Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
34 Cards in this Set
- Front
- Back
|
ebstein anomaly
|
assoc w/ lithium in preggers
tricuspid insuficiency |
|
|
pyloric stenosis race? sex? tx?
|
whites of Scandinavian decent and males outnumber females by a ratio of 4:1.
pyloromyotomy. This involves cutting of the thickened pyloric musculature while preserving the mucosal layer. |
|
|
AA developed pallor, dark urine, and jaundice over the past few days and is taking sulfa drugs, antimalarials, nitrofurans, naphthalene mothballs, or has an infection. Dx? Path?
|
G6PD path?
Deficiency of G6PD compromises the generation of reduced glutathione and upon exposure to oxidant agents such as sulfa drugs, antimalarials, nitrofurans, naphthalene mothballs, or infection, a hemolytic episode usually occurs. |
|
|
AA developed pallor, dark urine, and jaundice over the past few days and is taking sulfa drugs, antimalarials, nitrofurans, naphthalene mothballs, or has an infection. CBC smear?
|
The older RBCs containing Heinz bodies (insoluble precipitates resulting from oxidation), the "bite cells" (RBCs after the removal of the Heinz bodies), and cell fragments are removed from the circulation within 3 to 4 days.
|
|
|
older than 4 y/o w/ Chronic constipation and fecal incontinence b/c unaware that needs to go. Dx? Tx?
|
Encopresis due to overflow incontinence (retentive encopresis), leakage of liquid stool around a large fecal impaction, resulting in fecal soiling.
Treatment involves clearing the fecal mass, maintaining soft stools for a short period of time with mineral oil or stool softeners (3-6 months), and behavioral modification. |
|
|
Rotator cuff tendinitis of the biceps and/or the supraspinatus muscles. SPORT
|
SWIMMING
|
|
|
shortness of stature, mental retardation, increased bone density, brachydactyly (especially of the fourth and fifth digits), obesity with round facies and short neck, subcapsular cataracts, cutaneous and subcutaneous calcifications, and perivascular calcifications of the basal ganglia.
|
pseudohypoparathyroidism (Albright hereditary osteodystrophy).
low calcium, high phosphorus w/ high parathyroid hormone levels are high, indicating resistance to the action of this hormone. Parathyroid hormone infusion does not produce a phosphaturic response. |
|
|
infant has fusion of the eyebrows, heterochromic irises, a broad nasal root with lateral displacement of the medial canthi, and a white forelock. What is the major abnormality likely to be associated with?
|
Waardenburg syndrome
autosomal dominant trait deafness in 20% of cases. |
|
|
flank pain, chills, N/V polyuria, dysuria, fever, costovertebral tenderness.
|
pyelonephritis
|
|
|
what ages do kids start to engage in fantasy play?
|
Between the ages of 2 and 4, children attempt to master a world that is largely outside of their control
|
|
|
child refuses to walk, has fever, has significant pain with external rotation of the right leg, and has an elevated WBC count? DX?
|
Septic arthritis
Legg-Calvé-Perthes usually presents with a painless limp |
|
|
hyaline membrane disease (infant respiratory distress syndrome) is associated with a cardiac shunt in which direction?
|
significant right-to-left shunt of blood can occur - patent ductus arteriosus or foramen ovale, and some can be due to shunting within the lung. Also think that the neonate right heart is bigger and will be able to generate greater pressure
|
|
|
the most common reason for a psychiatrist to see an adolescent in an emergency room setting.
|
Suicidal behavior
|
|
|
adolescent patient with hematuria, red cell casts and an elevated creatinine. Next step in workup?
|
Think glomerulonephritis -> Poststreptococcal infection accounts for 50% of all cases of pediatric hematuria.
GET Antistreptolysin O (ASO) titer |
|
|
Normal ABG values for pH PaCO2, PaO2, HCO3, O2 sat?
|
7.4, 40, 90, 24, 98
|
|
|
acid base distrubance: low pH, low PaCO2, low HCO3
|
Metabolic acidosis where losing bicarb and gaining H+. Compensate by increasing ventillation
|
|
|
acid base distrubance: low pH, high PaCO2, high HCO3
|
respiratory acidosis due to hypoventillation. Bicarb is generated to compensate
|
|
|
acid base distrubance: high pH, high PaCO2, high HCO3
|
metabolic acidosis where lose H+ /gain bicarb and decrease ventillation to compensate
|
|
|
acid base distrubance: high pH, low PaCO2, low HCO3
|
respiratory alkalosis due to hyperventillation where bicarb is consumed to compensate
|
|
|
due pt w/ endocarditis need to restrict activity?
|
not usually
|
|
|
who gets prophylactic antibiotics when going to the dentist?
|
1. previous history of endocarditis,
2. prosthetic valve or material for repair, 3. heart transplant patients, and 4. severe or partially repaired congenital heart defects. |
|
|
3-day history of malaise, fever to 41.1°C (106°F), cough, coryza, and conjunctivitis. He then develops the erythematous, maculopapular rash w/ . He is noted to have white pinpoint lesions on a bright red buccal mucosa in the area opposite his lower molars. DX? Bug?
|
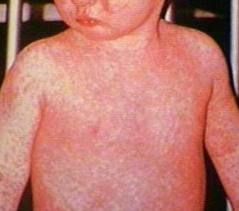
measles (rubeola)
|
|
|
>2 y/o congenital cyanosis. What is the most likely congenital cardiac anomaly?
|
Tetralogy of Fallot
|
|
|
Addison disease electrolyte abnormalities
|
hypOchloremia and hypERkalemia
Addison disease - deficiency of glucocorticoids and mineralocorticoids. Resorption of sodium and excretion of potassium and hydrogen ions are impaired at the level of the distal renal tubules. Sodium loss results in loss of water and depletion of blood volume. Persons with compensated Addison disease can have relatively normal physical and laboratory findings; Addisonian crisis, however, characteristically produces hyponatremia, hyperkalemia, and shock. The pathophysiology of the serum electrolyte abnormalities in this disorder is the same as in the salt-losing variety of adrenogenital syndrome. |
|
|
adolescent w/ unpredictable menstrual periods w/ no other clues. most likely cause?
|
Anovulatory bleeding is caused by continuous unopposed endometrial estrogen stimulation. Since these patients do not ovulate, progesterone from the corpus luteum is not secreted, the withdrawal from which would normally cause endometrial sloughing. It is the most common cause of dysfunctional uterine bleeding in women younger than 20 years of age, accounting for about 95% of cases. When women are within 2 years of menarche, this is especially common, and can be followed expectantly. Alternatively, oral contraceptives can be used to regulate periods.
|
|
|
> 30 days old w/ numbness and tingling possibly followed by seizures. Dx? Calcium? Phosphate?
|
hypocalcemia and hyperphosphatemia.
Hypoparathyroidism -> low concentrations of parathyroid hormone -> 1. reduced bone resorption. 2. reduced excretion of phosphate 3. reduced formation of 1,25-dihydroxy-vitamin D ->a) reduces the absorption of calcium b) reduces the absorption of phosphorus from the gut. |
|
|
kid w/ limp and has limited mobility of the hip, but denies pain and fever
|
Legg-Calvé-Perthes disease
avascular necrosis |
|
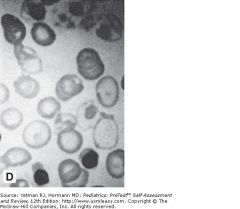
presents in the second 6 months of life with severe anemia requiring transfusion, heart failure, hepatosplenomegaly, and weakness. DX? Picture?
|
A target cell is an erythrocyte with a membrane that is too large for its hemoglobin content; a thin rim of hemoglobin at the cell's periphery and a small disk in the center give the cell a target-like appearance. Target cells, which are more resistant to osmotic fragility than are other erythrocytes,
DDX:1. -thalassemia, 2. hemoglobin C disease, or 3. liver disease (eg, obstructive jaundice or cirrhosis). Thalassemia major (slide D) presents in the second 6 months of life with severe anemia requiring transfusion, heart failure, hepatosplenomegaly, and weakness. Later, the typical facial deformities (maxillary hyperplasia and malocclusion) can be seen in a patient inadequately transfused. The diagnosis can be made on peripheral blood smear by the presence of poorly hemoglobinized normoblasts in addition to target cells in the peripheral blood. |
|
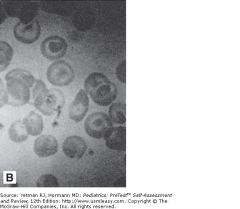
moderately severe hemolytic anemia, reticulocytosis, and splenomegaly and this on smear
|
hemoglobin C disease is frequently a mild disorder, target cells constitute a far greater percentage of total RBCs than in thalassemia major.
In the heterozygous state, no anemia or disease is noted, but target cells are seen. homozygous state, a moderately severe hemolytic anemia, reticulocytosis, and splenomegaly are seen, along with a smear containing a large number of target cells. |
|
|
nocturnal enuresis in 5 y/o? 6 y/o? inherited?
|
25% of 5-year-olds are enuretic. 10% of 6 y/o
Inherited: If one parent was enuretic, there is a 40% likelihood that the child will be. If both parents were bed wetters, there is a 70% risk that the child will be. |
|
|
T/F: nocturnal enuresis is due to deep sleep?
|
F
|
|
|
Congenital hydrocephalus may develop as a consequence of what first-trimester maternal disorders?
|
A maternal infection with mumps or rubella virus may produce aqueductal stenosis and, as a consequence, hydrocephalus. The aqueduct of Sylvius connects the third ventricle to the fourth ventricle. The lateral and third ventricles enlarge as the choroid plexus produces fluid that cannot migrate to the subarachnoid space to be reabsorbed.
|
|
|
Cause of an An infant who gags and chokes while feeding? Dx test?
|
uncoordinated suck-swallow reflex, or
may have significant gastroesophageal reflux. More rarely there may be an H-type tracheoesophageal fistula. A modified barium swallow with fluoroscopy allows direct visualization of the swallow reflex. |
|
|
arching of the back temporally related to feeds but has no emesis. Dx? test?
|
gastroesophageal reflux, causing Sandifer syndrome, a condition in which infants will arch and become tonic to protect their airway from the refluxing gastric contents.
esophageal pH probepreferred diagnostic test. |