Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
71 Cards in this Set
- Front
- Back
|
Why is Entacapone given with levodopa/carbidopa?
|
Entacapone is a COMT inhibitor and inhibits peripheral methylation.
This increases the quantity of levodopa entering the brain rather than being metabolized in the periphery. Tolcapone also does this. |
|
|
Best place to harvest great saphenous vein for CABG.
|
Just below the pubic tubercle
Note that the SMALL saphenous vein is found at the lateral aspect of the foot |
|
|
Why does squatting relieve symptoms of TOF?
|
Squatting increases systemic vascular resistance and decreases right to left shunting, thus increasing pulmonary blood flow
|
|
|
Testicular mass causing elevated hyperthyroidism:
Which mass does this and how? |
Teratomas (often found in testes and ovaries)
Structure of hCG is similar to TSH, LH, and FSH because of this, hCG can bind TSH (although with much lower affinity than TSH) Note that should use hCG as tumor marker for teratoma. |
|
|
Most common lung cancer in non-smokers
|
adenocarcinoma
|
|
|
Most drugs are eliminated through the _______.
|
Kidney--regardless of biotransformation (metabolism to active form)
Drugs with high hepatic clearance tend to have high lipophilicity and high Vd. |
|
|
What does vitamin C do and where in the cell does this take place?
|
Hydroxylation of proline (PROLINE!) and LYSINE residues
In ROUGH ER |
|
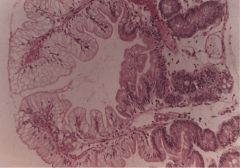
This is a jejunal biopsy.
What is this and how did it happen? |
Normal intestinal mucosa with clear ("FOAMY") cytoplasm, which is prominent on tips of villi
Occurs due to ACCUMULATION OF LIPIDS Typical of ABETALIPOPROTEINEMIA-- apolipoprotein B coats chylomicrons. Impaired synthesis of apoB results in an inability to transport lipids from intestine. This results in decreased serum levels of all lipids. Lipids are essential components of cell membranes, and their deficiency causes RBCs with abnormal membranes and thorny projections (acanthocytes). Lack of lipids in neuron membrane leads to multiple neurologic abnlts. |
|
|
What about the genetic makeup of DNA segment of interest is required in order to perform PCR?
|
Need to know bases the flank the target DNA to be amplified.
While PCR doesn't require the sequence of the target DNA be known, flanking sequences must be known to make primers. A thermostable DNA polymerase, deoxynucleotide triphosphates (to build new DNA strands) and target DNA template strand are also necessary. |
|
|
How do TNF-alpha, catecholamines, glucocorticoids, and glucagon result in insulin resistance?
|
Aberrant serine and threonine residue phosphorylation (inhibits tyrosine phosphorylation by insulin. Also hinders downstream signaling, resulting in resistance to normal actions of insulin)
Intracellular FFAs also suspected of increasing serine kinase activity as well. |
|
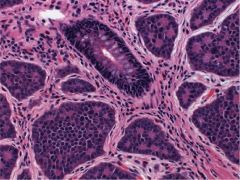
Appendix biopsy
|
Carcinoid tumor: easily recognizable as there is no variation in shape/size of tumor cells.
They grow in nests/sheets. Their granules contain secretory products of tumor cells. Most common location of intestinal carcinoids is ileum. Also frequently occur in appendix and rectum. |
|
|
Thiopental:
Drug Class |
Short-acting barbiturate used for induction of anesthesia; after equilibration with brain it rapidly redistributes into skeletal muscle and adipose tissue
|
|
|
12 year-old male falls from a tree but catches himself on a branch with his right hand.
Later presents with right hand clumsiness. What happened? |
Sudden upward stretching on arm at shoulder can damage LOWER TRUNK OF BRACHIAL PLEXUS; this trunk carries nerves from C8 to T1 that ultimately form median and ulnar nerves.
These nerves innervate all of the intrinsic muscles of the hand. |
|
|
What class of diuretic would be given to a patient with long-standing HTN, MI, crackles on lung auscultation, and edematous swelling of lower extremities.
|
Loop diuretic!!!
Likely furosemide |
|
|
Blood test for monitoring:
Warfarin therapy Heparin therapy |
Warfarin therapy monitored by measuring PT (INR)
Heparin therapy monitored by measuring PTT |
|
|
What does the PAS (periodic acid-Schiff) reaction stain?
|
Polysaccharides of fungal cell wall, mucosubstances, bm's
Also GLYCOPROTEIN of actinomycete Tropheryma whippelii (Whipple disease--presents as diarrhea, but can also affect joints, hearts, etc.) |
|
Periodic acid-Schiff reaction used on sample of intestine
|
PAS-->Whipple Disease
|
|
|
65 year-old male
Fatigue, mild normocytic anemia, anorexia Lost 10 pounds over last 2 months Irregular mass on right lung field What is causing the patient's symptoms? |
Patient has a lung neoplasm; body responds to neoplasm via macrophage release of TNF-alpha
This accounts for cachexia--anorexia, malaise, anemia, weight loss and generalized wasting due to underlying systemic dz |
|
|
Compare amount filtered with amount excreted for:
PAH Inulin Glucose Sodium Urea |
PAH: at low concentrations, completely secreted, always secreted more than filtered
Inulin: neither absorbed nor secreted, so amount filtered would = amount excreted Glucose: Completely reabsorbed at low filtered levels (so no excretion), but as filtered levels increase, will excrete more and more Sodium: Approximately 1% of sodium filtered is excreted, nearly 99% is reabsorbed!! Urea: About 40-50% of urea filtered is reabsorbed with some variable secretion; so you'd expect to see about 1/2 of urea filtered to be excreted |
|
|
46 year-old female
Persistent diarrhea, weight loss, abdominal pain Not responding to antibiotics Doesn't remit with fasting Duodenal and jejunal ulcers What hormone is elevated? |
Gastrin: neuroendocrine tumors most commonly in pacnreas/duodenum
Characterized by upper GI ulcerations (jejunal ulcers to be specific) VIPomas present with hard to control diarrhea, metabolic acidosis, and hypokalemia |
|
|
Cells that detect hypoxia and cause release of erythropoietin.
|
RENAL cortical cells (EPO release stimulates production of RBCs in BM)
|
|
|
Why does parenteral nutrition increase risk of gallstones?
|
No enteral stimulation-->no CCK release-->Biliary stasis
In those w/ileal resection, disturbance of enterohepatic bile acid circulation results in supersaturation of hepatic bile |
|
|
How do choriocarcinomas spread?
|
Hematogenously; lungs most common site of distal spread
Highly sensitive to chemo |
|
|
Enzyme deficiency in orotic aciduria.
|
Lack ornithine transcarbamoylase (enzyme that converts Carbamoyl phosphate and ornithine into citrulline)
Deficiency of this enzyme increase carbamoyl phosphate levels, which is converted to orotic acid. |
|
|
What is ferritin?
|
Stored form of iron; excellent marker of iron stores
Decreased in cases of iron deficiency and elevated in cases of iron overload It's also an acute phase reactant and may be elevated in pts w/infections or inflammatory dz |
|
|
What do transferrin levels monitor?
|
transferrin =transporter of iron; when supply of iron is dec'd, transferrin saturation drops
|
|

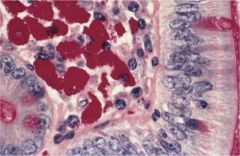
Gallbladder stone
5% cholesterol |
Black pigment stone--form when inc'd unconjugated bilirubin precipitates in bile as calcium bilirubinate
Elevated levels of unconjugated bilirubin primarily a/w chronic hemolysis (sickle cell, beta-thal, hereditary spherocytosis) |
|
|
What are the manifestations of MEN1/2A/2B?
Do not gloss this over. Be specific. |
MEN1:
Parathyroid--HYPERCALCEMIA Pancreatic (gastrin) Pituitary adenoma (prolactin, ACTH) MEN 2A: Medullary thyroid (calcitonin) Pheo (episodic HTN, and HA!!) Parathy MEN 2B: Medullary thyroid (calcitonin) Pheo Marfanoid habitus/mucosal neuromas Pheo needs to be excluded in all pts w/medullary thyroid cancer |
|
|
How does a dysplastic cell differ from carcinoma?
|
Dysplasia = REVERSIBLE change of epithelial cells
Epithelial malignancies progress through sequence of: Low-grade dysplasia (does not involve entire thickness of epithelium) -->High grade dysplasia (aka Carcinoma in situ) -->Invasive carcinoma Once dysplastic cells have breached BM (as sen in invasive carcinoma) process is no longer reversible |
|
|
What materials comprise a hamartoma?
|
Disorganized cartilage, fibrous, and adipose tissue
|
|
|
45 year-old female
Exertional dyspnea and fatigue Atrophic skin changes in hands, cold-induced digital vasospasm Accentuated second heart sound over left sternal border Pitting lower edema, hepatomegaly What is going on? Why? |
Patient has CREST syndrome---accentuated pulmonary component of second heart sound suggests increase in PA pressure-->cor pulmonale and syx of right-sided heart failure such as dyspnea on exertion, lower extremity edema and hepatomegaly
Both scleroderma and CREST develop due to increased deposition of collagen in tissues ("intimal thickening of pulmonary arterioles") Due to proliferation and accumulation of monoclonal T-cells in affected tissues that secrete a variety of cytokines, esp TGF-beta |
|
|
Measles vs Rubella:
Viral families Differences in presentation |
Measles = rubeola; paramyxovirus
Rash (koplik spots) Rubella: TOGAVIRUS; low-grade fever and skin rash that starts on face and spreads to trunk/extremities. Will also see postauricular and occipital LAD |
|
|
23 year-old heterosexual male
Hepatomegaly h/o Unprotected sex No illicit drugs What serum marker would you expect to find? |
Serum HBsAg
Although this individual isn't high risk, his clinical presentation suggests acute hepatitis B infection contracted during an episode of unprotected sex. HBV can be rspread through blood (Primary means), semen, saliva, sweat, tears, breast milk, pathologic effusions. |
|
|
20 year-old college student
Insomnia, headaches, agitation, dysphagia h/o of exploring caves No drugs or EtOH Diagnosis Treatment |
Patient has rabies encephalitis--common manifestations = nonspecific, flu-like prodrome (malaise, anorexia, mild fever, HA, nausea, vomiting)
Can also result in painful spasms with swallowing or inspiration (latter responsible for dysphagia) Postexposure prophylaxis likely isn't effective at this point, but prophylactic vaccination for indivudals at high risk of exposure to rabies virus (veterinarians, animal handlers, cave explorers, lab workers) Need to receive KILLED (INACTIVATED) vaccine--live vaccine doesn't exist for rabies |
|
|
What cell type is involved in the initial pathogenesis of atherosclerosis?
|
Thought to begin with ENDOTHELIAL CELL INJURY
Results from HTN, HLD, toxins (including EtOH); results in endothelial cell dysfn and/or exposure of subendothelial collagen (endothelial cell denudation) Denudation promotes platelet adhesion GFs produced by monocytes and platelets stimulate smooth muscle cell migration into and proliferation in the intima. At same time, inc'd endothelial cell permeability allows LDL cholesterol into intima, where it's phag'd by accumulating macrophages and smooth muscle myocytes to produce foam cells. Repetitive endothelial injury results in chronic inflammatory state. Results in progression of fatty streak within intima (containing mainly lipid-laden foam cells). |
|
|
Megaloblastic anemia
Bilateral foot numbness Difficulty walking What is deficient? |
COBALAMIN
COBALAMIN COBALAMIN |
|
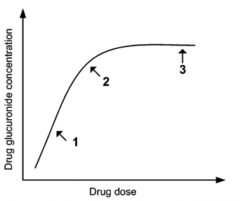
Describe the enzyme kinetics in this diagram.
|
This is a classic case of capacity-limited (saturable) enzyme kinetics.
At low doses (point 1), quantity of drug-glucuronide formed is directly proportional to dose administered. In other words, when more of drug administered, more drug-glucuronide produced. Because a fixed proportion of drug, rather than a fixed amount of drug, is converted to metabolite, early portion of graph represents first-order kinetics. Fist-order kinetics are represented graphically by a linear line with a positive slope, which indicates increase in drug dose leads to PROPORTIONAL INCREASE in metabolite conversion (point 1). When metabolizing enzyme's active sites become saturated, drug-glucuronide concentration doesn't continue to change w/increasing doses of substrate drug. It has reached its maximum capacity (Vmax). So at Point 2, the kinetics change from first-order to zero-order (saturable) kinetics--a constant amount of drug is metabolized and eliminated per unit time regardless of concentration of dose or drug. |
|
|
Where are gene-associated enhancer sequences located (in relation to gene)?
|
Variable locations; note that enhancers ≠ promoter regions (TATA, which is 25 base pairs upstream, and CAAT boxes, which is 70 base pairs upstream).
Enhancers increase rate of transcription initiation through protein binding and interactions with transcription factors bound to promoter sequences. Repressor elements are similar to enhancer elements, but they decrease instead of enhance transcription rates. |
|
|
Curling vs Cushing Stomach Ulcer
|
Curling--burns
Cushing--head trauma |
|
|
How does a stomach ulcer differ from a stomach erosion?
|
An ulcer involves the muscularis mucosa
An erosion does not involve the muscularis mucosa (it's limited to the mucosa and submucosa) |
|
|
Hyperplastic polyp vs Hamatomatous polyp
|
Hyperplastic polyps contain well-differentiated mucosal cell
Hamartomatous polyps consist of mucosal glands, smooth muscle, and connective tissue |
|
|
Which types of intestinal polyps are most likely to transform into adenocarcinoma (qualities!)
|
adenomatous polyps!! Which contain dysplastic mucosal cells and can transform into adenocarcinoma
Risk of adenocarcinoma determined by: -degree of dysplasia -VILLOUS adenomas much more likely to undergo malignant transformation than tubular adenomas -Size: adenomas >4cm have 40% risk of becoming malignant, those <1cm are most likely benign |
|
|
35 year-old patient with sickle cell goes into sepsis and dies.
What was the likely cause of his sepsis? |
At some point, patients with sickle cell disease become functionally asplenic. Asplenism puts patients at risk for infection by encapsulated organisms.
Strep pneumo is most likely cause followed by H flu |
|
|
Sickle cell patient with osteomyelitis
Cause |
Salmonella
|
|
|
Which diuretic increases longevity in patients with heart failure? Why?
|
Sprionolactone (in addition to ACEI, digoxin, diuretic)
In CHF pts, activation of renin-angiotensin-aldosterone system leads to elevated aldosterone levels. Aldosterone is known to cause ventricular remodeling leading to cardiac fibrosis. Note that while Furosemide (a loop diuretic) is a potent diuretic, it's mainly used for treating pulmonary congestion and fluid retention in heart failure patients. |
|
|
Flutamide:
MOA |
Inhibits binding to testosterone receptors
|
|
|
Describe cardiac tissue conduction velocity by region of the heart.
|
Park at Ventura Avenue
(fastest) Purkinje > Atrial> Ventricular > AV node (slowest) |
|
|
Describe phases I vs II of Schilling test (Intrinsic factor, radiolabeled B12)
|
Phase 1:
Oral radiolabeled B12 given with IM injection of non-radiolabeled B12 High urinary excretion of radioactive cobalamin during this step is e/o NORMAL ABSORPTION and dx of DIETARY B12 DEFICIENCY (need to give concomitant cobalamin during this step to create state of excess circulating B12, otherwise all of orally administered radioactive B12 would be taken up by tissues and little would be excreted in urine). Low urinary excretion of radioactive cobalamin rules out dietary deficiency and is suggestive of poor absorption of vitamin. Can result from lack of intrinsic factor (pernicious anemia) or malabsorption syndrome. Phase II: Radiolabeled B12 administered with IF and urinary excretion measured. If cause of impaired absorption is lack of IF, it will be corrected during this stage of testing and urinary excretion of radiolabeled B12 would increase. Low excretion of radiolabeled cobalamin after administration of intrinsic factor suggests another cause of poor cobalamin absorption such as pancreatic insufficiency, intestinal bacterial overgrowth or ileal disease. |
|
|
How is Bosentan useful in primary idiopathic pulmonary hypertension?
|
This is what primary idiopathic pulmonary hypertension is:
Inherited form of primary pulmonary HTN due to dec'd apoptosis of endothelial and smooth muscle cells in pulmonary arterioles (example: 36 year-old woman with dyspnea and weakness with dec'd intraluminal diameter of small branches of pulmonary artery and medial hypertrophy; mother had similar syx and died at 42) Bosentan is an enothelin-receptor antagonist. Endothelin is a potent vasoconstrictor and stimulant of endothelial proliferation. Bosentan, by blocking endothelin, has been shown to decrease pulmonary arterial pressure and lessen progression of vascular and right ventricular hypertrophy. |
|
|
Aerosol flunisolide therapy:
How does it work (drug class) |
Inhaled glucocorticoid--beware of thrush
|
|
|
48 year-old male
Small fibrotic focus in lower lobe of right lung Calcified lymph node in right lung hilus |
M tuberculosis infection
A lower lung lesion (Ghon focus) accompanied by ipsilateral hilar adenopathy is described as a Ghon complex Remember: immune response to M. tuberculosis if TH1 cell mediated, resulting in caseating necrosis where organisms are present. |
|
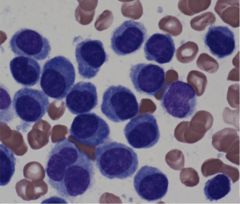
BM biopsy
|
BM infilitrated by plasma cells; note characteristic appearance of plasma cells (basophilic cytoplasm, eccentric nucleus, clock face distribution of chromatin)
This is diagnostic of multiple myeloma Expect to see: Normocytic and normochromic anemia seceondary to BM infiltration and replacement by malignant plasma cells -Secretion of IL-1 (osteoclast activating factor) and IL-6 to activate osteoclasts-->bone resorption (PUNCHED OUT LYTIC LESIONS ON X-RAY) Hypercalcemia due to inc'd bone destruction Produciton of monoclonal immunoglobulin by abnl plasma cells-->inc'd susceptibility to infection (presnce of M protein and monoclonal light chains--Bence-Jones protein in urine) AL amyloid forms due to accumuln of monoclonal immunoglobulin light chains; apple-green birefringence (AL amyloidosis contributes to dev't of renal failure in multiple myeloma) Renal failure develops due to infiltration of kidney by plasma cells, deposition of amyloid |
|
|
Punched out bone lesions
Apple green birefringence with Congo red stain |
Multiple myeloma
|
|

Diagnosis
Cause |
Acanthosis nigricans
Benign causes: insulin resistance (inc'd insulin and insulin-like GFs stimulate epidermal and dermal prolifereation)--insulin resistant states include DM, acromegaly, obesity and others Malignant acanthosis nigricans a/w underlying neoplasms, esp of GI/GU tract Sudden appearance of this in middle-aged or elderly pts is suggestive of underlying malignancy, with GASTRIC ADENOCARCINOMA the most common cause of malignant acanthosis nigricans |
|
|
29 year-old female
Decreased vision and pain around her eyes, aggravated by eye movement Intention tremor of left arm What are the eye symptoms called? What disease is this? |
Eye symptoms = optic neuritis (pain with ocular movements and dec'd vision)
Intention tremor = sign of cerebellar dysfn Both of these are seen commonly in multiple sclerosis Etiology remains unknown but is currently considered an AUTOIMMUNE DZ |
|
|
38 year-old female
Severe, right-sided facial pain Like a knife stabbing my face Instigated by meal or teeth brushing Diagnosis Treatment |
Trigeminal neuralgia--episodes of sudden and severe pain of CN V (particularly V2 and V3)--triggered by any stimulus to CN V, e.g., chewing, teeth brushing, shaving
Tx: Carbamazepine is drug of choice |
|
|
Phenytoin:
MOA |
Inhibits neuronal high-frequency firing by reducing ability of sodium channels to recover from inactivation
|
|
|
Carbamazepine:
MOA |
Inhibits neuronal high-frequency firing by reducing ability of sodium channels to recover from activation
|
|
|
Dermatologic name for a bruise by size
|
<5mm: petechiae
5mm-1cm: purpura 1cm+: ecchymoses |
|
|
Why would a patient with sickle cell present with pancytopenia?
|
Formation of autoantibodies against RBCs, WBCs, and platelets
This is a type II hypersensitivity rxn |
|
|
What spinal effects does B12 deficiency have?
|
Degeneration of dorsal columns (ascending)
and degeneration of corticospinal tract (descending) pathways Loss of position and vibration sensation, ataxia, spastic paresis are common manifestations |
|
|
What is the most common amino acid found in collagen?
|
Glycine--Gly-X-Y-333 (found in at least every third amino acid position
|
|
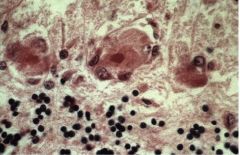
Brain biopsy
What happened and how long ago did it occur? |
Deeply eosinophilic neurons = "red neurons"--sign of irreversible neuronal injury
This is in response to inadequate blood supply to the brain, leading to ischemic stroke. These microscopic changes occur 12-24 hours after cessation of blood supply are are described as "red neurons". |
|
|
Fever, weight loss, muscle pain
Muscle biopsy shows transmural inflammation of arteries with fibrinoid necrosis What is this and what disease is it associated with? |
Transmural inflammation of arterial wall with fibrinoid necrosis = POLYARTERITIS NODOSA
Inflammation can occur in any organ with exception of lung Associated with HEPATITIS B INFECTION in 10 to 30% of cases |
|
|
What problem does a decreased angle between the aorta and SMA develops?
|
Entrapment of the transverse portion of the duodenum between the SAM and aorta--causes partial intestinal obstruction (bilious vomiting!)
|
|
|
40 year-old man with pain on defecation
Pain is sharp and severe, but subsides within minutes of passing bowel movement He sees spots of bright red blood on toilet paper Rectal exam reveals tear of anal mucosa What are these tears called? Where are they mostly likely to occur? |
This is an anal fissure (a longitudinal tear in the mucosa of the distal anal canal)
Majority occur at POSTERIOR MIDLINE of ANAL VERGE This is bc the posterior anaal canal is poorly perfused and makes its mucosa sensitive to trauma by hard fecal masses--anal fissures are a/w constipation and low-fiber diets |
|
|
HbA1c vs HbA2:
What does HbA1c measure? When is HbA2 elevated? |
HbA1c is glycosylated hemoglobin A1 (HbA1 = alpha2beta2); in normal adults, HbA1 makes up about 97% of total hemoglobin, while HbA2 (alpha2delta2) makes up about 2.5% and fetal Hg makes up less than 1%
HbA2 is elevated in beta-thalassemia to compensate for decreased synthesis of HbA1 that results form beta-globin chain UNDERProduction Note that in sickle cell, the HbS percentage is increased and the HbA21 levels are reduced. HbA2 percentage is normal. |
|
|
4 year-old male
Fever, bilateral conjunctivitis, bright red tongue Skin on fingertips is sloughing What disease is this? What is this patient at risk of? |
Kawasaki disease is a vasculitis of medium-sized arteries that affects very young children. Presents with:
-STRAWBERRY TONGUE -edema of hands, feet, palms, soles; desquamation of fingertips (periungal) Generalized rash (beginning on extremities and moving to trunk) Lethal Complication= CORONARY ARTERY ANEURSYM |
|

What disease is this?
What specific damage occurs? |
This is Wilson's Disease (Kayser-Fleischer rings)--rare, autosomal recessive disease
Copper accumulation will cause damage to hepatic tissue through generation of free radicals. From there it will leak from hepatocytes into blood and deposit in cornea, basal ganglia. Will results in BASAL GANGLIA ATROPHY. |
|
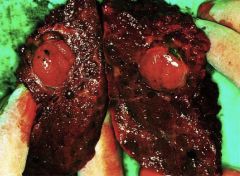
What is this?
|
Hepatocellular carcinoma
|
|
|
There are three types of Rapidly Progressive GN:
Type 1: Goodpasture's Type 2: Immune-complex Type 3: Pauci immune List what you can about each. |
Type 1: Linear GBM deposits of IgG and C3; anti-GBM ab's cross-react w/pulmonary alveolar BM's, producing pulmonary hemorrhages (hemoptysis)
Type 2: Lumpy bumpy granular pattern; complication of poststreptococcal GN, SLE, IgA nepropathy, or Henoch-Schonlein purpura Type 3: Pauci Immune--no immunoglobulin or complement deposits; associated with ANCA (C-Wegener's) |