Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
57 Cards in this Set
- Front
- Back
|
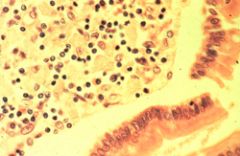
Whipples dx; foamy macrophages in the lamina propria of the small bowel
|
|
|
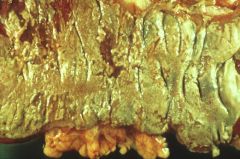
Pseudomembranous colitis due to clostridium difficile
|
|
|
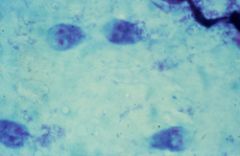
Giardia trophozoites. The organism is a flagellated protozoan that produces diarrhea, cramps, flatulence, and malabsorption by infecting the small intestine
|
|
|
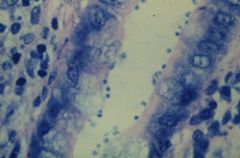
Cryptosporidiosis
Note the blue staining oocysts. They are acid-fast |
|
|
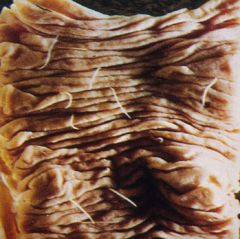
Necator (hookworm) infestation of the bowel
Note the worms attached to the surface of the mucosa. Iron deficiency is a complication |
|

|
Ascariasis of bowel
Note the conglomeration of worms that obstructed the bowel lumen. |
|
|
Strongyloidiasis; Note the adult worms embedded in the bowel mucosa
|
|

|
Enterobiasis (pinworm)
Note the characteristic embryonated egg with a flat side. |
|
|
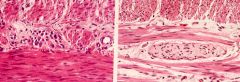
Hirschsprung's disease
The frame on your left depicts ganglion cells and the one on your right the absence of ganglion cells in the rectosigmoid. |
|

|
Volvulus
Note how the colon is twisted around the mesentery. |
|
|
Schematic of intussusception
Note how the terminal ileum has intussuscepted into the cecum. |
|

|
Intussusception
The sausage shaped mass in the lumen of the cecum is the terminal ileum |
|

|
Crohn's disease
This slide shows a gross specimen of Crohn's disease demonstrating fissuring, serpiginous ulcers and cobblestone mucosa |
|

|
Crohn's disease
This slide demonstrates cobblestone change in the mucosa of the colon. |
|
|
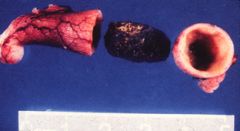
Crohn's disease
Note the thickened terminal ileum emptying into the cecum. The lumen is extremely narrow and would show up as a string sign on a barium enema. |
|

|
Ulcerative colitis
Note the islands of red, inflamed mucosa representing pseudopolyps and the gray-yellow ulcerated mucosa |
|
|
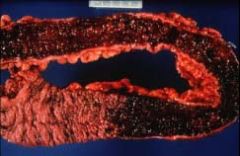
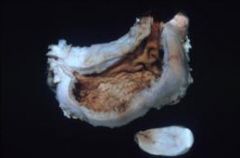
Ulcerative colitis
This slide is a gross specimen from a case of UC. Note the hemorrhagic ulcerated appearance of the mucosa and the continuous involvement without skip areas. |
|

|
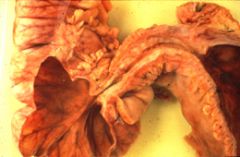
Infarcted small bowel
note the localized hemorrhagic infarction of the small bowel. It may have been entrapped in the external inguinal canal of an indirect inguinal hernia. |
|

|
Diverticulosis
This gross specimen demonstrates the development of diverticuli where the artery penetrates the muscular wall of the colon. |
|

|
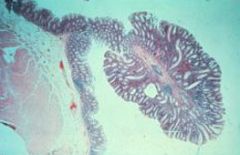
Diverticulosis
This slide is a microscopic section of a diverticulum in the colon. Note that the wall of the diverticulum does no contain all layers of the colon wall, which makes it a false diverticulum. |
|

|
Barium enema with diverticulosis
Note the numerous outpouchings. |
|

|
Familial polyposis
This autosomal dominant condition is associated with multiple tubular adenomas and tubulovillous tumors in the colon. The patient has greater than 100 polyps and is at risk for colon cancer. There is an association with the APC tumor suppressor gene. |
|

|
Hyperplastic polyps
This slide also shows multiple hyperplastic polyps, most being sessile (without a stalk). |
|

|
Ischemic stricture at splenic flexure
Note the thick wall of the bowel and narrow lumen from repeated small infarcts with repair by fibrosis. |
|
|
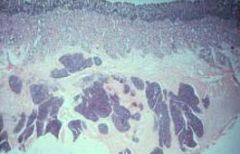
Tubular adenoma
This is a microscopic section of a neoplastic polyp arising from the colon mucosa. The polyp is pedunculated and is composed of colonic glands which have lost many of the normal goblet cells. This is called an adenomatous change. |
|

|
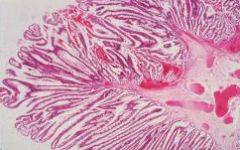
Villous adenoma
This slide demonstrates the velvety appearance of a villous adenoma of the colon. |
|
|
Villous adenoma
This is a microscopic section of a villous adenoma. Note the long stalk-like papillary projections of the tumor. These tumors are typically sessile and have a high incidence of malignant transformation |
|

|
Adenocarcinoma of colon
This tumor is a fungating mass with central necrosis which arises from colonic mucosa. It tends to infiltrate the wall of the colon in a "napkin-ring" fashion producing obstruction. Obstructive lesions occur in the descending colon. |
|

|
Adenocarcinoma of the colon
This lesion is growing as a polypoid mass into the lumen of the ascending colon. Right sided colonic masses typically present with anemia and bleeding. |
|
|
Acute appendicitis with fecalith
Fecaliths are more commonly associated with adult rather than childhood appendicitis, which is more often secondary to a viral infection (measles, adenovirus). |
|
|
Choristoma (heterotropic pancreas)
This is a section of duodenum showing an aggregate of pancreatic tissue in the wall. The pancreatic tissue is normal in appearance but in an abnormal location. This is a non-neoplastic process. |
|

|
Peutz-Jeghers
This is a syndrome associated with mucocutaneous pigmentation and hamartomatous polyps of the GI tract. |
|
|
Barrett's esophagus-mucin stain
This is a metaplastic change in the esophagus associated with reflux esophagitis. The normal squamous esophageal mucosa is replaced by gastric glandular mucosa. It is a precursor lesion for adenocarcinoma of the esophagus. |
|

|
Squamous cell carcinoma of the larynx
Note the fungating mass on the lateral border of the larynx with central ulceration. These tumors are associated with smoking and chronic alcohol use. The first symptom is hoarseness |
|

|
Squamous cell carcinoma of esophagus
This tumor typically arises in the middle third of the esophagus and infiltrates the wall. The most common symptom is dysphagia, first for solids and then both liquids and solids. |
|

|
Squamous cell carcinoma of esophagus
This tumor has invaded the walls of local structures around the esophagus and infiltrates the wall. The most common symptom is dyphagia, first for solids and then both liquids and solids. |
|
|
Linitis plastica (adenocarcinoma of the stomach (signet ring carcinoma)
This tumor invades the wall of the stomach producing a desmoplastic response. The stomach becomes hard like a leather bottle. This tumor presents late in its course and has a tendency to metastasize to the ovaries |
|
|
Carcinoid tumor of the appendix
This is the most common location of an asymptomatic carcinoid tumor. The tumor arises in the tail of the appendix from resident neuroendocrine cells (APUD cells). It is usually an incidental finding in this location. |
|

|
Tubular adenoma
There are four slide demonstrating a tubular adenoma. The slide on the upper left is a endoscopic view of the pedunculated tumor. A barium outlines the polyp. The last two slides show the pedunculated polyp. There is a slight risk of malignant transformation with tubular adenomas |
|
|
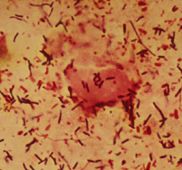
ram positive rods in stool- Clostridium difficile:
This organism is part of the normal flora of stool. However, when antibiotics are administered (e.g., ampicillin, clindamycin) bacteria that normally keep C. difficile in check are destroyed allowing for rapid proliferation and the potential for pseudomembranous colitis |
|
|
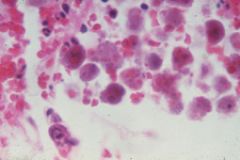
Entameba histolytica trophozoites with erythrophagocytosis and necrotic debris from ulcer in the cecum:
The red dots in the trophozoites represent RBCs |
|
|
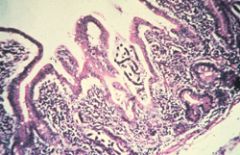
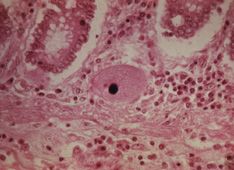
Flask shaped ulcer in cecum due to Entameba histolytica:
In the middle of the biopsy, there is defect in the mucosa and a stream of inflammatory cells extending out into the lumen of the bowel (bottom of the slide) and into the submucosa. Organisms are not visible at this magnification. |
|
|
Cecal biopsy showing trophozoites of Entameba histolytica:
Note erythrophagocytosis |
|

|
Needle aspirate of liver abscess in a patient with amebiasis due to Entameba histolytica:
Note the brown discoloration of the aspirate fluid, which some have described as having an "anchovy paste" appearance |
|

|
CT of liver showing an abscess due to Entameba histolytica:
Trophozoites gain entry into the portal vein tributaries draining the cecum. Most abscesses are in the right lobe. Rx is metronidazole. |
|
|
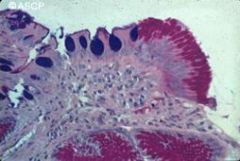
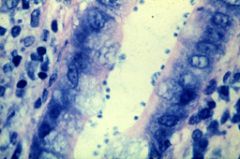
Small bowel biopsy showing Cryptosporidium parvum acid-fast oocysts in mucous layer:
Cryptosporidium is a sporozoan that is the MCC of diarrhea in patients with AIDS. It is a frequent contaminant of reservoirs and produces epidemics of diarrhea (e.g., Milwaukee). Entero-Test (string test) is positive. |
|
|
Colon biopsy demonstrating Balantidium coli:
Balantidium is a ciliate. It produces colonic ulcers leading to bloody diarrhea |
|
|
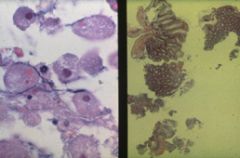
Leishmanial forms of Leishmania donovani complex (visceral leishmaniasis) phagocytosed by a macrophage:
In leishmaniasis, only the leishmanial form is present in disease. Phlebotomus (sandfly) is the vector for the disease. Visceral leishmaniasis is called kala azar and is characterized by massive splenomegaly and eosinophilia. Macrophages contain the leishmanial forms, which are very similar in appearance to the yeast forms of Histoplasma and the Donovan bodies in granuloma inguinale. |
|
|
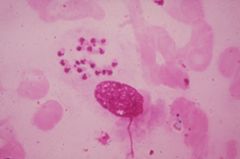
Scotch tape preparation taken from the perianal area showing egg of Enterobius vermicularis (pinworm, nematode):
Note the flat side to the embryonated egg. Anal pruritus is the key feature of the disease and is due to the adult worms laying eggs around the anus in the early morning hours. There is no eosinophilia, since it is non-invasive. Using two-sided tape and compressing it around the anus attaches to the eggs and allows for easy diagnosis under the microscope. Rx is albendazol |
|

|
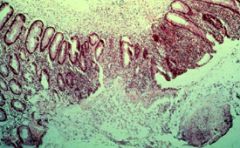
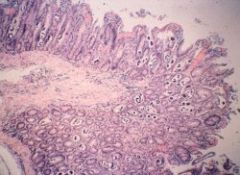
Bowel with Trichuris trichiura (nematode):
Trichuris trichiura is also called the whipworm. Note the organisms attached to the cecum. Patients experience diarrhea and children may develop rectal prolapse. Rx is albendazole. |
|
|
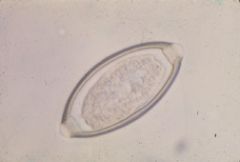
Egg of Trichuris trichiura:
Note the characteristic egg with a plug at both ends |
|

|
Child with passage of adult Ascaris lumbricoides worms (nematodes) and x-ray demonstrating location in the bowel:
Larval phase is in the lungs and produces cough, pneumonitis, and eosinophilia. Adults cause intestinal obstruction and are not invasive, hence no eosinophilia. |
|
|
Bowel with Strongyloides stercoralis (nematode):
Infective filariform larvae in the soil penetrate the skin and migrate to the lungs. They are swallowed and develop into adult worms which burrow into the wall of the bowel, where they mate and lay eggs which hatch rhabditiform larvae, which enter the lumen and are passed into feces. In soil, they molt and produce the infective filariform larvae. Autoinfection and superinfection (especially in AIDS) may occur. Positive Entero-Test (string test). Rx is ivermectin or albendazole |
|

|
Rhabditiform larva in stool preparation of Strongyloides stercoralis:
Note that this is the only worm that does not normally pass eggs in the stool |
|
|
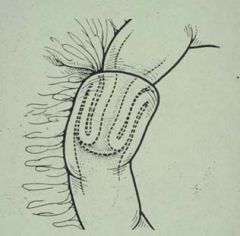
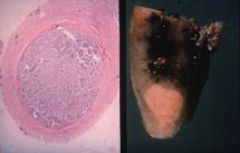
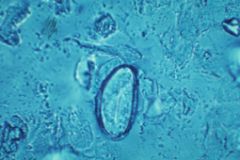
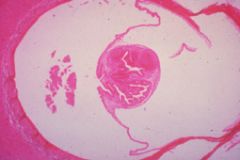
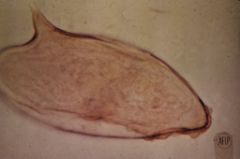
Scolex of Echinococcus granulosus (cestode):
Note the scolex, which has hooks for attachment if it ever developed into an adult, which it cannot do in man |
|
|
Schistosoma mansoni (trematode) egg:
Note the sharp lateral spine. Schistosomes have the following life cycle: egg (human)g ciliated miracidia larvaeg infect snails (1st intermediate host)g produce fork tailed cercaria larvaeg penetrate skin of humang produce disease |
|

|
Tongue of a patient with Candida albicans glossitis:
Note the white pseudomembrane covering the tongue. The patient was HIV positive. It is not AIDS-defining |