Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
61 Cards in this Set
- Front
- Back
|
2 day-old neonate
Persistent vomiting Atresia of large small bowel Apple peel appearance Diagnosis Pathophys |
Jejunal, ileal, and colonic atresia are not caused by abnormal fetal development (they are not congenital malformation)
They're results of diminished intestinal perfusion in utero, which leads to ischemia of a segment of bowel, with subsequent narroiwng or obliteration of the lumen. If a major vessel is occluded (such as the SMA), the area of intestinal wall necrosis is large. |
|
|
Apple peel atresia in neonate
|
Vascular blockage in utero leading to bowel ischemia
|
|
|
Describe the process of T cell maturation.
Where does it occur? |
In Thymus, T-cell Receptor (TCR) gene rearrangement, positive selection, negative selection and expresison of ECM markers and co-stimulatory molecules occur
Pro-T cells are double negative (lack both CD4 and CD8) Then acquire both CD4 and CD8 ("double positive" AKA immature T cells) FInal step in maturation is los sof either CD4 or CD8 |
|
|
Efficacy vs Potency
|
Efficacy - intrinsic ability of a drug to elicit an effect (such as receptor activation or dilation of a vessel). It's measured by maximum ceiling of activity (Vmax).
Potency - drugs that bind receptors with a higher affinity or are able to better access target wtissues will have greater potency. Potency of different agents can be determined by dose of drug required to produce one-half (50%) of the maximum biological response (ED50). |
|
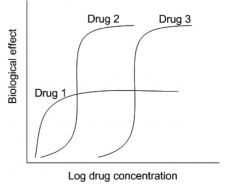
Compare drug efficacy and potency.
|
A much lower dose of drug 2 is required to produce the same effect as seen with drug 3, so Drug 2 is more potent than drug 3 and has a lower ED50. TO achieve higher potency, binding of drug 2 to its receptors must be higher than that of drug 3.
Drug 1 has a higher potency than Drug 2 because at low biological activity, it can cause same effect with much lower concentrations of drug. Drug 1 demonstrates the lowest efficacy (ceiling of biological effect) of the three drugs graphed. Drug 2 has a lower ED50 (greater potency) than drug 3. Both have equal efficacy. |
|
|
What cranial nerves can be affected by intracranial schwannomas?
|
CN VIII (duh)--hearing loss and difficulty balancing
CN VII--facial paralysis CN V--loss of sensation around mouth/nose, loss of corneal reflex, paralysis of muscles of mastication |
|
|
3 ways to get Down Syndrome.
|
1) Meiotic non-disjunction (Trisomy 21)--95% of cases
2) Unbalanced Robertsonian Translocation 3) Genetic mosaicism--parents have two cell lines--one with a normal genotype and one with trisomy 21 |
|
|
______ disomy exists in a ______ hydatidiform mole.
|
Paternal disomy exists in a complete mole.
|
|
|
Beginning with endothelial cell injury, describe the pathogenesis of atherosclerotic plaques.
|
Endothelial cell injury-->exposure of subendothelial collagen (endothelial cell denudation)
Promotes PLT adhesion, aggregation, release of factors that promote migration of smooth muscle cells from media into intima, as well as SMC proliferation These factors must include PDGF and TGF-beta. |
|
|
How would a prolactinoma predispose a patient to osteoporosis?
|
High levels of prolactin suppress GnRH secretion from the thypothalamus.
Leads to decreased estrogen levels. |
|
|
Phencyclidine abuse:
MOA Presentation |
Hallucinogen that inhibits NMDA receptor
Presents as slurred speech, ataxia, nystagmus, HOSTILE AND AGGRESSIVE behavior--may be indistinguishable from schizophrenia |
|
|
Which anti-tb agents are used for extracellular tb? Intracellular? Why?
|
Extracellular: INH (inhibits mycolic acid synthesis--important for Tb cell walls), Ethambutol (inhibits arabinosyl transferase--impt for cell wall synthesis), Rifampin (inhibits DNA-dependent RNA polymerase)
Intracellular: Pyrazinamide--requires an acidic environment (as is present within macrophage phagolysosomes) to exert effects. |
|
|
57 year-old man
Right-sided eye pain, ipsilateral headache Reports severe nausea and seeing halos Diagnosis Treatment Treatment MOA |
Acute close-angle glaucoma
Treat with acetazolamide (carbonic anhydrase inhibitor)--acts in PCT and enhances HCO3- and H2O excretion as well as inc'd urinary pH (potential for metabolic acidosis) |
|
|
What reactions are affected by biotin deficiencies?
|
1) Inc'd pyruvate-->converted to lactic acid (LACTIC ACIDOSIS)
2) Build up of propionyl CoA and metabolized into surplus of odd-chain fatty acids (need biotin to synthesize succinyl Coa from amino acids such as valine) 3) Need biotin for Pyruvate-->Acetate |
|
|
What features of Grave Disease are not found in other causes of hyperthyroidism?
|
Exophthalmos
Infiltrative dermopathy (PRETIBIAL MYXEDEMA--infiltrative accumuln of glycosaminoglycans in dermis. Results in non-pitting edema sometimes scaly in appearance, resembles an "orange peel") |
|
|
How can ether help identify viruses?
|
Ether and other organic solvents dissolve the lipid bilayer that makes up the viral outer envelope.
Loss of infectivity after exposure to ether is characteristic of enveloped viruses. |
|

36 year-old male
Hemoptysis, HTN, hematuria Alcohol-fixed neutrophils treated with patient's serum demonstrate indirect immunofluorescence (see image) Diagnosis Pathophys |
Image shows positive-cANCA (cytoplasmic antineutrophil cytoplasmic Ab)--seen in Wegener's (a necrotizing granulomatous vasculitis)
Syx: Hemotpysis, chronic sinusitis/mucosal ulceration, rapidly progressive (CRESCENTIC) GLOMERULONEPHRITIS |
|

|
p-anca stain
|
|

|
c-anca stain
|
|
|
False vs True Diverticula:
Differences Examples |
False: only contain mucosa and submucosa. These layers herniate through defects in muscular layer. Ex: Zenker (upper esophageal) diverticula.
True: Consists of all parts of intestinal wall: contains mucosa, submucosa, muscularis. Often contains ectopic mucosa (gastric epithelium and pancreatic most common). Ex: Meckel's diveritculum |
|
|
34 year-old alcoholic
Vomiting, prolonged oliguria Vacuolar degeneration and ballooning of proximal renal tubules Oxalate crystals in tubular lumen Diagnosis Pathophys |
Patient likely ingested ethylene glycol which is widely-available and found in antifreeze, engine coolant, hydraulic brake fluids.
Metabolized to glycolic acid, which is TOXIC TO RENAL TUBULES. Damage manifests itself as ballooning and vacuolar degeneration (predom in PCTs). Leads to actue renal failure due to precipitation of calcium oxalate crystals. Will also see anion gap metabolic acidosis. |
|
|
Where is the primary site of potassium absorption? Secretion?
|
Majority of potassium is absorbed in the proximal tubule.
Potassium regulation (secretion) occurs in collecting duct. |
|
|
18 year-old girl
Nausea, vomiting, abdominal pain, bloody diarrhea Garlic odor breath BP 90/60 Consumed insecticide Type of poison Treatment Treatment MOA |
Arsenic Poisoning
Treat with Dimercaprol Dimercaprol is a chelating agent that will displace arsenic ions from enzymes. |
|
|
CaN2EDTA:
Use |
Lead, Mercury poisoning
|
|
|
Methylene Blue:
Use |
Treatment of methemoglobinemia (converts iron in heme from Fe3+ to Fe2+)
|
|
|
Beginning in the marrow, outline the process of T cell maturation. Include selection processes and interactions required.
|
T cells initially produced in BM; migrate to Thymus
Pro-T cells arrive as double negative cells in subcapsular zone TCR rearrangement occurs to form double-positives In thymic cortex: positive selection allows T cells expressing TCR able to bind self MHC to survive. Cells expressing a TCR unspecific for self MHC signaled for elimination by apoptosis. Requires THYMIC CORTICAL EPITHELIAL CELLS. Positive selection responsible for dev't of T cell repertoire that can recognize self. Negative selection: TCRs that bind w/high affinity to self Ag or self MHC eliminated by apoptosis. Requires THYMIC MEDULLARY EPITHELIAL and DENDRITIC CELLS. Serves to eliminate T cells that may be overly autoreactive against self-Ag. |
|
|
Aortic rupture due to MVA:
Most common site of rupture |
Aortic isthmus: where ascending aorta becomes descending (at branch of subclavian)
|
|
|
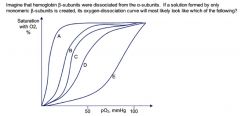
The answer is A.
Remember: Hgb A is composed of two alpha and two beta chains. Myoglobin is a monomeric protein and the primary oxygen-carrying protein of skeletal and cardiac muscles. The beta-subunits of hemoglobin and myoglobin are identical. As are the alpha-subunits. P50 of Hgb is ~26mmHg, P50 myoglobin ~1mmHg Each globular subunit of Hgb assocd w/1 heme group so a single Hgb molecule is able to carry 4 heme groups. HOWEVER, each myoglobin carries only 1 heme group. Additionally, after binding to one oxygen molecule, the affinity of other heme molecules for O2 increases (heme-heme interaction), accounting for sigmoidal shape of Hgb curve. Myoglobin has a much higher affinity for oxygen and doesn't experience heme-heme interactions; therefore, its oxygen-dissocn curve is hyperbolic. |
|
|
Amphotericin B:
MOA Toxicities and their MOA |
MOA: Binds ergosterol of fungal cell membranes, leading to fungal cell lysis. Relatively selective since has a higher affinity for ergosterol (in fungal membranes) than for cholesterol (in human cell membranes). However, it does bind cholesterol to a degree which explains its AEs:
1) Infusion-related reactions (fever, chills, hypotn). Prevent w/antihistamines and antipyretics. 2) Dose-dependent nephrotoxicity bc it decreases GFR. 3) Electrolyte abnlts (hypoMg, hypoK) 4) Anemia due to suppression of renal EPO synthesis 5) Thrombophlebitis at site of injection |
|
|
What accounts for the significant increase in nosocomial staphylococcal infections (bacteremia and sepsis) over the last 20 years?
|
Intravascular devices
|
|
|
23 year-old male
Urinalysis positive for reducing sugar, negative for glucose PMH unremarkable No specific diet Diagnosis Pathophys |
Essentil fructosuria--benign disorder resulting from a defect or deficiency in FRUCTOKINASE.
PLEASE NOTE: this differs from hereditary fructose intolerance and classic galactosemia in that these disorders will be SYMPTOMATIC (failure to thrive, hepatomegaly--due to inability to breakdown sugars, cirrhosis) |
|
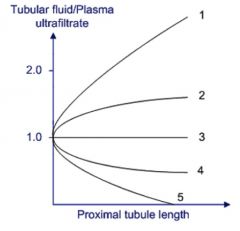
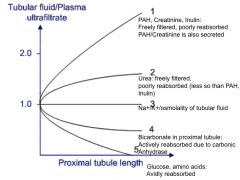
Label and explain
|
|
|
|
Telomerase:
Function Role in oncogenesis |
Telomerase is a reverse transcriptase enzyme (RNA-dependent DNA polymerase) that adds TTAGGGG repeats to 3' end of DNA strands.
Stem cells have very long telomeres and active telomerase, but with every division, length of telomeres shortens. Terminally differentiated adult somatic cells have very short telomeres. Thought to be a signal for programmed cell death. Cancer cells up-regulate telomerase activity, preventing cellular death. They're considered immortal. |
|
|
This bacterial exotoxin inactivates 60S ribosomal subunit.
|
Shiga toxin (of both shigella and EHEC)
|
|
|
Cryptococcus:
Sources Route of infection |
Present in soil/pigeon droppings
Yeast transmitted via respiratory route, with lungs as primary site of entry |
|
|
What are the molecular effects of multiple sclerosis?
|
Loss of myelin sheaths
Depletion of oligodendrocytes Oligoclonal bands of IgG in CSF Will also see lipid laden macrophages containing products of myelin breakdown |
|
|
32 year-old male
h/o PCP pneumonia Severe chest pain on swallowing Endoscopy reveals hyperemia, ulcerations of esophageal mucosa Differential |
Patient is likely HIV-infected, as Pneumocystis jiroveci affects exclusively immunocompromised individuals.
Patient presents w/painful swallowing, which is characteristic of esophagitis. 3 main causes of HIV-associated esophagitis: Candida CMV HSV |
|
|
Babesiosis:
Pathophys |
Transmitted by tick bite. Endemic in NE US w/influenza-like syx, HSM, anemia. Often affects asplenic pts.
|
|
|
26 year-old male
h/o childhood dermatitis, asthma, hay fever Applies corticosteroid to flexor areas Areas remain free of lesions and scales What would biopsy show? How would this differ if he didn't use the steroid cream? |
Patient is being treated for atopic eczematous dermatitis.
Histologic findings of active eczema include: -intraepidermal vesicles -epidermal hyperkeratosis -scales epidermal hyperplasia (acanthosis) -chronic inflammatory infiltrate within dermis Corticosteroids decrease production of ECM collagen and glycosaminoglycans. Consequences include atrophy of dermis w/loss of dermal collagen, drying, cracking, and/or tightening of skin. Telangiectasia, ecchymoses from mild trauma, and atrophic striae may also be found. |
|
|
Risk of rapid correction of chronic hyponatremia?
Presentation Pathophys |
Osmotic demyelination of axons in central part of pons
Called central pontine myeloniolysis Presents as quadriplegia due to demyelination of corticospinal tracts and pseudobulbar palsy. |
|
|
56 year-old male
HIV positive Weight loss, fevers, weakness HSM Blood cultures reveal acid-fast bacteria that grow best at 41ºC Diagnosis Treatment |
Infection with Mycobacerium avium complex (MAC)
MAC can affect both immunocompetent and immunosuppressed hosts Entry through respiratory route Tx: Clarirthromycin or Azithromycin with any combination of rifabutin and/or ethambutol Weekly prophylaxis w/azithromycin recommended for CD4<50 |
|
|
22 year-old male
Severe HA, vomiting Goes into coma and dies Autopsy shows ruptured cerebral aneurysm with extensive intracranial hemorrhage Diagnosis Other symptoms |
Since there is no h/o head trauma, patient likely suffered spontaneous intracranial hemorrhage. Most common causes are arteriovenous malformations, ruptured cerebral aneurysms, or abuse of sympathomimetic drugs such as cocaine.
BERRY ANEURYSMS are particularly PRONE TO RUPTURE WITH AORTIC COARCTATION because of HTN in branches of aortic arch proximal to coarct. SAH is the result. |
|
|
66 year-old male
Recent diagnosis of lung cancer Dizziness, dysarthria, limb ataxia Autopsy shows extensive cerebellar Purkinje cell degeneration Diagnosis Pathophys |
Paraneoplastic syndrome from lung cancer--caused by substances produced from tumor cells that induce an autoimmune response, with Abs produced against tumor cells cross-reacting w/body's own healthy organs and tissues.
Paraneoplastic cerebellar degeneration is a type of paraneoplastic syndrome most commonly assocd w/cancer of lung, breast, ovary, uterus, and lymphoma. |
|
|
Orthopnea:
Pathophys |
Results from acute exacerbation of baseline pulmonary edema that occurs when cetnral venous, pulmonary venous, and cardiac filling pressures are increased by redistribution of blood that had been pooled in dependent veins back into central circulation.
Seen in LEFT HEART FAILURE |
|
|
ANP vs BNP:
Where is each secreted from? When is each secreted? Function? |
ANP secreted by atria, and in some cases, ventricles in response to volume overload. Also released in response to HYPERTROPHY.
BNP predominantly secreted by ventricles, also in response to volume overload. These peptides facilitate natriuresis and diuresis. |
|
|
8 year-old male
2 day h/o fever, abdominal pain, diarrhea Stool negative for O&P Patient's pet had diarrhea one week ago Diagnosis |
Campylobacter jejuni
|
|
|
What is the cause of Guillain-Barre?
|
Campylobacter jejuni
|
|
|
23 year-old female
Acute pancreatitis that resolves on fasting PMH unremarkable Denies alcohol use Diagnosis Cause |
Gallstones typically affect middle-aged and older patients unless there is a predisposing condition (young patient w/sickle cell for example)
This patient is unlikely to have gallstones and does not consume alcohol, so must be a less common cause: -Recent ERCP (endoscopic retrograde chalongiopancreatography) -HYPERTRIGLYCERIDEMIA (not hypercholesterolemia!!) |
|
|
77 year-old male
BP 170/70 Returns with bilateral ankles swelling and flushing Diagnosis What drug was given? |
Patient has isolated systolic HTN (common form of HTN)
Thiazide diuretics and dihydropyridine calcium antagonists are first-line treatment for isolated systolic HTN Side effect profile most consistent with amlodipine |
|
|
Side effects of CCBs (dihydropyridine)
|
Flushing
Ankle swelling |
|
|
t(9;22):
Diagnosis Associated protein Treatment |
CML
bcr-abl Imatinib |
|
|
Atypical antipsychotics:
List them How do they differ from typical antipsychotics? |
Antipsychotic ROCS!
Risperidone Olanzapine Clozapine Quetiapine (Seroquel) Atypicals can treat both positive and negative syx of schizophrenia |
|
|
How does Crohn's disease contribute to kidney stones?
|
Wehn wall of terminal ileum is inflamed, most bile acids are lost with feces, which causes impaired fat absorption. Calcium then binds to lipids, making it unavailable for complexing with oxalate. The excess lipids are excreted with feces.
As a result, increased oxalate is absorbed, promoting formation of urinary stones. |
|
|
What key growth factors promote angiogenesis?
|
VEGF
FGF (fibroblast growth factor) |
|
|
Which cytokines increase the expression of VEGF?
|
IL-1, IFN-gamma
|
|
|
35 year-old IVDU
Fever, jaundice, anorexia Liver biopsy reveals mononuclear infiltrates, hepatocyte swelling, acidophilic bodies What are the acidophilic bodies a result of? What are these bodies called? |
Fever, jaundice, anorexia-->acute viral hepatitis
All of hepatotropic viruses that cause acute viral hepatitis produce the same histopathologic findings: hepatocyte necrosis and apoptosis Acidophilic bodies = COUNCILMAN BODIES or APOPTOTIC BODIES |
|
|
A 34 year-old male receives a kidney transplant. His T-lymphocytes quickly recognize the foreign HLA molecules of the renal transplant cells.
Inhibition of what substance would reduce the proliferation and differentiation of these T lymphocytes? How? |
Calcineurin--essential protein in activation of IL-2, whoch promotes growth and differentiation of T cells.
Immunosuppressants such as cyclosporine and tacrolimus work by inhibiting calcineurin activation. |
|
|
2 equations for cardiac output.
|
CO = SV x HR
CO = O2 consumption/arteriovenous O2 difference |
|
|
Bronchi reveal thickened bronchial walls, neutrophilic infiltrates, mucous gland enlargement and patchy squamous metaplasia of bronchial mucosa.
Diagnosis Cause |
Chronic bronchitis.
Cigarette smoking. |
|
|
Wide, fixed splitting of S2
|
Atrial Septal defect
|
|
|
What is Eisenmenger syndrome and what vessels are affected?
|
ASD creases a LtoR shunt because of high pressure in LA. Increased flow through pulmonary artery, which may develop medial hypertrophy.
At this point, pressure builds and flow becomes Rto (presenting w/late cyanosis). Eisenmenger syndrome = name for reversal of shunt flow. Over time, pulmonary vascular sclerosis becomes irreversible. |