![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
63 Cards in this Set
- Front
- Back
|
Functions of digestive system (6) |
Ingestion, movement of food, Digestion, Absorption (main), Defecation, Other (pleasure, barrier integrity, medicinal) |
|
|
Function of the mouth in digestion |
Chewing through the use of pattern generators mechanically breaks up food. It helps mix food with saliva (lipase and amylase) to start the digestion process. When ready the body initiates a swallowing action to push the food bolus into the oesophagus. |
|
|
Function of the stomach in digestion |
A container for food, acts as a grinder for the food, initialises proteolysis and continues lipolysis. This mix is then under regulation emptied into the SI depending on the neural and hormonal feedback from the SI. |
|
|
Function of the SI |
Peristalsis (movement), segmentation (mixing of contents to allow everything to be absorbed) |
|
|
Function fo LI |
Most of H2O absorption occurs here. Flora within the LI can break down foods we cannot (cellulose). Retropulsion pushed food back up LI for more digestion. Haustration is a more vigerous version of segmentation to increase SA contact. Peristalsis still occurs. |
|
|
What is eliminated during defication. What controls defecation? |
Bacteria, exfoliated cells, secretions, bile breakdown products, undigested foods. The ENS controls defecation but it hands over to voluntary control once faeces arrives at the rectum. |
|
|
Describe the inputs that allow for the rhythmic peristalsis to occur. |
Pacemaker cells (called interstitial cells of Cajal) in the stomach (near greater curvature) and SI (near common bile duct) produce constant slow waves that propagate through the smooth muscle cells. But this AP is not enough to cause contraction. However, Vagal and enteric neurons can release ACh onto M2 and M3 receptors, which increases cytosolic Ca2+ allow contraction. So therefore, contraction only occurs where ACh is. Also the summation of APs can occur to cause larger contractions. |
|
|
Where are the GIT PSNS and SNS efferents coming from. |
PSNS - Upper efferents are from Vagus n (CN X) - Lower from S2/3/4 to pelvic splanchnic nn SNS - T5-9 via greater splanchnic - T9,10 via lesser splanchnic - T12 via least splanchnic - L1-2 via lumbar splanchnic |
|
|
What are the plexuses of the GI |
Myenteric Plexus - Motility Submucosal plexus - secretions and sensory |
|
|
What do the ENS inhibitory neurons release, Excitability release? |
ACh from M receptors causes excitation. VIP and NO inhibit. |
|
|
What are the 5 endocrine molecules and functions |
Gastrin - Stomach acid secretion and GO growh. Cholecystokinin - pancreatic contraction and bile secretion Secretin - controls pH via bicarbonate secretion. Gastric inhibitory peptide - insulin release and suppression of Acid production. Motilin - fasting state |
|
|
What are the paracrine factors |
Histamine and somastatin |
|
|
What are the 3 phases of digestions |
1. Cephalic - feeling hungry, tastebuds send a quick message to stomach to get reading for food. 2. Gastric phase - food is mixed with stomach acids 3. Intestinal phase - the mix the then regulated and pushed out by bit into the SI |
|
|
Describe the cephalic phase |
Smell, taste or thought of food triggers the CNS to send an impulse through the PSNS via the vagus nerve to the submucosal plexus. This plexus innervates mucous cells (mucous), chief cells (pepsinogen), parietal cells (HCl) and G cells (stimulate the release of gastrin into the blood). This all happens in preparation for food to arrive. |
|
|
Describe salivation and its reflexes. |
Simple reflex: Pressure receptors and chemoreceptors in the mouth detect information such as a dry mouth and send afferent info to the salivary centre in the medulla where it is integrated by salivatory nuclei -> then efferents are sent through the ANS visceral motor nerves to the salivary glands to begin secretion. Nerve afferents: touch - Trigeminal (CN V) Taste - facial (Vll), Glossopharyngeal (lX), Vagus (X) Nerve efferents (PSNS via CNS) - submandibular, sublingual: facial (Vll) - Parotid: glossopharyngeal (lX) |
|
|
Deglutition (Swallowing) |
It is initiated voluntarily by the pharyngeal constrictor muscles for the first 1/3 of oesophagus. Then the ENS takes over for the lower 1/3 with peristaltic waves. Upper and lower oesophageal sphincters coordinate. So swallowing can be concious and voluntary but it is also a reflex. tactile receptor at the entrance of the pharynx send sensory info to the swallowing centre in the medulla and lower pons -> motor outputs go through: - cranial nerve to pharynx and upper oesophagus - vagus to the rest of oesophagus - also the centre pauses pontine respiratory centre The sequence 1. soft palate elevates to close entry to nose 2. vocal cords close and larynx elevates 3. epiglottis closes 4. pause in breathing 5. briefly relax UES 6. contract upper oesophagus 7 peristaltic waves to the rest. If the food bolus is not moved by the 1st wave, then continued oesophageal distension triggers a secondary peristaltic wave (ENS reflex). |
|
|
vomiting |
Triggers in the medulla - SNS, PSNS activity includes: - sweating, pallor - Tachycardia, tachypnoea - salivation - increased gastric tone. The abs contract to make a pressure gradient and the LES/UES relax to allow contents to pass. Nasopharynx is closed off by palate. |
|
|
The Gastric phase |
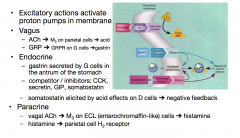
Distention in the stomach, increased pH, protein detection and peptide detection stimulated the gastric phase. ENS stimulates parietal and chief cells (ACh) and G cells (GRP) and increases motility for mixing waves Endocrine actions: peptides and AAs in the pyloric antrum are detected and stimulte G cells to release gastrin which increase parietal and chief cell secretion and also increases motility. Paracrine actions: distention + vagus stimulates ECL (enterochromaffin-like) cells to release histamine -> which stimulates parietal acid production. |
|
|
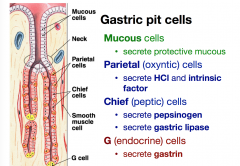
what are the cells in the gastric pits and what do they secrete? |
|
|
|
What is intrinsic factor? |
It is secreted from parietal cells along with HCl. Its job is to seek out Vit B12 and form a dimer complex. This complex is resistant to pepsin digestion. The B 12 can survive through the stomach, until it binds to a certain receptor in the iluem which allos the B 12 to be internalised. If you are defiecient in intrinsic factor => pernicious anaemia. |
|
|
How do parietal cells secrete HCl |

Acid from CO2 crossed the parietal cell membrane. Proton pump pushes H+ out and K+ in. Cl- ions go from blood to cytosol through exchange channel with HCO3- (which goes into blood) then to gastric lumen through channel, it is balanced by the K+ leak channels. |
|
|
What are the ways the proton pumps are activated? |
|
|
|
What is the function of mucous in the stomach |
Acts as a protective barrier for the cells. Pepsin constantly degrades the mucus. But mucus is constantly replaced. The epithelial cells secrete HCO3- which increases pH to ~ 7 under the mucous. This way the stomach can stay at ~pH 2 without destroying the cells. |
|
|
Basal electric rhythm |
BER pacemaker are different to other pacemaker cells, the waves are lower frequency and amplitude and are longer in duration. produced by the interstitial cells of cajal and propagated between cells through gap junctions. Different GI sections have different rhythms governed by separate clusters of ICC cells. Middle corpus - slow BER towards antrum - amplitude increases, at the pylorus the amplitude is high enough to break the AP threshold and a massively stronger contraction (as Ca++ can enter from extraceullar stores) squeezes food up against the pyloric sphincter The wave amplitude and plateau can be changed - ACh and gastrin increase - NE decreases (SNS decreases digestion) |
|
|
Regulated filling of duodenum and duodenal feedback |
stomach emptying into the duodenum is constant regardless of irregular food intake. This is important to prevent injury to the duodenum by acid. Low duodenal pH stimulates duodenal motility and decreases antrum contraction to stop acid stomach contents from entering. Also the SI digests different foods at different rates. Reflexes regulate gastric emptying depending on food composition. (the alcohol + fatty food timebomb) Duodenal feedback ENS and ANS reflexes regulate pyloric sphincter. Hormones are produced when undigested food remains in the duodenum. It is released by duodenum to compete with gastrin to decrease gastrin effect. |
|
|
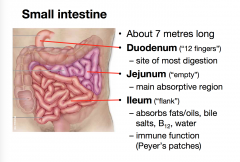
What happens most at the duodenum, jejunum and ileum? |
|
|
|
Intestinal phase of digestion |
Chyme released from the stomach into the duodenum has a negative feedback on gastric activity and stimulates antacid and chemical digestion. Processes of inhibition: - Neural: enterogastric reflex reduces gastrin production and stomach motility. - Endocrine: secretin (in response to low pH), CCK (Cholecystokinin) and GIP (in response to Lipid and Carbohydrates in Duodenum) inhibit stomach activity and stimulate pancreas to release pancreatic juice. Gastrin, CCK and insulin stimulate peristalsis. But this can be inhibited by the SNS (danger/stress) |
|
|
Cholecystokinin (CCK) |
In response to Lipid and Carbohydrates in the Duodenum -> i cells release CCK -> stimulates the gallbladder to contract and pancreatic enzyme secretion to occur. It also inhibits gastric emptying (by occupying the gastrin receptor) and Reduced appetite (CNS receptors) |
|
|
Secretin |
Low duodenal pH stimulates S cells to release secretin. This retrieves HCO3- from the pancreas, liver and brunner's glands of the duodenum to neutralise the acidic chyme. Also secretin inhibits gastric acid and pepsin secretion via VIP receptors (vasoactive intestinal polypeptide). |
|
|
GIP |
sugars/fats in the duodenum/jejunum stimulates K cells to release GIP (gastric inhibitory peptide) -> GIP stimulates pancreatic beta cells to release insulin which inhibits gastric acid secretion, gastric motility and inhibits liver glycolysis. |
|
|
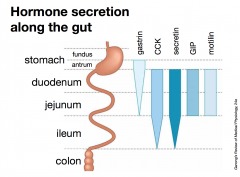
Where are the hormones in the gut found? |
|
|
|
control of pancreatic/biliary secretions |
chyme entering the duodenum stimulates the following. - slow neural Enterogastric reflex - increase in CCK (activates pancreatic enzyme secretion) and secretin (elicits alkaline pancreatic juice) - decrease in gastrin - CCK and secretin also activate gallbladder contraction and relaxes the hepatopancreatic sphincter to release bile. Pancreatic juice - aqueous component which raises duodenal pH (by secreting HCO3- and dumping H+ into ECF) is released from duct cells in response to secretin. - enzyme components lipase (TGs -> FFAs) and amylase (carbohydrates -> disaccharides) are released from acini of pancreas. |
|
|
purpose of microvilli |
maximises SA |
|
|
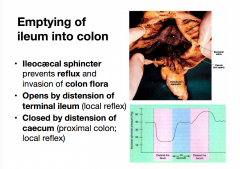
Ileum emptying into colon |
|
|
|
Main functions of the LI |
- water and ion absorption - Bioreactor and maintenance of complex flora - absorption of short chain fatty acids fro bacterial breakdown of undigested food. - storage of post digestion/faecal matter for 16-20 hours. |
|
|
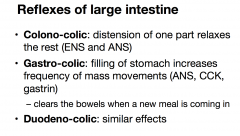
Reflexes of LI |
|
|
|
Rectum |
the rectum is usually empty due to retrograd contractions returning faeces to the sigmoid colon. Just before defecation there is a mass movement of faeces to the rectum from the sigmoid c. Visceral stretch receptors detect increase in pressure. This causes relaxation of the inner sphincter and contraction of outer sphincter. |
|
|
Defecation, whats in faeces |
- bacteria - exfoliated cells - secretions of intestinal linings like mucous - bile breakdown products - undiested or un-absorbed food intake. Delivery to rectum controlled by ENS and voiding of rectum is voluntary through relaxation of external anal sphincter (this sphincter has atypical striated muscles which are continuously contracted. The reflex for defecation is located within the sacral spinal cord, which is then voluntarily modulated. Sigmoid colon undergoes propulsive contraction. Also expiratory, lungs and abdominal muscles act to create a pressure gradient compared to the outside. Efferents: PSNS fibres located in the pelvic nerves. |
|
|
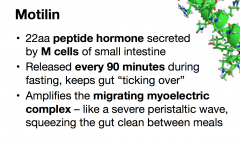
Fasting state |
Migrating myoelectic complex (MMC) removes large undigested remnants from the stomach. It is wave that occurs every 70-90 mins regardless of food input. BER frequency is similar after a meal, but amplitude is below contraction/AP threshold. |
|
|
Motilin |
|
|
|
Enterohepatic circulation of bile salts |
Hepatocytes release bile acids, then these deconjugate into bile salts in the alkaline environment of duodenum. These bile salts are reabsorbed into portal circulation back to the liver to repeat cycle. If there is failure to reabsorb this causes insufficient lipid digestion and osmotic problems later on in the colon |
|
|
regulation of body water |
Intake of water is regulated by the hypthalamus. The kidney regulate via hormones excretion of water. this balance can be upset by hyperventilation, vomiting, diarrhoea, perspiration, burns etc. water intake - metabolic (fat) - ingestion Water loss - GI tract - Lungs - skin - kidneys |
|
|
How is water absorbed in the intestines |
The intestines have large SA and are ideal for absorption. Solutes (salts) are moved mostly paracellularly (and 1/3 intracellularly) in across the intestine wall. Then water follows via osmosis paracellularly mostly (some transcellularly across lipid membrane). In the jejunum - sodium transport through uniports (for salts) and co-transporters (eith aid of glucose, AAs) In ileum and colon - sodium transport via H+ exchangers. |
|
|
Na balance |
average intake is variable:30-250 mmol/day another 250 mmol/day enters from: - salivary - gastric - biliary - intestinal secretions Pancreatic juice puts out lots of sodium but most of it is reabsorbed. Mostly by jejunum (50%), ileum (25%) and colon (variable)
|
|
|
Sodium absorption in upper SI |
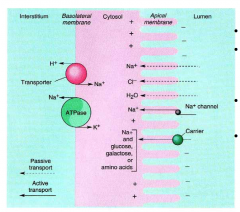
SI absorbs 95% of Na via Na+/glucose co transporter. The intracellular pH is maintained by the H+/Na+ exchanger. |
|
|
Water absorption on lower SI |
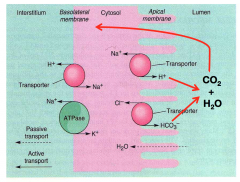
Most H2O absorption occurs from lumen across apical membrane of epithelial cells via Na+/H+ and Cl-/HCO3- exchangers In the lumen H + HCO3 -> H20 + CO2 which then diffuses back in to cells. Active secretion of Na into paracellular space occurs via osmotic absorption. |
|
|
Sodium and water absorption in LI and Diarrhoea |
Na+/H+ and Cl-/HCO3- exchanger pumps in the apical membrane of epithelial cells. In the lumen H + HCO3 -> H2O + CO2 A pH gradient running cytosol 5.5 : Lumen 7.5 affects Na+ uptake rate. If this is decreased e.g. by lactic acid from later lactose breakdown it impairs Na+ and H2O absorption -> Diarrhoea. Diarrhoea failure of water reclamation from gut lumen -> increased stool frequency, fluidity, volume. As a protective function it clear the intestine when distended, or invaded/poisoned by organisms or toxins. But negatively is is the worlds leading cause of death and disability -> hypocolaemia and CVS collapse, hypokalaemia and acid-base imbalance. |
|
|
The bristol stool scale |

Constipated: passing type 1 or 2, infrequently Diarrhoea: passing type 6 or 7, very frequently 'Normal': passing type 3 or 4 every 1-3 days, depending on the normal patterns of the individual. |
|
|
Diarrhoea and solutes |
As water follows solute, the amount of solute in the lumen is important. Release of salts by gut wall - inflammation - stimulated secretion (e.g. cholera toxin) Excess of solutes in the lumen - un-absorbable solutes (e.g. Mg2+, SO42-, sorbitol) - failure of absorption mechanisms (alcohol, coeliacs) - overwhelming of absorption (e.g lactose intolerance; bile acids in colon; coeliac) - overwhelming of absorption |
|
|
E. Coli and diarrhoea |
The E. Coli attaches to the enterocytes of the GIT via the cells own proteins -> once attached the E. Coli send signals into the cells, causing breakdown of the tight juctions between cells -> this increases permeability and allows water to seep out. |
|
|
Types of diarrhoea Physiological aetiological |
Secretory - toxins (e.g. V. Cholera) increase intracellular cAMP in crypt cells -> stims oversecretion of chloride. (cholera treated with combined glucose & Na+ rehydration) Osmotic - osmolarity of lumen contents > normal (e.g. lactase deficiency leaves lactose in lumen). This keeps water in lumen Defective ion transport - bile acids present in the colon - inflammation, decrease in Na+ absorption - congenital lack of Na+/H+ exchanger Hypermotility - bacterial toxins - transit too fast (e.g IBD) Aetiological types tumours - release secretagogues (upset normal GI secretions) Infection - if infection lingers in the small bowel, damage to mucosa can leave patients with post-enteric diarrhoea Traveller's diarrhoea - bacterial infections causing secretory diarrhoea |
|
|
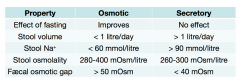
Osmotic vs secretory diarrhoea |
|
|
|
Laxatives |
same principle as diarrhoea Secretory laxatives (e.g. castor oil, fig syrup) - broken down by bacteria into stimulatory factors for the ENS -> Cl- oversecretion Osmotic laxatives (sorbitol, epsom salts - MgSO4) Fibre (indigestible cellulose) -physically retains water in colon to bulk up and plasticise faeces (thus making it easier to move) |
|
|
visceral afferents to the CNS |
The visceral afferents are 1/10 the amount of somatic afferents. Mechanical stimuli (both innocious and noxious) make up 50% of afferents Mechanically insensitive information makes up 40-50% of afferents. There is high and low threshold afferents. - low threshold (responds to distension at innocuous and noxious pressures) - High threshold aka silent fibres (responds to distension only within noxious pressures) |
|
|
visceral nociceptive pathways |
Visceral nociceptor afferents travel with ANS motor nerves and enter spinal cord via dorsal root. primary afferents make local synapses with relay neurons (These neurons share afferents from somative nociceptors) secondary visceral and secondary somatic nociceptor axons travel to thalamus and cerebrum to give sensation and experience of pain. |
|
|
nociception and pain (generally) |
nociception (noxious reception) - senses tissue damage - can cause withdrawal reflex - the information detected is quantifiable and and objective Pain sensation is the subjective interpretation of nociception + other factors emotions (distress, anxiety, fear) are significant in relation to visceral pain. |
|
|
Somatic nociception and pain |
Cutaneous - detects damage of free nerve ending in skin and near structures - produces sharp and localised pain, this pain is influenced by experience. Deep somatic - detects pressure, ischaemia, tissue damage at periosteum, muscles and tendons - resultant pain is diffuse and radiates. There is hyperalgesia on compression of site Note: there are also somatic nociceptors in the parietal structure which gives a localised pain ontop of the visceral responses. |
|
|
visceral nociception and pain |
distension, spasm, inflam or ischaemia (not necessarily related to tissue damage) of visceral organs sends info via visceral and/or vagal afferents to produce visceral responses: nausea, vomiting, sweating (all reflexes to slow the person down) Note: there are also somatic nociceptors in the parietal structure which gives a localised pain ontop of the visceral responses. Viseral pain is poorly localised, dull, felt at midline (mostly). There is no hyperalgesia on compression of site Emotional reactions: anxiousness, anguish |
|
|
visceral peripheral sensitisation |
This refers to when the nociceptor thresh hold (point at which stimuli makes AP to stim pain) is lowered. this can be caused by pro-inflammatory substances (e.g. LPS in an inflammed bladder causes greater pain response for low thresh and also turns on silent fibre (high thesh) sensation) Pro-inflammatry mediators - bradykinin - prostaglandins - substance P - serotonin - Acid (H+) "Silent" visceral C-fibres (acount for 40-50% of total afferent info) - normall unresponsive to noxious and innocuous mechanical simuli but are 'switched on' when organ is inflamed - found in bladder, bowel |
|
|
Central sensitization |
refers to the decrease of activation threshold fro the CNS nociceptive relay. It is caused by an abnormal increase in signalling from peripheral nociceptors. Thus it is more likely after peripheral sensitisation. It persists after sensitising stimulus has finished. This is because local interaction caused by the original stimulus can increase the excitability of second order nociceptor neurons. These neurons can be driven without primary input. This whole process is mediated by neuronal plasticity and glial responses to the abnormal activity levels. Inflammatory mechanisms of increased nociceptive transmission - irritation to microglia in the spinal cord can enhance nociceptive transmission across the synapse. Acitvated microglia allow the post-synaptic NMDA receptor to be open. This receptor acts as a positive feedback loop allowing more Neuron transmitters to send pain info. - Nerve damage can sensitise intact fibres and make them more responsive. |
|
|
progression of visceral pain. |
prolonged visceral nociception can create an abnormal (sensitised) sensory states. At first there is hyperalgesia from sensitisation of peripheral and central mechanisms. If extreme prolonging -> results in neuropathic pain where the system drives itself. |
|
|
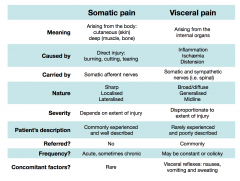
visceral vs somatic pain |
|
|
|
Convergence and referred visceral pain |
Because the viscera, skin and other structures originate from the same embryological layer, afferents from all these areas converge together and travel as one to be interpreted, even though organs may be far away from the other structures. Referred pain occurs due to confusion of where the afferents are coming from. So you may feel pain on your skin even though an internal organ tissue is actually what is damaged. Normally there is parietal localised somatic pain on the organ + referred visceral pain somewhere else on a part of skin. Segments parietal pleura, pericardium - C3-5 Heart T1-T5 Foregut T6-T9 Midgut T9-T11 Hindgut T11-L1 Kidneys T10-L1 Ureter L2 Classic example is appendicitis - visceral referred pain to the umbilical region - parietal peritoneum somatic pain at the overlying location of the appendix (RIF) |