvis ME: Internally Rotated Hip Dysfunction, Externally Hip Dysfunction,
|

Gluteus medius/minimus Restriction
Piriformis Restriction |
|
|
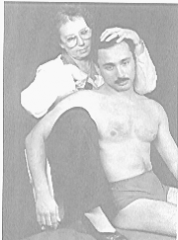
Costoclavicular Maneuver
|
Tests for vascular compromise of SUBCLAVIAN A. as palpated at radial a.
EXTEND head with shoulders RETRACTED +: Diminished RADIAL pulse or reproduction of neurologic symptoms–Indicates INHALED RIB1 or INFERIOR CLAVICLE, Nerve root impingement DISTAL to BRACHIAL PLEXUS |
|
|
ME: Rib 1, Rib 2 (Inhaled)
|

Pt supine, Dr at head of table.
FLEX & SIDEBEND to involved rib: Forces localized to key rib (lowest rib) by placing CAUDAL pressure on rib anteriorly. Patient holds breath out at end of expiratory phase 2 –3 seconds. During this time physician adjusts flexion/sidebending to new restrictive barrier. The physician may follow rib down while patient holds end expiratory phase 2-3 seconds. The patient performs isometrics by EXTEND HEAD against your counterforce, if necessary (last breath only). Engage the new barrier. Repeat 3-5 times Note:Remember-1strib is in supraclavicular fossa and 2ndrib just below the clavicle. |
|
|
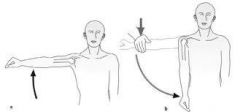
Unilateral Shoulder Abduction Maneuver
|
Ideal: Supraspinatus, Deltoid, Infraspinatus, Mid/Low Trapezius, Contralateral Quadratus Lumborum
Dysfunctional: Levator scapula, late middle/lower trapezius, Ipsilateral quadratus lumborum |