Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
68 Cards in this Set
- Front
- Back

|
change in pigmentation is increased pigment secretion NOT increased # of melanocytes
freckles = appear after sun exposure |
|
|
lentigo
|
does NOT darken with sun; involves increased # of melanocytes
|
|
|
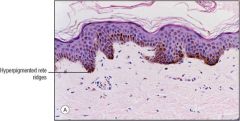
congenital nevus
|
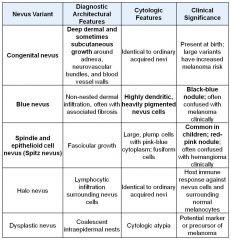
grows deep; variant of melanocytic nevus but goes deep
|
|
|
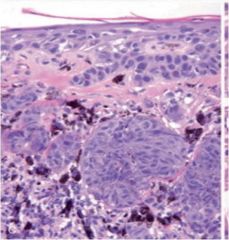
blue nevus
|
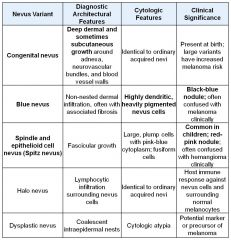
highly dendritic, very pigmented, black/blue
|
|
|
spindle and epitheliod cell envus
|
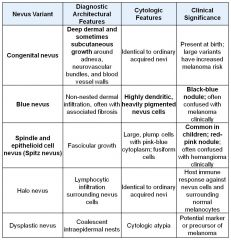
variant of melanocytic nevus
|
|
|
junctional nevi
|
nest of melanocytes; nuclei are uniform and round (non malignant)
grow into underlying dermis, become compound nevus (pieces at different layers) initially nevus cells = round, oval, nests -> as they migrate down they get smaller, dont produce as much pigment, become more fusiform/spindly = normal maturation in malignancy they will retain their size as they go down |
|
|
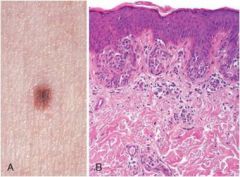
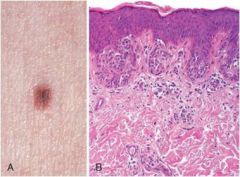
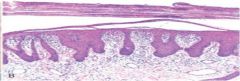
Melanocytic Nevus, junctional type.
Note the small, flat, symmetric, and uniform lesion. Note the rounded nests of nevus cells at the tips of the rete ridges along the dermoepidermal junction |
|
|
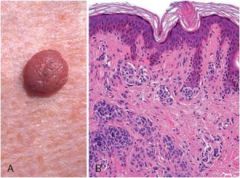
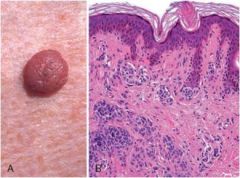
compound nevus; cells have moved from junction
Melanocytic Nevus, compound type. Note the raised lesion. It is symmetric with uniform pigment distribution. This lesion combines features of junctional nevi with nests and cords of nevus cells in the underlying dermis |
|
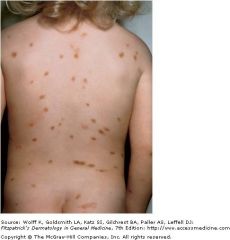
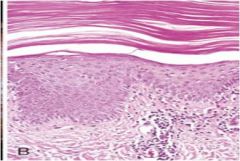
dysplastic nevi; do not progress; all over the place
|
larger than most acquired nevi; can be raised o flat; variability in pigmentation; in both sun exposed and nonsunexposed regions; w dysplastic nevus syndrome get lots and lots of lesions
|
|

|

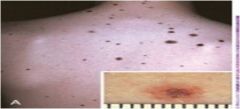
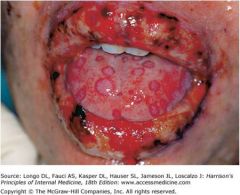
melanoma
Most melanomas arise in the skin Other sites include Oral and anogenital mucosal surfaces Esophagus Meninges Eye acbd = asymmetric, irregular borders, variegated color, diameter (anything greater than 6mm is suspicious) red flags = change in appearance, diameter greater than 6 mm, new onset itching or pain |
|
|
significance 2 growth phases of melanoma
|
radial vs vertical growth phase
vertical growth phase goes deep = higher chance of metastases; as you go deep might get a nodule clinically; cells are not breaking up as they're going deep; |
|
|
melanoma presdisposing factors
|
inherited genes; sun exposure
upper back in men; back and legs in women; lightly pigmented are at greater risk |
|
|
lentigo maligna melanoma
|
melanoma variant; linear hyperplasia; melanocytes combine w epidermis and when it invades it becomes melanoma
tends to occur on face in older pt |
|
|
mc type of melanoma
|
superficial spreading melanoma; nests form at junction and it spreads out radially
|
|
|
acral-lentiginous melanoma
|
arises on palmer, plantar, and subungal skin
more common in blacks subungal = under toenail |
|
|
benign epithelial tumors
|
derived from keratinizing epithelium of epidermis and hair follicles and ductular epithelium of cutaneous glands
|
|

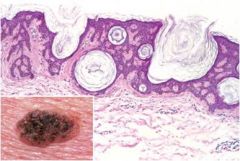
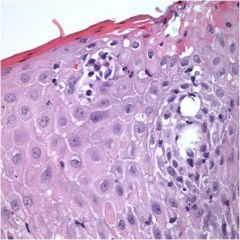
seborrheic keratoses
|
round/oval and tandem dark brow; appear to be stuck on; have a waxy velvety appearance to them;
|
|
|
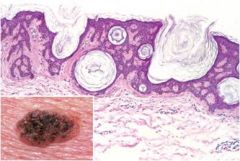
keratin pores; big keratin cysts which open to surface + proliferation of basaloid cells
|
|

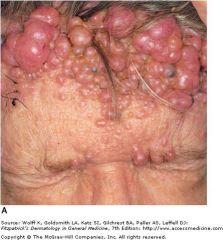
acanthosis nigricans
|
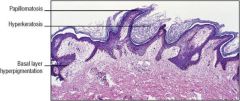
note papillomatosis on histo slide; this spires; hyerkeratosis = excess keratin
Thick, velvety, hyperpigmented skin Common sites include flexural areas such as axillae, skin folds of neck, groin, and anogenital regions ASSOCIATION with obesity or endocrine disorders in an older person GI ADENOCARCINOMA association |
|

fibroepithelial polyp
|
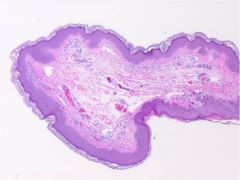
fibrovascular cores covered w squamous epithelium
note vessels and fiber deposition = fibrovascular; common benign disorder |
|
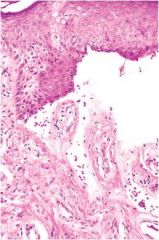
cysts of epidermal origin
|
cysts filled w keratin bc invaignation and cystic expansion of epidermis or hair follicle
dermoid cyst = epidermal inclusion cyst + appendages (hair collicles) = more complex than epidermal cyst; note keratin debri accumulation within the cyst; if it breaks open itll gonna be inflammatory |
|
|
appendage tumor
|
|

|

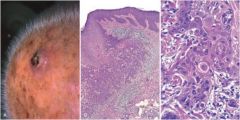
actinic keratosis; looks like a cigarette; cutaneous horn = scale formation
|
|
|
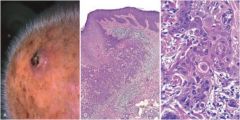
squamous cell carcinoma; bleeding nodule - far beyond actinic keratosis; middle slide shows tongues of squamous epithelium breaching basement membrane = inflammatory response. C: abnormal cells w enlarged nuclei w angulated contours and prominent nucleoli
|
|
|
2nd mc type of skin cancer
|
squamous cell carcinoma
non-healing lesion on skin prognosis for small lesions that are treated early is excellent |
|
|
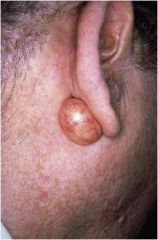
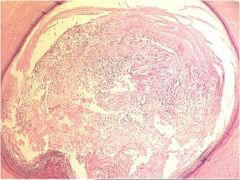
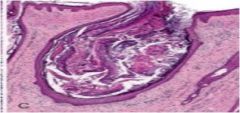
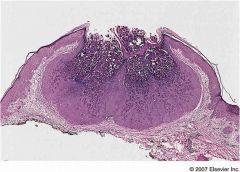
keratoacanthoma
|

RAPID GROWTH then spontaneously regresses
cup shaped lesion w keratin filled crater |
|
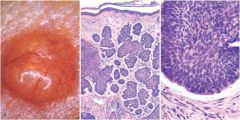
basal cell carcinoma
|
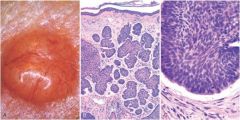
mc form of skin cancer; sun exposed regions in lightly pigmented individuals
rolled border pearly lesion; neoplastic cells look like basal cell layer (basophilic hyperchromatic layer) blood vessels growing over surface; basaloid cells (blue high nuclear density); peripheral palisating (cells lining up along the edge in order); cancer pulls away from stroma |
|

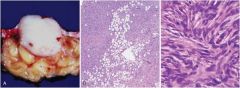
dermatofibrom
|

occurs on LEGS; benign proliferation of fibroblasts and histiocytes;
pseudoepithelium hyperplasia along the edge; |
|
|
"pinwheel pattern"
|
|
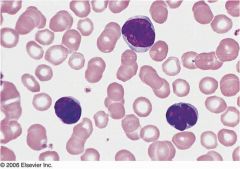
sezary lutzner cell
|
cell clusters known as Pautrier microabscess; link to mycosis fungoides; look like a BRAIN (hyperconvulated or cerebriform)
|
|

|
mycosis fungoides; usually involves truncal areas; can go systemic
|
|
|

Urticaria pigmentosa; cutaneous forms in children
|
|

ichthyosis (etymologically related to the word fish)
|
impaired epidermal maturation; chronic and exceessive accumulation and keratin
|
|

|
utricaria; mast cells release histamine; wheals/itching
IgE dependent; most cases; IgE independent: indirect activation of mast cells = opiates, antibiotics, radiographic contrast media complement mediated (inherited deficiency of C1 inhibitor) |
|

ezcema;
|

nonspecific inflammatory reaction; red papulovesciular lesions that can ooze and become crusted; when scratching you can get a superinfection
|
|
erythema multiforme
|
acute inflammatory disease: sign of something else; multiforme = all kinds of different lesions;
target lesions epithelial cells destroyed by Cd8+ CTL |
|
steven johnson syndrome
|
skin starts to slough off; skin lesions resemble erythema multiforme but more generalized
|
|
|
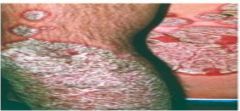
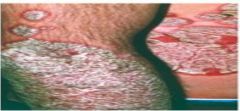
Psoriasis; associated with autoimmune dz; may be associated with
Arthritis Myopathy Enteropathy Spondylitic joint disease AIDS Most frequently affects the following sites Elbows Knees Scalp Lumbosacral area Intergluteal cleft Glans penis salmon colored plaquescovered by a loose silver/white scale nail change seen in 30%' pitting/dimpling of nail Koebner phenomenon; local trauma can induce lesions in susceptible individuals |
|
Acanthosis
|
Psoriasis; large tongues dip down
munro microabscessses; aggregates of neutrophils within the parakeratotic stratum corneum |
|
seborrheic dermatitis;
|
involves areas w high density of sweat glands; scaling and crusting; dandruff is commmon clinical manifestation; cradle cap in infants
often in HIV |
|

lichen planus
|
wickman striae; lacy white dots or lines on top of papules; recurrent, pruiritic inflammatory disorder
LICHEN PLANUS = flat topped, pink-purple, polygonal papule. interface dermatits; inflammatory cells affecting base of skin |
|
|
jig saw mophology of lichen planus
|
saw toothed ridge
|
|
|
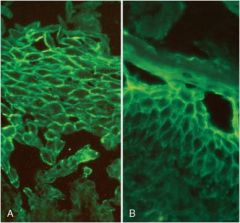
pemphigus
|
group of blistering disorders due to autoantibodies that result in the dissolution of the intercellular attachments within the epidermis and mucosal epithelium
|
|
|
nikolsky's sign
|
lateral pressure on skin that is adjacent to blister causes epideral detachment; w/o tx course is often fatal
|
|

pemphis vulgaris
|

autoimune against desmosomes (desmoglein 3); 80% of pemphigus; always
Scalp Face Axilla Groin Trunk Pressure points lesions = superifical easily rupted blisteres that leave shallow, crusted erosiosn; uniformly fatal if untreated (acantholysis = lysis of the intercellular adhesions connecting squamous epithelial cells) = selectively involves the cells directly above the basal cell layer |
|

pemphis foliaceus
|
BRAZIL; same as vulgaris but benign; note how these superficial blisters are less erosive than that of pemphis vulgaris; selectively involves the epidermis at the layer of hte STRATUM GRANULOSUM (acantholysis = lysis of the intercellular adhesions connecting squamous epithelial cells)
|
|
|
Retiular fishnet pattern due to deposition of IgG autoantibodies against desmogleins alon gthe plasma embrane o fthe epidermal keratinocytes; HLA linkage
|
|
|
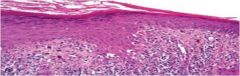
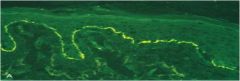
Bullous pemphigoid; elderly individuals; Ab against hemidesmosomes on basal membrane; antibodies cause injury by secondary complement activation and granulocyte recruiement
development of subepidermal cleft associated w basal cell dstruction |
|

|
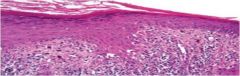
Bullous pemphigoid; elderly individuals; Ab against hemidesmosomes on basal membrane; antibodies cause injury by secondary complement activation and granulocyte recruiement
development of subepidermal cleft associated w basal cell dstruction DIFFICULT TO RUPTURE compraed to pemphigus vulgaris |
|
|
Antibody involved in dermatitis herptiformis
|
IgA ab to dietary gluten; cross rx w reticulin; injury inflammation = subepidermal blister
|
|
|
dermatitis herpatiformis
|
IgA ab to dietary gluten; cross rx w reticulin; injury inflammation = subepidermal blister
|
|

|

dermatitis herptiformis; IgA ab to dietary gluten; cross rx w reticulin; injury inflammation = subepidermal blister;
microabscesses develop at the tips of dermal papillae forming subepidermal blisters; note accumulation of neutrophils (microabscesses) at the tips of dermal papillae |
|

bilateral, symmetric, grouped lesions on extensor surfaces in a pt w malabsorption syndrome
|
dermatitis herpetiformis
|
|

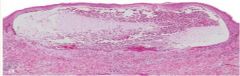
epidermolysis bullosa
|
inherited structural protein defects compromising mechanical skin stability; blisters develop at site sof pressure, rubbing or trauma; NONINFLAMMATORY subepidermal blister
|
|

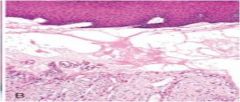
Utricaria and vesicles exacerbated by sun exposure and heal without scarring
|
porphyria; disorders of porphyrin metabolism; deposition of glycoproteins in and around the upper dermal vessels the dermal papillae are rigid
|
|

|
inflammatory acne associated with erythematous papules and pustules; formation of comedones secondary to obstruction and inflammation of pilosebaceous units; in adolescents = hormonal and alterations of hair folicles
exacerbated by drugs, occupational contacts, heavy clothing, coismetics, tropical environments |
|
|
four factors of acne pathogenesis
|
Follicular hyperkeratinization
Increased sebum production Propionibacterium acnes (P. acnes) within the follicle Inflammation note open comedon |
|
|
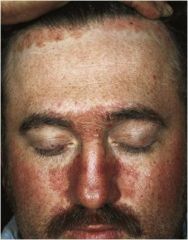
rosacea
|
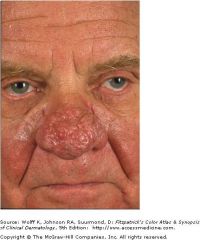
chronic inflammatory disorder (facial flushing, teleangiesctasia, erythema, papules, pustules)
rhinophyma in severe cases (large red bulbous nose) perifollicular infiltrate composed of lymphocytes surrounded by dermal edema |
|

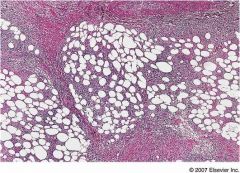
erythema nodosum
|
form of panniculitis (subcut fat inflammation); inflammation fo connective tissue septa = edema, fibrin exudation, neutrophilic infiltration, other inflammatory mediators such as multinucleated giant cells
|
|
|
erythema induratum
|
form of panniculitis (subcut fat inflammation); affects vasculitis of vessels supplying subcutaneous fat = inflammation/necrosis of adipose tissue; erythematous and tender nodule that generally will eventually ulcerate
|
|
|
weber-christian disease
|
panniculitis; foci of inflammation with foamy histiocytes, lymphocytes, neutrophils and giant cells; (relapsing febrile nodular panniculitis)
|
|

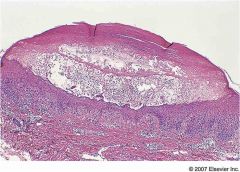
molluscum contagiosum
|
poxvirus; cuplike verrucous epidermal hyerplasia
|
|
|
impetigo
|
superficial skin infection with crusting or bullae caused by streptococci or staphylococci;
children note subcorneal blister w inflammatory cells |
|
|
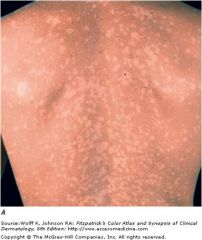
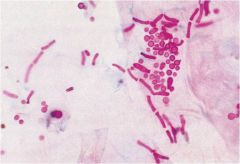
tinea versicoloar secondary to superifical fungal infection by malassezia furfur
hypopigmented or hyperpigmented mascules; common sites include upper trunk, arms, chest, shoulders, face and neck |
|

|
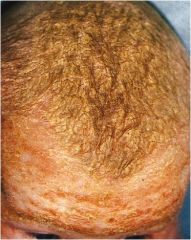
tinea barbae; dematophyte infection of the beard area; kerion can occur resulting in hair loss due to scarring
|
|

tinea capitis
|
scalp ringworm; dermatophyte infection of scalp; gradual appearance of round patches of dry scale and or alopecia; kerion may occur due to inflammatory scalp mass;
|
|

|
tinea corporis; body ringworm
dermatophyte infection of the body surface; pink to red annular patches and plaques with raised scaly borders that expand peripherally; proclivity for clearing of the center of lesion |
|

tinea unguium
|
Onychomycosis; nails are thickened, discolored and brittle
|