Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
46 Cards in this Set
- Front
- Back
|
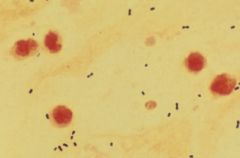
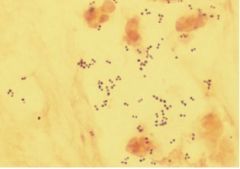
Strep pneumoniae. Sputum sample showing gram-positive diplococci.
|
|
|
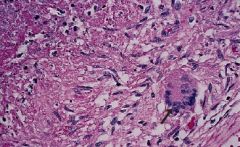
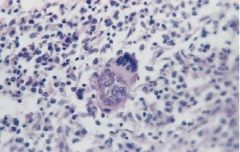
Mycobacterium TB. Caseating granulomas containing Langhan's giant cells, which have a "horseshoe" pattern of nuclei.
|
|
|
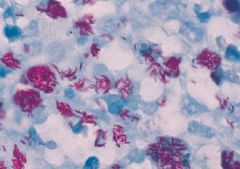
Mycobacterium TB. Organisms are identified by their red color on acid-fast stain ("red snappers.")
|
|
|
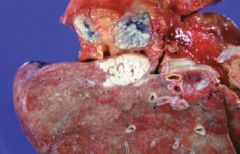
Mycobacterium TB. Miliary TB is seen here w/ large caseous lesions at the left medial upper lobe and miliary lesionsin the surrounding hilar node. This life-threatening infection is caused by blood-borne dissemination of Mycobacterium TB to many organs from a quiescent site of infection.
|
|
|
Staph aureus. Sputum sample from a pt w/ pneumonia shows gram-positive cocci in clusters.
|
|
|
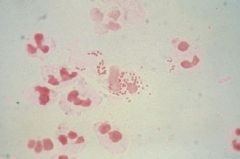
Neisseria gonorrhoeae. Gram stain shows multiple gram-negative diplococci within PMNs as well as in the extracellular areas of a smear from a urethral discharge.
|
|

|
Giardia lamblia in the small intestine. The trophozoite has a classic pear shape, with double nuclei giving an "owls-eye" appearance.
|
|
|
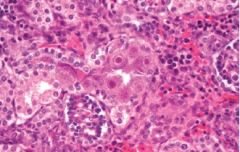
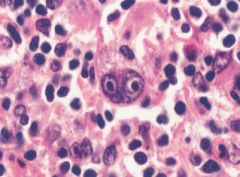
CMV. Renal tubular cells in a neonate w/ congenital CMV infection show prominent Cowdry type A nuclear inclusions resembling owls eyes.
|
|
|
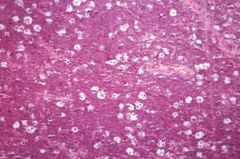
Coccidioidomycosis. Endospores within a spherule in infected lung parenchyma. Initial infection usually resolves spontaneously, but when immunity is compromised, dissemination to almost any organ can occur. Endemic in SW US.
|
|

|
Cryptococcus neoformans. The polysaccharide capsule is visible by India ink preparation in CSF from an AIDS pt w/ meningoencephalitis.
|
|

|
Candida albicans. KOH prep showing branched and budding C. albicans.
|
|
|
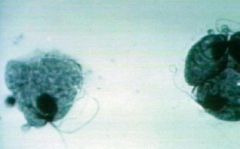
Trichomonas vaginalis demonstrating trophozoites w/ flagellae.
|
|

|
Herpes genitalis. Ulcerating vesicles from HSV-2.
|
|

|
Primary syphilis. Painless chancre.
|
|
|
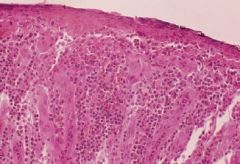
Primary syphilis. A dense infiltrate of plasma cells and dilated blood vessels can be seen. There is epidermal ulceration with crust; PMNs are present within the predominantly plasmacytic infiltrate.
|
|
|
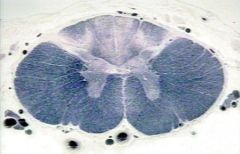
Tabes dorsalis from progressive syphilis infection, affecting the thoracic spinal cord. Note degeneration of the dorsal columns and dorsal roots.
|
|

|
Bacterial vaginosis. Saline wet mount of clue cells. Note the absence of inflammatory cells.
|
|

|
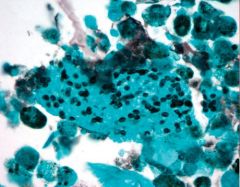
HPV. Metastatic epithelium at the cervical squamocolumnar junction.
|
|

|
Coxsackie exanthem (hand-foot-mouth disease.) Diffuse eruptive vesiculopapules are seen on the hand of a 3-year-old.
|
|
|
Pneumocystis carinii. Special silver stain of lung epithelium shows numerous small, disk-shaped organisms.
|
|
|
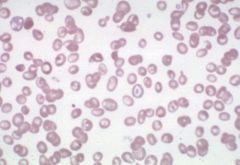
Target cells. Due to an increase in surface area-to-volume ratio from IDA (decreased cell volume) or obstructive liver disease (increased cell membrane.)
|
|
|
Thalassemia major. A blood dyscrasia caused by a defect in beta-chain synthesis in hemoglobin. Note the presence of target cells.
|
|
|
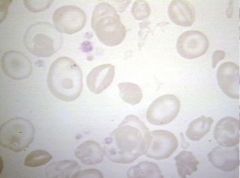
IDA. Microcytosis and hypochromia can be seen.
|
|
|
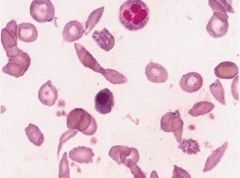
Sickle cell anemia on peripheral blood smear. Note the sickled cells as well as anisocytosis, poikilocytosis, and nucleated RBCs.
|
|

|
Splenic infarction from sickle cell anemia. The splenic artery lacks collateral supply, making the spleen particularly susceptible to ischemic damage. Coagulative necrosis has occurred in a wedge shape along the pattern of vascular supply. Individual sickle cells cause generalized splenic infarcts that result in autosplenectomy by adolescence.
|
|

|
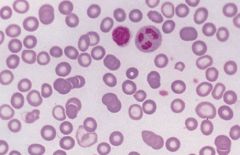
ALL peripheral blood smear. Affects children < 10 yo.
|
|

|
AML with Auer rods. Affects adolescents to young adults.
|
|
|
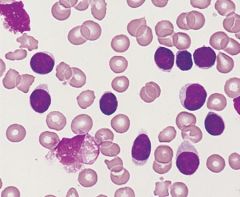
CLL. The lymphocytes are excessively fragile and easily destroyed during slide prep, forming "smudge cells." Affects individuals > 60 yo.
|
|
|
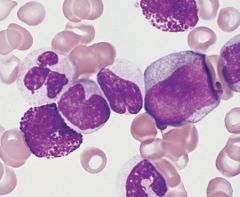
CML. Promyelocytes and myelocytes are seen adjacent to a vascular structure. Affects individuals 30-60 yo.
|
|

|
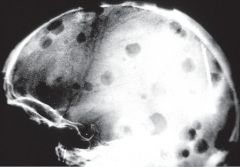
Multiple myeloma. X-ray showing numerous punched-out lytic lesions. Note generalized osteopenia and multiple compression fractures.
|
|
|
Multiple myeloma. Classic bone lytic lesions.
|
|
|
Multiple myeloma. Smears show an abundance of plasma cells. RBCs will often be seen in rouleaux formation. MM is a/w hypercalcemia, lytic bone lesions, and renal insufficiency due to Bence Jones (light-chain) proteinuria.
|
|
|
|
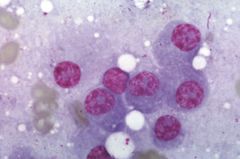
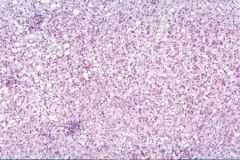
Burkitt's lymphoma. Classic "starry sky" appearance from macrophage ingestion of tumor cells.
|
|
|
Burkitt's lymphoma. Classic "starry sky" appearance from macrophage ingestion of tumor cells.
|
|
|
Hodgkin's disease. Binucleate Reed-Sternberg cells w/ prominent inclusion-like nucleoli surrounded by lymphocytes and other reactive inflammatory cells. The RS cell is a necessary but insufficient pathologic finding for the diagnosis of Hodgkin's.
|
|
|
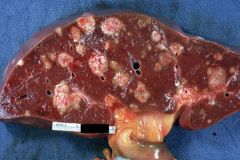
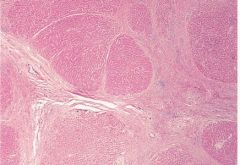
Metastatic carcinoma to the liver. The MC primary sites are the breast, colon, and lung. Primary tumors of the liver are less common than metastatic disease.
|
|
|
Fatty metamorphosis (macrovesicular steatosis) of the liver. Early reversible change a/w alcohol consumption. There are abundant fat-filled vacuoles, but as yet there is no inflammation due to fibrosis or more serious alcoholic liver damage.
|
|

|
Micronodular cirrhosis of the liver from an alcoholic patient. The liver is approximately normal in size with a fine, granular appearance. Later stages of disease result in an irregularly shrunken liver with larger nodules, giving it a "hobnail" appearance.
|
|
|
Cirrosis. Regenerative lesions are surrounded by fibrotic bands of collagen ("bridging fibrosis,") forming the characteristic nodularity.
|
|
|
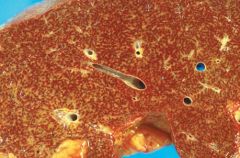
Cirrhosis. Chronic passive biliary congestion gives the liver a "nutmeg" appearance.
|
|
|
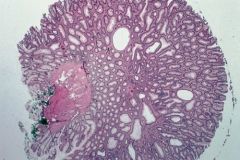
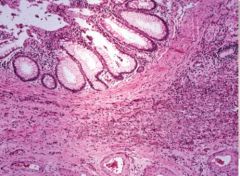
Colonic polyps - tubular adenomas - smaller and rounded in morphology than villous adenomas, and have less malignant potential.
|
|
|
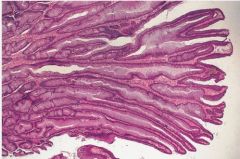
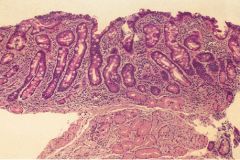
Colonic polyps - villous adenomas - composed of long, fingerlike projections. Greater metastatic potential than tubular adenomas.
|
|
|
Diverticulitis. Inflammation of the diverticula typically causes LLQ pain and can progress to perforation, peritonitis, abscess formation, or bowel stenosis. Note the presence of macrophages. Gut lumen is seen at the top.
|
|
|
Celiac sprue. Histology shows blunting of villi and crypt hyperplasia.
|
|
|
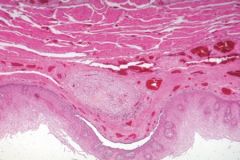
Sclerosed esophageal varix. Overlying esophageal mucosa is generally normal.
|
|

|
Intussusception of infant gut.
|