Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
381 Cards in this Set
- Front
- Back
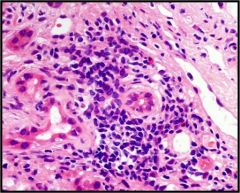
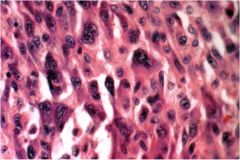
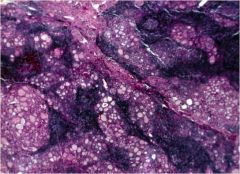
acute or chronic hepatitis?
|
acute hepatitis
|
|
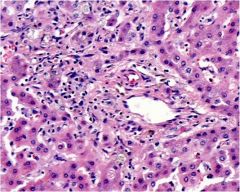
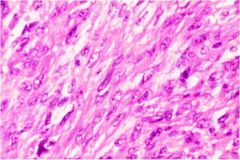
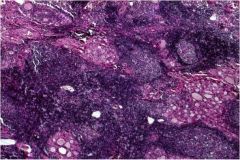
acute or chronic hepatitis?
|
acute hepatitis with Kupffer cell hypertrophy (stain is for Kupffer cells)
|
|
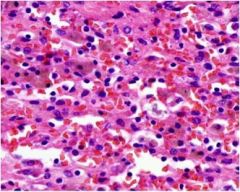
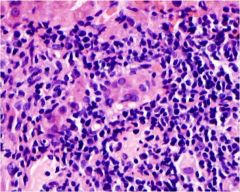
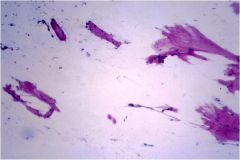
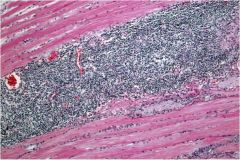
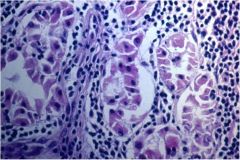
acute or chronic hepatitis?
|
acute hepatitis, mostly lymphocytes
|
|
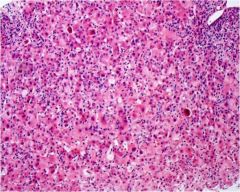
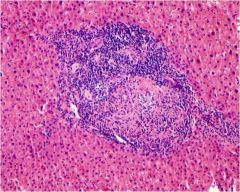
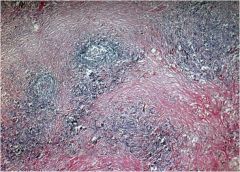
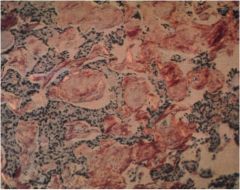
acute or chronic hepatitis?
|
acute, necrosis
|
|
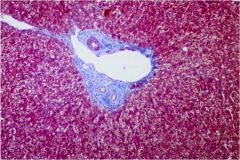
what is wrong with this liver?
|
cholestasis
|
|
acute or chronic hepatitis?
|
chronic hepatitis, bridging fibrosis
|
|
|
What is the histopathological difference between acute and chronic hepatitis?
|
Acute hepatitis = lobular inflammation. Chronic hepatitis = portal inflammation, spreading to lobules as it worsens. Acute will NOT have fibrosis; chronic might.
|
|
acute or chronic hepatitis?
|
chronic, with interface activity
|
|
acute or chronic hepatitis?
|
chronic, because there is periportal fibrosis
|
|
acute or chronic hepatitis?
|
chronic, portal inflammation
|
|
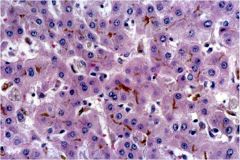
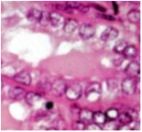
what feature of chronic hepatitis B is shown here?
|
ground glass hepatocytes
|
|
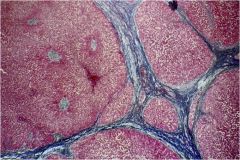
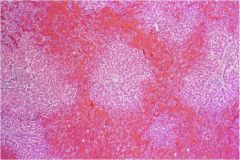
What pathological process is seen in this liver?
|
Cirrhosis = regenerative nodules + bridging fibrosis
|
|
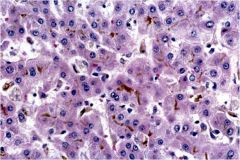
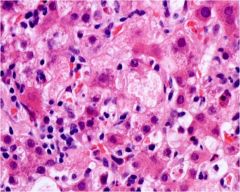
What type of cell death is occurring in this liver?
|
Apoptosis
|
|
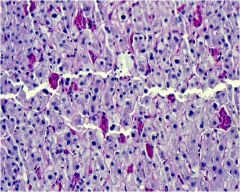
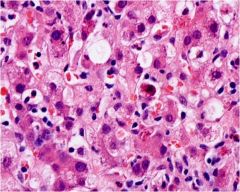
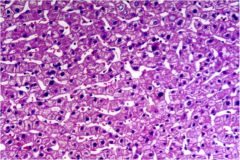
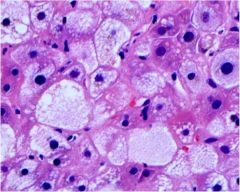
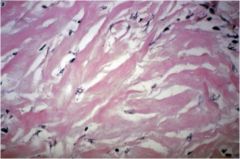
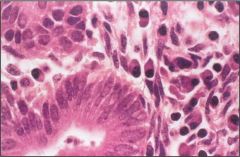
What feature of hepatocyte damage is seen in this picture?
|
ballooning degeneration
|
|
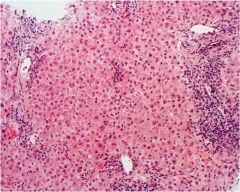
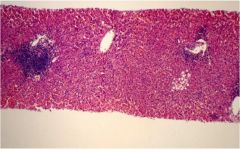
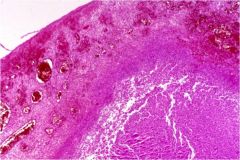
Which side of this liver is normal, and why?
|
RIGHT is normal because sheets of hepatocytes are 1 cell thick. LEFT is abnormal because there is disarray of the sheets, > 1 cell thick.
|
|
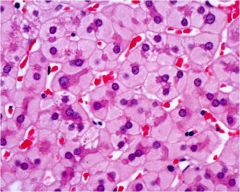
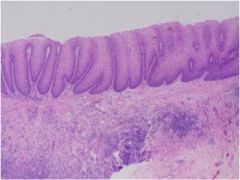
Normal or hepatitis?
|
Normal
|
|
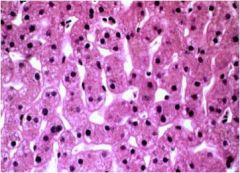
Normal or hepatitis?
|
Normal
|
|
What microarchitectural feature of the liver is seen at the center of the image?
|
Portal triad
|
|
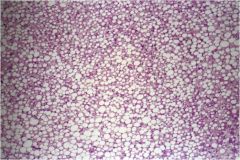
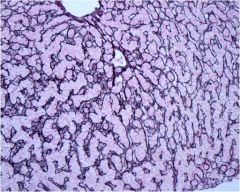
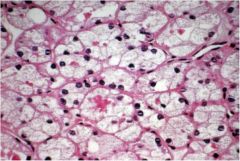
What pathological process has occurred in this liver?
|
steatosis
|
|
Describe the acinar scheme of liver histology. Which zone is congested in this image? What might have caused this damage?
|
Acinar scheme - metabolic segments centered on the blood supply, characterized by an enzymatic gradient. Zone 3. Acetominophen.
|
|
|
What is the main difference between primary biliary cirrhosis (PBC) and primary sclerosing cholangitis (PSC)?
|
PBC = microscopic cholangitis, PSC = macroscopic cholangitis. Both are autoimmune.
|
|
|
Which mostly co-occurs with ulcerative colitis: PBC or PSC?
|
PSC
|
|
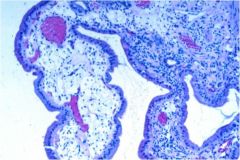
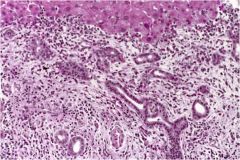
This is a section of cholecystitis. Is it acute or chronic?
|
Acute cholecystitis with congestion, hemorrhage, and purulent exudate (=neutrophils).
|
|

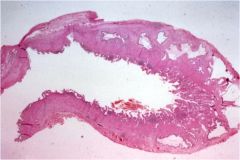
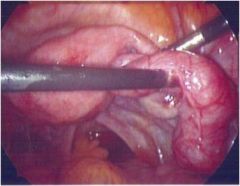
This is a gross specimen of a gallbladder. What is the diagnosis?
|
Acute cholecystitis (hemorrhagic, edematous instead of fibrotic)
|
|
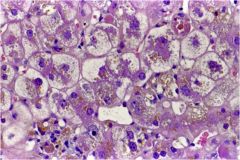
What pathologic process is occurring in this liver?
|
Canalicular cholestasis
|
|
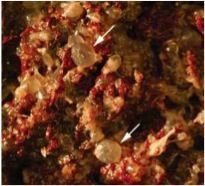
This is a section of gallbladder. Give the diagnosis and "buzzword."
|
Cholesterolosis, "strawberry gallbladder."
|
|
This is a section of cholecystitis. Is it acute or chronic?
|
Chronic
|
|

This is a gross specimen of the gallbladder. What is the diagnosis?
|
Cholesterolosis, "strawberry gallbladder"
|
|
Describe the pathologic process in this image of the liver.
|
intrahepatic cholestasis
|
|
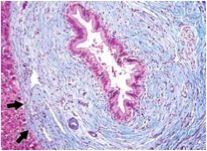
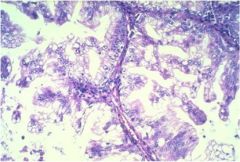
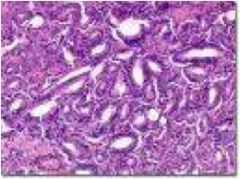
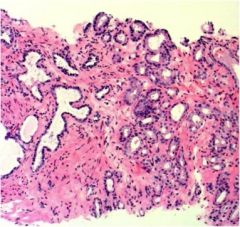
What is the diagnosis for this section of liver?
|
Primary biliary cirrhosis. Note atrophy of the bile duct and thickening of its basement membrane.
|
|
What is the diagnosis for this section of liver?
|
Primary biliary cirrhosis, bile duct loss (ductopenia)
|
|
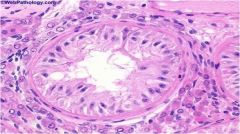
What is the diagnosis for this section of liver?
|
Primary biliary cirrhosis, small bile duct damage
|
|
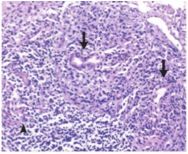
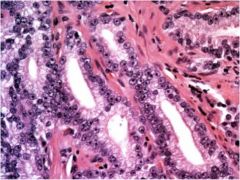
What is the diagnosis and what is the main histologic feature?
|
Primary biliary cirrhosis with periductal granuloma
|
|
This is a section of primary sclerosing cholangitis. What does the microscopic bile duct pathology imply?
|
Nonspecific findings for downstream obstruction, in this case due to PSC
|
|
What is the diagnosis?
|
Large bile duct inflammation, in this case due to primary sclerosing cholangitis.
|
|
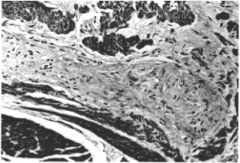
This is a section of primary sclerosing cholangitis. What pathologic process is occurring periductally?
|
Fibrosis
|
|
|
What is the difference between steatosis and steatohepatitis?
|
Steatosis is completely reversible, whereas steatohepatitis causes irreversible cell damage. Signs of this damage include ballooning degeneration, apoptosis, and fibrosis. Alcoholic steatohepatitis may have Mallory bodies.
|
|
|
What are Mallory bodies and with which liver condition are they associated?
|
Mallory bodies are cytoplasmic inclusions composed of cytokeratins, ubiquitins, and other proteins. They are seen in alcoholic steatohepatitis.
|
|
|
Is the inflammation and fibrosis in steatohepatitis primarily lobular or periportal?
|
Lobular
|
|
|
Microvesicular steatosis is rare. Name some conditions in which it occurs.
|
Reye syndrome, fatty liver of pregnancy, foamy degeneration, certain drugs, congenital mitochondrial cytopathies.
|
|
|
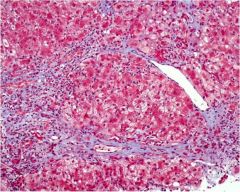
What are the causes of hepatocellular and Kupffer cell hemochromatosis, respectively?
|
Increased iron from any source --> hemochromatosis. Hepatocellular is from increased uptake, eg genetic hemochromatosis. Kupffer cell is from increased RBC breakdown, such as hemolytic anemia or blood transfusions.
|
|
|
True or false: Hepatocellular vs. Kupffer cell hemochromatosis becomes more distinct as the disease progresses.
|
FALSE. As hepatocytes die, the Kupffer cells clean up, and vice versa, making the diseases less distinguishable.
|
|
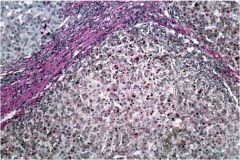
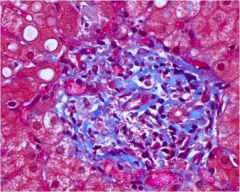
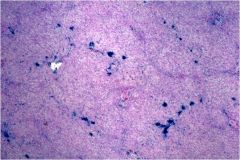
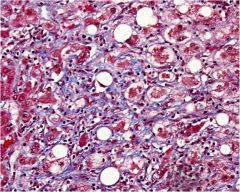
What general pathological process is occurring in this liver? What disease caused it?
|
Cirrhosis, alpha-1 antitrypsin deficiency
|
|
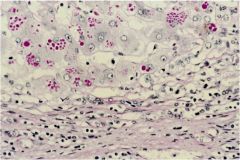
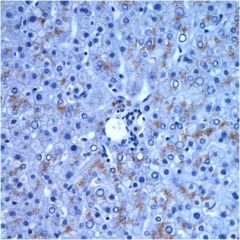
What disease is shown in this section of liver stained with diastase?
|
alpha-1 antitrypsin deficiency. The granules are clumps of accumulated defective enzyme.
|
|
|
What organ is most commonly affected by alpha-1 antitrypsin deficiency?
|
Lungs. Loss of inhibition of elastase --> emphysema.
|
|

Which pancreas is normal? What's wrong with the other one?
|
RIGHT is normal. LEFT has hemochromatosis
|
|
|
What organ is most commonly affected by alpha-1 antitrypsin deficiency?
|
Lungs. Loss of inhibition of elastase --> emphysema.
|
|
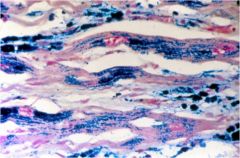
What is wrong with this cardiac tissue?
|
Iron accumulation due to hemochromatosis
|
|
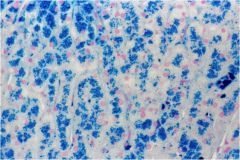
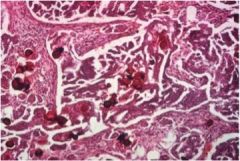
What type of hemochromatosis is seen in this image? What is the most common cause?
|
Hepatocellular hemochromatosis, MCC=genetic
|
|

Describe the sign seen here.
|
Kayser-Fleischer rings in Wilson's disease
|
|
What type of hemochromatosis is seen here? What are some of the causes?
|
Kupffer cell (secondary) hemochromatosis. Causes include hemolytic anemia and iron overload from blood transfusions.
|
|
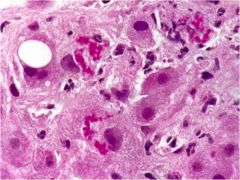
What is the pathologic process in this liver?
|
Alcoholic steatohepatitis with Mallory bodies
|
|
The liver condition shown is rare. Name the condition and its causes.
|
Microvesicular steatosis. Causes include Reye syndrome, fatty liver of pregnancy, and foamy degeneration.
|
|
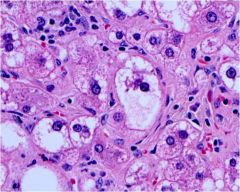
What pathologic process is seen in this liver?
|
Steatohepatitis with ballooning degeneration, cell lysis, and LOBULAR damage.
|
|
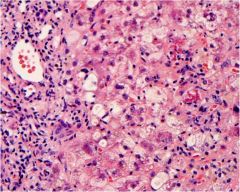
Name the condition seen in this liver.
|
Steatohepatitis with lobular fibrosis
|
|

Name the condition seen in this liver.
|
Steatohepatitis with lobular fibrosis.
|
|
Name the liver condition and the inclusions.
|
Mallory bodies indicate alcoholic steatohepatitis
|
|

What is wrong with this liver?
|
It's yellow and thus full of fat!
|
|
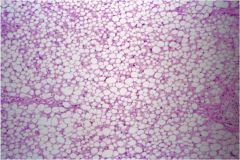
Is this steatosis or steatohepatitis?
|
Steatosis. No permanent cell damage.
|
|
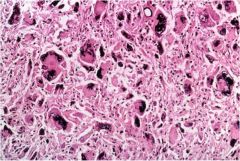
What metal is deposited in this liver?
|
Copper, Wilson's disease.
|
|

This is a pancreas. Acute or chronic pancreatitis?
|
Acute, it's hemorrhaging!
|
|
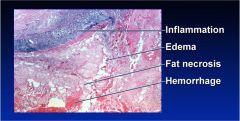
Acute or chronic pancreatitis?
|
Acute, hemorrhage & acute inflammation
|
|
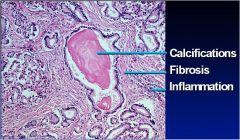
Acute or chronic pancreatitis?
|
Chronic - fibrosis, calcification, chronic inflammation
|
|
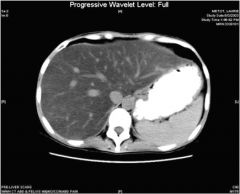
What's wrong with this picture?
|
Enlarged, fatty liver
|
|

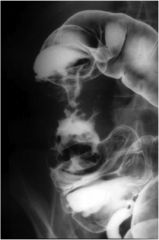
Does this barium study show ulcerative colitis or Crohn's disease? Why?
|
CD, cobblestoning
|
|

Does this colon show ulcerative colitis or Crohn's disease? Why?
|
CD, long linear ulcer, not pancolitis
|
|

Does this barium study show ulcerative colitis or Crohn's disease? Why?
|
CD, string sign from stricture
|
|
Ulcerative colitis or Crohn's disease? Why?
|
CD, granuloma
|
|

Skin findings in IBD.
|
YAY!
|
|

Is this colonoscopy normal?
|
Normal
|
|

Does this patient most likely have ulcerative colitis or Crohn's disease?
|
Ulcerative colitis. Primary sclerosing cholangitis - "string of beads"
|
|
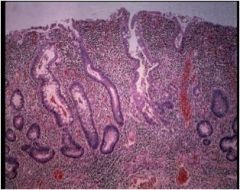
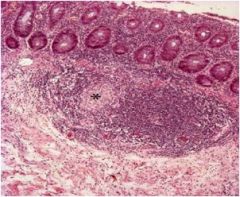
Does this segment of colon show ulcerative colitis, Crohn's disease, or neither?
|
Ulcerative colitis. Infiltration of the mucosa with inflammatory cells.
|
|

What is wrong with this colon - ulcerative colitis, Crohn's disease, or nothing?
|
UC, severe
|
|

What is wrong with this colon - ulcerative colitis, Crohn's disease, or nothing?
|
Ulcerative colitis, mild. Compared to a normal colonoscopy, it is inflamed and you cannot see any blood vessels
|
|

What is wrong with this colon - ulcerative colitis, Crohn's disease, or nothing?
|
Ulcerative colitis, moderate
|
|
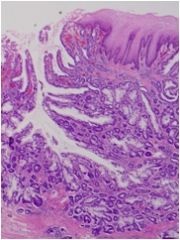
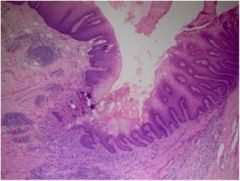
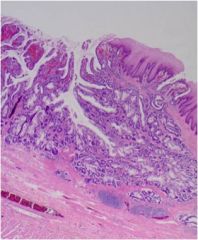
What is wrong with this section of esophagus?
|
Barrett's esophagus, defined as intestinal metaplasia with the presence of goblet cells
|
|

What is wrong with this esophagus on EGD?
|
Esophageal adenocarcinoma, which has progressed from Barrett's esophagus
|
|

What is wrong with this esophagus?
|
Esophageal adenocarcinoma
|
|
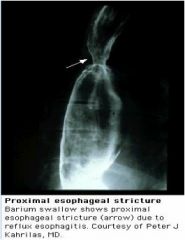
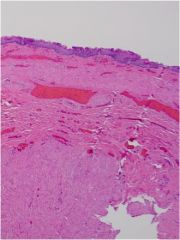
What has occurred in this esophagus, and why?
|
Esophageal stricture, most likely secondary to GERD --> esophagitis --> collagen deposition with healing
|
|
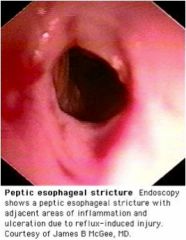
What abnormality is seen on this EGD?
|
Esophageal stricture, most likely secondary to GERD --> esophagitis --> collagen deposition --> stricture
|
|
What caused this esophageal abnormality?
|
Esophageal ulcers, most likely secondary to GERD
|
|
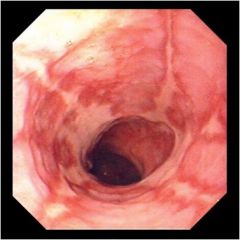
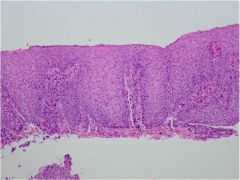
What is wrong with this esophagus as seen on EGD?
|
Esophagitis, most likely secondary to GERD
|
|

What is wrong with this esophagus?
|
Esophageal stricture, most likely secondary to GERD esophagitis --> collagen deposition
|
|
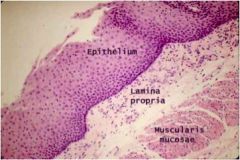
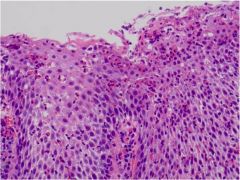
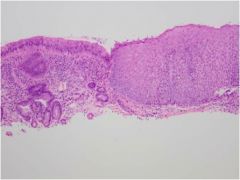
From what part of the GI tract is this healthy tissue?
|
Esophagus (squamous epithelium)
|
|

What is wrong with this colon?
|
Colorectal cancer
|
|
What abnormality is seen on this CT scan?
|
Rectosigmoid mass (colorectal cancer)
|
|

What abnormality is shown on this colonoscopy?
|
Familial adenomatous polyposis, >100 polyps in colon
|
|

What is wrong with this picture?
|
Acute anal fissure
|
|
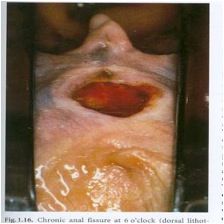
What is wrong with this picture?
|
Chronic anal fissure
|
|

What are these? Are they thrombosed?
|
Hemorrhoids, no, not thrombosed
|
|

What are these? Are they thrombosed?
|
Hemorrhoids, not thrombosed
|
|

What are these and what causes them?
|
Condyloma acuminata, HPV infection
|
|

What is the lesion and what causes it?
|
Condyloma acumulata, HPV infection
|
|

What is this?
|
Perianal abscess
|
|

What is this and what causes it?
|
Squamous cell carcinoma of the anus, HPV infection
|
|

What is this and what causes it?
|
Squamous cell carcinoma of the anus, HPV infection
|
|

What is this?
|
A thrombosed external hemorrhoid
|
|

What is this?
|
A thrombosed external hemorrhoid
|
|

Which artery is angiographed here, and what does it show?
|
Inferior mesenteric artery (note how it's left colon) showing diverticular bleed
|
|

What does this barium enema show?
|
Diverticulosis
|
|
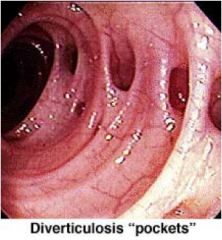
What does this colonoscopy show, and what 2 conditions is this person predisposed to?
|
Diverticulosis, prone to diverticular bleeding and diverticulitis
|
|

What does this CT show and what is the diagnosis?
|
Pneumatosis intestinalis (air in the intestinal wall) from perforated diverticulitis
|
|

What is the most likely cause of this infant's dilated colon?
|
Hirschprung's disease, failure of migration of neural crest cells to ganglia in colonic myenteric, submucosal plexuses
|
|

Name the pathology in this colon.
|
Pseudomembranous colitis from C. difficile
|
|

What diagnostic test has been performed in this patient, and what does it show?
|
Sitzmark capsule transit test demonstrating slow intestinal transit (>5 beads)
|
|
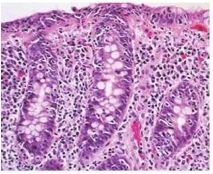
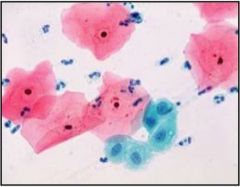
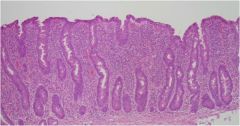
What does this gastric biopsy show?
|
H. pylori
|
|

What is the defect in this disease?
|
Autosomal recessive defect in MTTP, which encodes microsomal triglyceride transfer protein. MTTP is a component of B-lipoproteins, which are necessary for the absorption of fat.
|
|

Diagnosis?
|
Abetalipoproteinemia
|
|
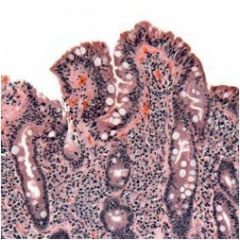
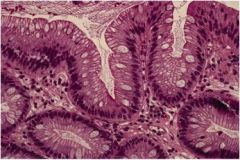
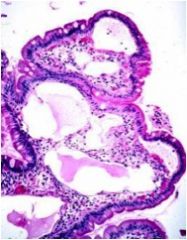
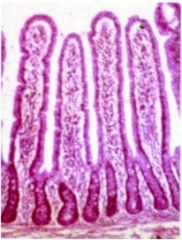
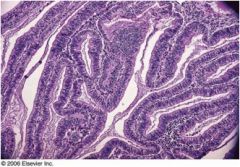
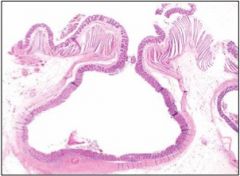
What is wrong with this small bowel biopsy specimen?
|
Celiac disease
|
|
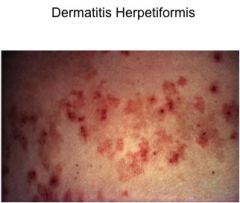
What is this, and which intestinal disease is it associated with?
|
Dermatitis herpetiformis, Celiac disease
|
|
What is wrong with this small bowel? What is the #1 absorptive deficit?
|
Lymphangectasia, trouble absorbing fat
|
|
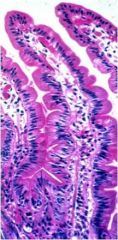
What is wrong with this small intestine?
|
Nothing, it's normal
|
|
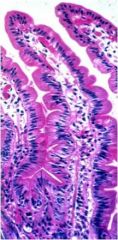
What is wrong with this small intestine?
|
Nothing, it's normal
|
|
Name the defect in this small intestine.
|
Nothing, it's normal.
|
|
|
What type of microscopic colitis is this - collagenous or lymphocytic?
|
Collagenous microscopic colitis
|
|

What type of microscopic colitis is this - collagenous or lymphocytic?
|
Collagenous microscopic colitis
|
|

What disease do these lymphocytic nodules suggest?
|
Common variable immunodeficiency - loss of IgG, sometimes T cell fxn
|
|
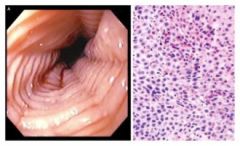
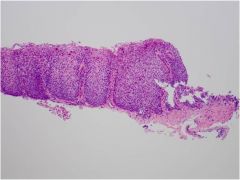
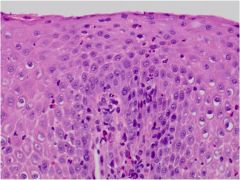
What is wrong with this esophagus?
|
Eosinophilic esophagitis
|
|
What type of microscopic colitis is this - collagenous or lymphocytic?
|
Lymphocytic microscopic colitis
|
|
Is this PBC or PSC? What is the "buzzword"?
|
PBC, florid duct lesion
|
|
What sign is shown here?
|
"String of beads" - primary sclerosing cholangitis
|
|
What is wrong with this large bile duct?
|
PSC, "onion skinning"
|
|

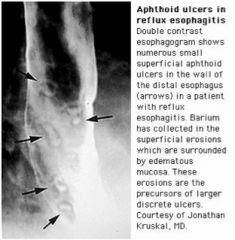
What pathology is seen in this barium study of the lower esophagus?
|
Achalasia (tonic contraction of LES due to loss of myenteric plexus)
|
|
This EM shows achalasia. What is the histopathological defect?
|
Loss and fibrosis of the myenteric plexus, which normally inhibits tonic contraction of the LES
|
|
What is wrong with this esophagus? How does this happen?
|
Achalasia --> food stasis --> inflammation of mucosa
|
|

This image shows a dilated esophagus. What is the most likely cause?
|
Achalasia (note that the LES is closed, and that the dilation is just above it)
|
|
What is wrong with this esophagus?
|
Adenocarcinoma, because the tumor forms glandular structures
|
|
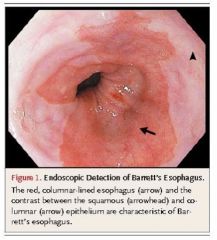
What precancerous lesion can be seen on this upper endoscopy?
|
Barrett's esophagus (--> adenocarcinoma, 0.12-0.5% per yr)
|
|
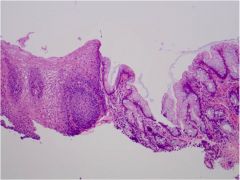
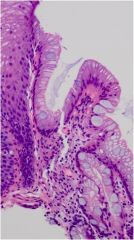
What metaplastic process has occurred in this esophagus?
|
Barrett's esophagus (esophageal squamous-->intestinal columnar with goblet cells)
|
|
Name the cell required for the diagnosis of this condition of the esophagus.
|
Goblet cells (not required in Europe or Japan, but they are predictive of transformation to adenocarcinoma)
|
|
This patient has achalasia. What causes the inflammation seen here?
|
Food impaction (seen at center of photograph)
|
|
What is wrong with this esophagus?
|
Eosinophilic esophagitis
|
|
What is wrong with this esophagus?
|
Eosinophilic esophagitis
|
|
What is wrong with this esophagus?
|
Esophageal varices
|
|

This is an esophageal cancer. Is it adenocarcinoma or squamous cell carcinoma?
|
Adenocarcinoma (making glands)
|
|
Is this esophageal adenocarcinoma or squamous cell carcinoma?
|
Adenocarcinoma (making glands)
|
|

What is wrong with this esophagus?
|
Esophageal varices
|
|
What is wrong with this gastroesophageal junction?
|
Reflux esophagitis
|
|
What is wrong with this esophagus?
|
Reflux esophagitis with an eosinophil (need >15/hpf for eosinophilic esophagitis)
|
|
What is wrong with this esophagus?
|
Reflux esophagitis
|
|
What is wrong with this esophagus?
|
Squamous cell carcinoma. Note the keratin pearls.
|
|

Does this patient have esophageal adenocarcinoma or squamous cell carcinoma?
|
Squamous cell carcinoma (no gland formation)
|
|
What type of cancer is seen in this esophagus?
|
Esophageal squamous cell carcinoma
|
|

Is this esophagus normal or not?
|
Yes, this is a healthy squamocolumnar junction.
|
|

Is this esophagus normal?
|
Yes. You can see the normal squamocolumnar junction.
|
|

Does this specimen of bowel show Crohn's or UC? Why?
|
Crohn's - thickened ileum near the ileocecal valve (most common site)
|
|

Does this barium swallow show achalasia or diffuse esophageal spasm?
|
Achalasia (LES only)
|
|

Does this barium swallow show achalasia or diffuse esophageal spasm?
|
Diffuse esophageal spasm
|
|

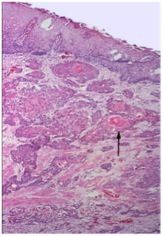
What is the arrow pointing at?
|
A tumor in the esophagus.
|
|

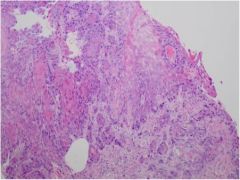
What is wrong with this stomach on endoscopy?
|
Gastric cancer
|
|

What is wrong with this stomach on UGI?
|
gastric cancer
|
|
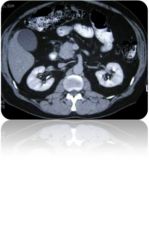
Name the abnormality.
|
Tumor in the head of the pancreas
|
|

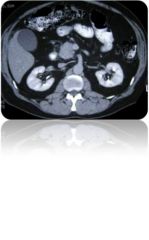
Name the abnormality.
|
Tumor in the head of the pancreas.
|
|
This patient has cancer. Where is the mass?
|
head of the pancreas
|
|
This patient has cancer. Where is the mass?
|
head of the pancreas
|
|

This patient has a tumor. Where is the mass?
|
Head of the pancreas
|
|

What type of tumor does this patient have? What neurotransmitter causes this?
|
Carcinoid tumor, 5-HT (serotonin)
|
|
This tumor is most likely found in the pancreas or duodenum. What is it, and what syndrome does it cause?
|
Gastrinoma, Zollinger-Ellison syndrome
|
|

This patient has a neuroendocrine tumor. Find the mass.
|
Head of the pancreas (VIPoma)
|
|

This patient has collagenomas and angiofibromas in addition to multiple endocrine tumors. What gene is defective?
|
Menin gene (MEN-1)
|
|

This patient has Marfanoid habitus and multiple endocrine tumors. What is his prognosis?
|
Very poor. Most patients with MEN-2b die shortly after presentation.
|
|

What condition is seen on this x-ray? What neuroendocrine tumor most likely caused it?
|
Pneumoperitoneum. If caused by a neuroendocrine tumor, it's most likely a perforation from hypersecretion secondary to gastrinoma.
|
|

What endocrine gland is this? Name the hormone(s) secreted by each zone.
|
Adrenal gland. Glomerulosa, aldosterone (mineralocorticoid); fasciculata, cortisol (glucocorticoids); reticularis, DHEA, androstenedione, etc (androgens); medulla, epinephrine and norepinephrine (catecholamines)
|
|

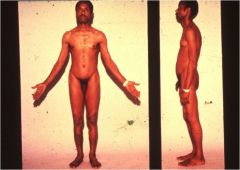
Why does this patient have hyperpigmentation?
|
Addison's disease. High ACTH production --> lots of POMC --> lots of MSH
|
|

What are the results this patient's cosyntropin stimulation test?
|
This patient probably has Addison's disease (at least, that's the Block 7 diagnosis!) Cosyntropin stimulation test would reveal low cortisol (<16 ug/dL or increments <7 ug/dL above baseline) and low aldosterone.
|
|
This patient presents with cramping, parasthesias, fatigue, and hypertension. What is the most likely diagnosis?
|
Aldosterone-secreting adrenal adenoma
|
|

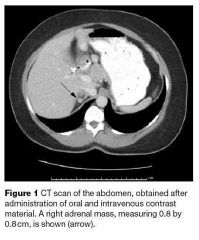
This patient presents with headaches, sweating, and palpitations. She also feels flushed, anxious, and nauseated. What is the most likely diagnosis?
|
Adrenal pheochromocytoma
|
|
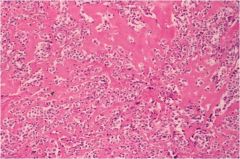
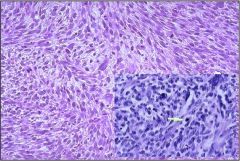
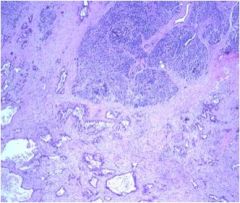
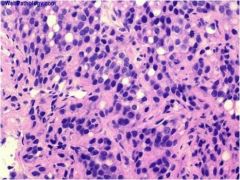
What type of thyroid cancer is this?
|
Anaplastic thyroid carcinoma
|
|
What is the prognosis of this type of thyroid cancer?
|
Poor (anaplastic thyroid carcinoma)
|
|
What type of thyroid cancer is this?
|
Anaplastic thyroid carcinoma
|
|
You perform an FNA on someone with goiter, and all you get is collagen. Diagnosis?
|
Chronic sclerosing thyroiditis
|
|
This patient has goiter. Does she have chronic sclerosing thyroiditis or Graves' disease?
|
Chronic sclerosing thyroiditis
|
|
Chronic sclerosing thyroiditis or Grave's disease?
|
Chronic sclerosing thyroiditis
|
|
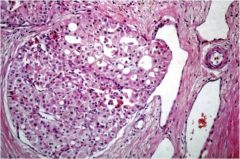
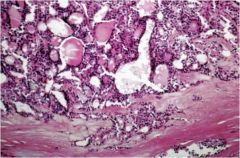
What condition is seen in this thyroid?
|
Chronic sclerosing thyroiditis
|
|

Is this thyroid mass benign or malignant? How can you tell?
|
Very well-circumscribed benign follicular adenoma
|
|
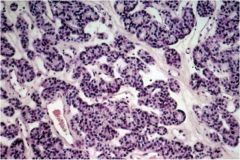
What type of thyroid neoplasia is this?
|
Follicular adenoma
|
|
This is a thyroid neoplasia. Is it benign or malignant?
|
Benign follicular adenoma
|
|
Is this benign (follicular adenoma) or malignant (follicular thyroid carcinoma)?
|
Malignant follicular thyroid cancer. You can tell because it's invading a blood vessel.
|
|
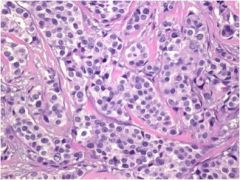
This image shows the hallmark sign of which type of thyroid cancer?
|
Follicular thyroid carcinoma, invasion of blood vessel on left
|
|
Name the thyroid neoplasia seen here.
|
Malignant follicular thyroid carcinoma, invading the capsule
|
|
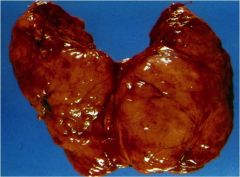
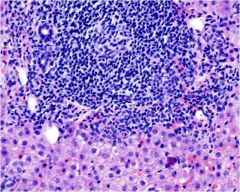
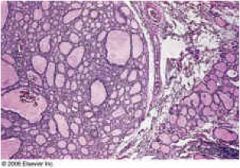
This thyroid is diffusely enlarged. What is the most likely diagnosis?
|
Hashimoto thyroiditis
|
|
What type of autoimmune thyroid disease is seen here?
|
Hashimoto thyroiditis
|
|
Hashimoto's or Graves' disease?
|
Hashimoto's
|
|
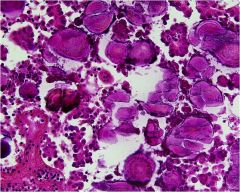
What characteristic cell is shown in this image of Hashimoto's thyroiditis?
|
Oncolytic cells (Hurthle cells are also diagnostic)
|
|

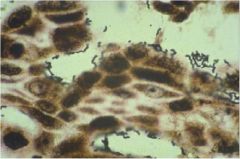
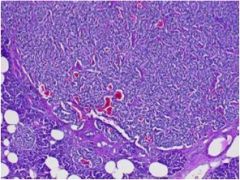
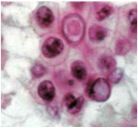
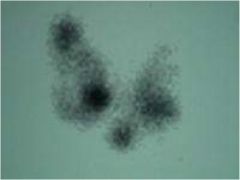
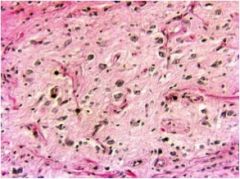
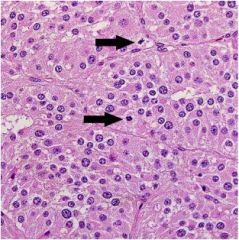
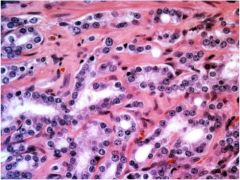
What characteristic of medullary thyroid cancer is seen here?
|
Salt and pepper nuclei (chromatin)
|
|
From which cell did this thyroid cancer originate?
|
Parafollicular C cells (medullary thyroid cancer)
|
|
With what genetic syndrome is this thyroid cancer associated?
|
MEN2a/2b (RET mutations)
|
|
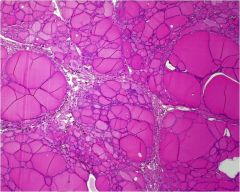
What is wrong with this thyroid?
|
Multinodular goiter
|
|

Does this patient have multinodular goiter or Graves' disease?
|
Multinodular goiter. Graves' is diffuse hyperplasia
|
|

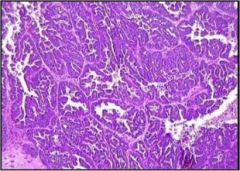
What type of thyroid cancer is shown?
|
Papillary thyroid cancer, intranuclear grooves (also characteristic are intranuclear pseudoinclusions, Orphan Annie nuclei)
|
|
What are these?
|
Psammoma bodies, in this case due to papillary thyroid carcinoma
|
|
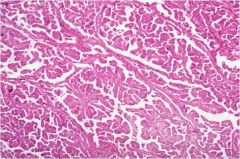
What type of thyroid cancer is this?
|
Papillary thyroid carcinoma (these are papillae!)
|
|
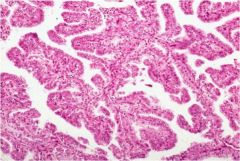
Is this thyroid normal?
|
NO, this is papillary thyroid carcinoma. There are no normal follicles
|
|
These multinucleated giant cells are commonly seen in the thyroids of mothers exposed to Coxsackie virus by their young children. Diagnosis?
|
Subacute thyroiditis
|
|
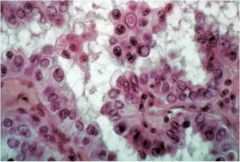
This is papillary thyroid cancer. What characteristic feature is shown here? What are the other 2?
|
These are intranuclear pseudoinclusions. Also characteristic are Orphan Annie nuclei (optically clear nuclei) and nuclear grooves.
|
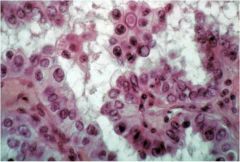
|
This is papillary thyroid cancer. What characteristic feature is shown here? What are the other 2?
|
These are intranuclear pseudoinclusions. Also characteristic are Orphan Annie nuclei (optically clear nuclei) and nuclear grooves.
|
|
What are these?
|
Orphan Annie (optically clear) nuclei in papillary thyroid carcinoma.
|
|
What are these?
|
Intranuclear pseudoinclusions in papillary thyroid CA.
|
|

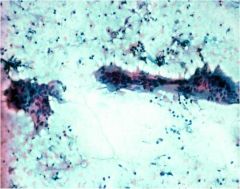
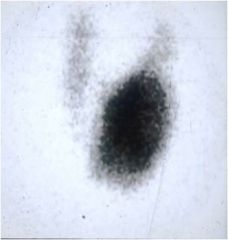
What percentage of nodules look like this on radioiodide uptake scan?
|
90% are cold nodules; this is why radioiodide scan isn't 1st line anymore--it doesn't really help. Do FNA instead.
|
|

What happened to this person's neck?!
|
Goiter compressing the trachea
|
|
What percentage of these thyroid nodules are cancerous?
|
Hot nodule, <1% are cancerous. Only account for 10% of all nodules; do FNA instead!
|
|
Normal thyroid vs. multinodular goiter?
|
Multinodular goiter
|
|
Diagnose this thyroid condition.
|
Multinodular goiter
|
|
What is wrong with this thyroid?
|
Nothing, it's normal
|
|
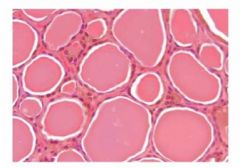
What is wrong with this thyroid?
|
Nothing, it's normal
|
|

Diagnose this patient and explain the mechanism of these findings.
|
Graves' disease, with proptosis and paralysis of an extraocular muscle due to infiltration of the periorbital connective tissue and EOMs
|
|
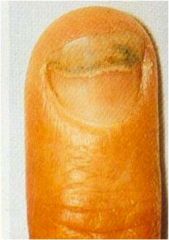
Does this patient most likely have hyperthyroidism or hypothyroidism?
|
Hyperthyroidism, Graves' disease --> onycholysis
|
|

What endocrine problem is this patient most likely to have?
|
This patient has R CNIII palsy. The endocrine problem most likely to cause this is a pituitary macroadenoma compressing CNIII.
|
|
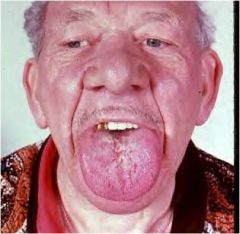
Diagnosis?
|
Acromegaly with macroglossia
|
|

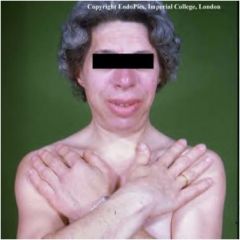
Diagnosis?
|
Acromegaly with macrognathia
|
|
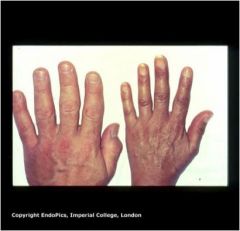
Diagnosis (on left)?
|
Acromegaly, enlarged hands
|
|

Aside from hyperinsulinemia in T2DM, excesses of which 2 hormones can cause this condition?
|
This is acanthosis nigricans due to insulin resistance. In addition to diabetes mellitus type 2, it can be caused by high growth hormone or high cortisol.
|
|
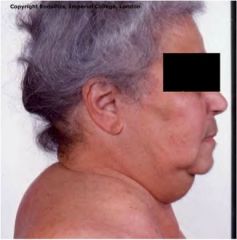
Diagnosis?
|
Acromegaly
|
|
Diagnosis and most common cause?
|
Cushing's syndrome, MCC=iatrogenic glucocorticoid administration
|
|

Diagnosis and findings?
|
Cushing's syndrome. Findings seen in this photo include truncal obesity, buffalo hump, moon facies, violaceous striae, muscle wasting.
|
|

What hormone is this patient missing?
|
GnRH, Kallman's syndrome
|
|
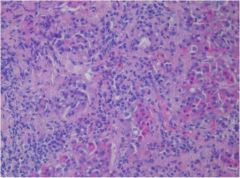
What is wrong with this anterior pituitary gland?
|
Lymphocytic hypophysitis
|
|
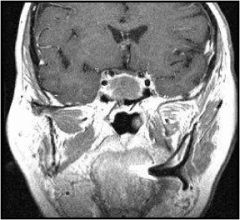
What is wrong with this picture?
|
Giant pituitary gland, in this case from macroadenoma.
|
|
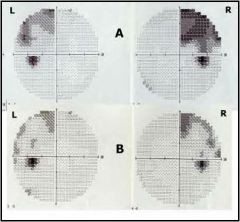
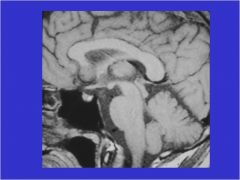
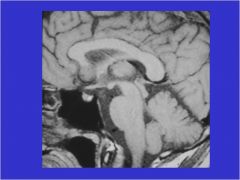
What is the most likely cause for this visual field defect?
|
Pituitary macroadenoma
|
|
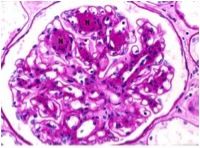
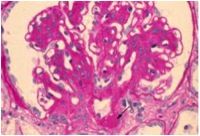
What is wrong with this kidney?
|
Diabetic nephropathy (mesangial thickening)
|
|
What is wrong with this kidney?
|
Diabetic nephropathy
|
|

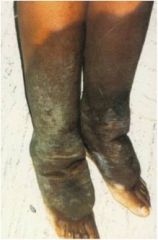
Why does clawing of the feet occur in diabetes?
|
Diabetic neuropathy --> atrophy of intrinsic muscles of feet --> clawing
|
|

What is wrong with this eye?
|
Diabetic retinopathy
|
|
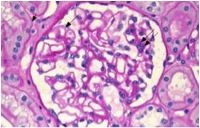
What is wrong with this kidney?
|
Nothing, this is a normal glomerulus
|
|

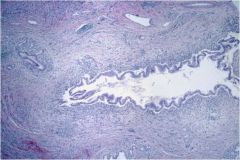
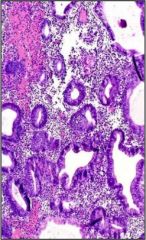
What is wrong with this uterus?
|
Complex endometrial hyperplasia
|
|
What is this?
|
Endometriosis
|
|

What cancer was this woman at risk for, and how common is it?
|
Leiomyosarcoma, extremely rare. She had leiomyomata (fibroids).
|
|
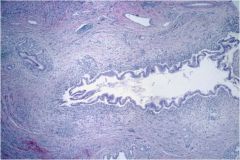
What, if anything, is wrong with this uterus?
|
Simple endometrial hyperplasia
|
|

Diagnosis and definition?
|
Adenomyositis, where the endometrium invades the myometrium
|
|
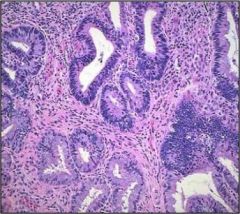
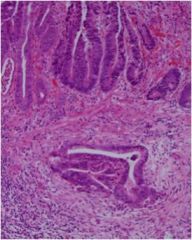
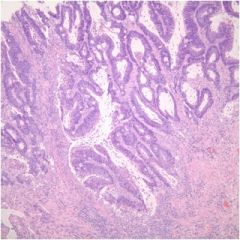
What is wrong with this cervix?
|
Cervical adenocarcinoma
|
|
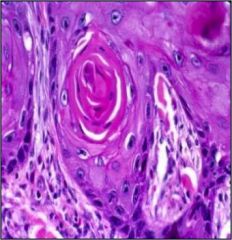
What is wrong with this cervix?
|
Squamous cell carcinoma of the cervix (keratin pearl)
|
|
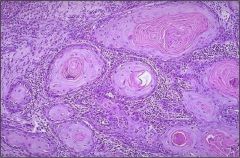
What is wrong with this cervix?
|
Squamous cell carcinoma of the cervix (keratin pearls)
|
|
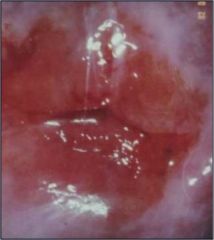
What is wrong with this cervix?
|
Chronic cervicitis
|
|
Acute or chronic endometritis, and why?
|
Chronic, plasma cells
|
|
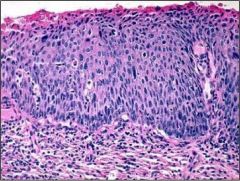
Is this normal or neoplastic cervix?
|
Cervical intraepithelial neoplasia grade II
|
|

What is this?
|
an endocervical polyp
|
|
What type of endometrial cancer is this?
|
clear cell
|
|
What type of endometrial cancer is this?
|
Papillary serous
|
|
What type of endometrial cancer is this?
|
Papillary serous
|
|

What is this?
|
Endometriosis (chocolate cysts)
|
|

What are the theories for how this tissue develops?
|
This is endometriosis. Theories: regurgitation (out the Fallopian tubes); metaplasia (of peritoneal/abdl/gyn structures); hematogenous spread
|
|
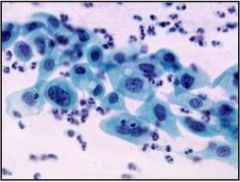
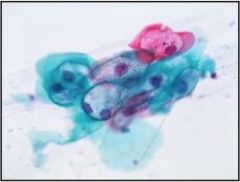
This is a Pap smear. Is this normal, low grade, or high grade?
|
High grade
|
|
This is a Pap smear. Normal, low grade, or high grade?
|
High grade (enlarged nucleus!)
|
|
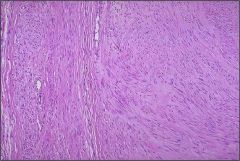
Is this a leiomyoma or a leiomyosarcoma?
|
leiomyoma (fibroid) - benign
|
|
Is this a leiomyoma or a leiomyosarcoma?
|
Leiomyosarcoma (malignant), a leiomyoma would look like normal smooth muscle
|
|
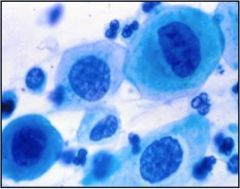
This is a Pap smear. Is it normal, low grade, or high grade?
|
Low grade dysplasia
|
|
This is a Pap smear. Is it normal, low grade, or high grade?
|
Normal
|
|

What is this?
|
Vulvar squamous cell carcinoma, sometimes caused by HPV. (The lecture says this is vaginal, but unless it's a metastasis, I don't see how this is the vagina.)
|
|
What is wrong with this endometrium?
|
Endometrial cancer, papillary serous type
|
|
What organ is this?
|
Uterus. You can see the outline of the endometrium.
|
|
What element of a teratoma, shown here, confers malignancy in a female?
|
Immature neural elements, otherwise they're benign in females. Teratomas in post-pubertal men are considered malignant.
|
|
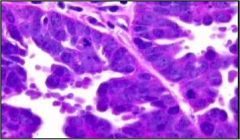
What type of ovarian cancer is this?
|
clear cell
|
|
Believe it or not, this is ovarian cancer. What type?
|
Endometrioid
|
|
What type of ovarian cancer is this?
|
mucinous
|
|
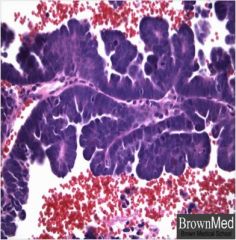
What type of ovarian cancer is this?
|
papillary serous cystadenocarcinoma
|
|

This patient has ovarian cancer. What should the surgeon do at this point?
|
Remove as much of the tumor as possible! One of the few cancers where aggressive surgical removal improves outcomes. Preferably, this surgery should be done by a gynecologic oncologist, not a "regular" ob/gyn or a general surgeon.
|
|

What is this?
|
Teratoma
|
|

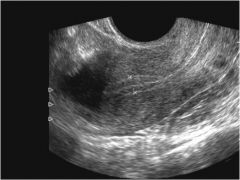
This is an ultrasound of an ovary. Diagnosis?
|
PCOS
|
|

What does this female patient probably have?
|
This patient has hirsutism and acanthosis nigricans. MCC=PCOS
|
|
Should this XY patient's testes be removed, and if so, when?
|
This patient has androgen insensitivity syndrome and thus intra-abdominal testes. This is the 1 exception to the rule about removing undescended testes ASAP--allow the patient to go through puberty first, then remove at age 16-18.
|
|

Diagnosis?
|
Imperforate hymen
|
|

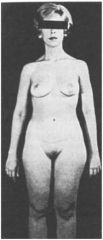
Will this patient most likely present with primary or secondary amenorrhea?
|
This patient has Turner's syndrome (45X) and will most likely present with primary amenorrhea.
|
|
What's wrong with this uterus?
|
Bicornate uterus, from failure of mullerian ducts to fuse properly
|
|

What is this?
|
endometriosis
|
|

What is this?
|
endometriosis
|
|
What is the cause of this patient's infertility?
|
Tubal factor (Fallopian tubes are swollen and likely blocked)
|
|
What is wrong with this uterus?
|
septate uterus
|
|
|
What is Virchow's triad?
|
Identifies the 3 major factors in clotting risk: hypercoagulability, stasis, and endothelial injury.
|
|
|
What is the definition of preterm birth?
|
<37 weeks gestation
|
|
|
What is the definition of very preterm birth?
|
<32 weeks gestation
|
|

What 4 factors may have contributed to this baby's condition?
|
This baby is premature. 4 factors: stress (premature activation of HPA axis); infection/inflammation; uteroplacental ischemia; pathological uterine stretching
|
|
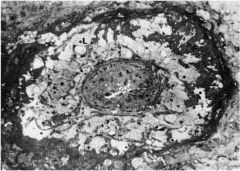
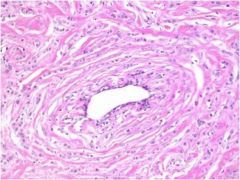
This EM shows the spiral artery of a pregnant woman. What is wrong?
|
The artery is occluded, preventing good blood flow to the baby. Uteroplacental ischemia can lead to preterm delivery.
|
|

Diagnosis?
|
Anembryonic gestation (there is no embryo!)
|
|
A woman's pregnancy is terminated and the entire product of conception looks like this. What is the typical karyotype?
|
46XX or 46XY
|
|
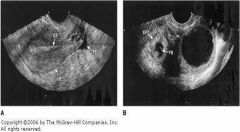
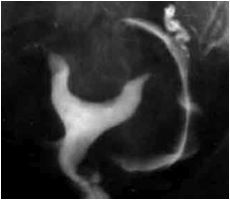
Is the ectopic pregnancy on the left or the right?
|
right
|
|
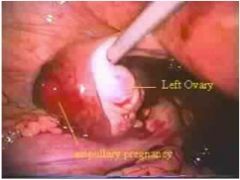
Diagnosis?
|
Ectopic pregnancy.
|
|
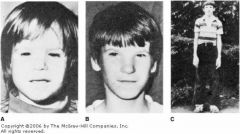
What teratogen was this boy exposed to as a fetus?
|
alcohol
|
|

Gastroschesis or omphalocele?
|
Gastroschesis
|
|
A woman who is 10 weeks pregnant presents with vaginal bleeding. Is this a threatened abortion, incomplete abortion, or complete abortion?
|
Incomplete abortion
|
|

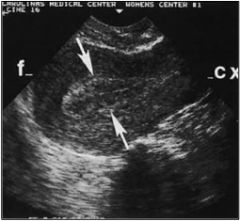
Diagnosis?
|
Pregnancy (intrauterine!)
|
|

Diagnosis?
|
Intrauterine pregnancy
|
|

Diagnosis?
|
Partial mole (69XXX or 69XXY)
|
|
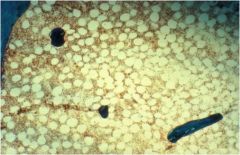
This patient has elevated alkaline phosphatase. Diagnosis?
|
Osteomalacia, an excess of unmineralized bone
|
|
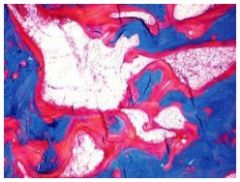
If the blue dye stains bone, what is the diagnosis?
|
Osteoporosis. The bone has been replaced by fat.
|
|
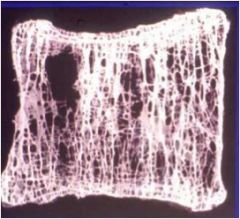
Diagnosis?
|
Osteoporosis
|
|
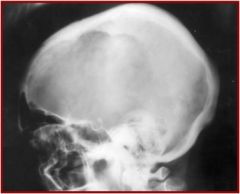
Diagnosis?
|
Paget's, osteolytic phase
|
|

Diagnosis?
|
Paget's, sclerotic phase
|
|
This patient's symptoms began in adulthood. What is his diagnosis?
|
Paget's disease of the bone (lower extremity deformation)
|
|
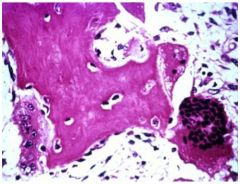
This is a bone biopsy. Diagnosis?
|
Paget's disease of the bone
|
|
This patient's symptoms began in childhood. Diagnosis?
|
Rickets secondary to vitamin D deficiency
|
|
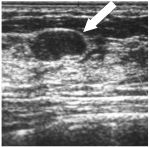
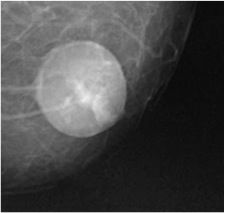
Most likely benign or malignant?
|
Benign - well-circumscribed borders
|
|
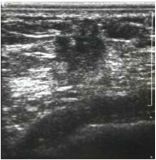
Is this breast mass most likely benign or malignant?
|
Malignant - irregular, unclear borders
|
|

Diagnosis?
|
Breast abscess
|
|
Diagnosis? (hint: breast)
|
fat necrosis
|
|
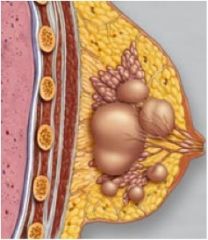
Diagnosis?
|
Fibrocystic changes, caused by blockage of ducts
|
|

This shows a breast duct. Diagnosis?
|
Intraductal papilloma
|
|

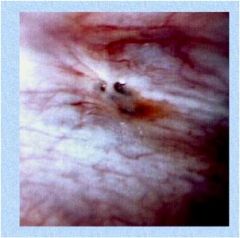
You notice this at an annual physical. The patient did not have this last year. What must you evaluate for?
|
Breast mass!
|
|

Diagnosis?
|
Phyllodes tumor
|
|

Is this most likely a simple cyst or breast cancer?
|
simple cyst
|
|

Diagnosis?
|
Inflammatory breast cancer
|
|
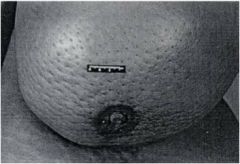
What sign characterizes this case of inflammatory breast cancer?
|
Peau d'orange
|
|
Ductal or lobular carcinoma of the breast?
|
ductal
|
|
Ductal or lobular carcinoma of the breast?
|
Lobular
|
|

Diagnosis?
|
Paget's disease of the breast, associated with malignancy ~97% of the time
|
|

Diagnosis?
|
Paget's disease of the breast, associated with malignancy 97% of the time
|
|
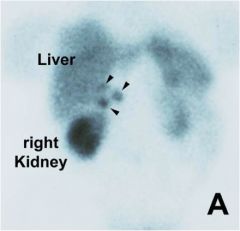
What neuroendocrine tumor is this if the scan was performed with octreotide?
|
gastrinoma
|
|
Is this pituitary gland normal or abnormal?
|
Normal
|
|
Is this pituitary gland normal or abnormal?
|
Normal
|
|

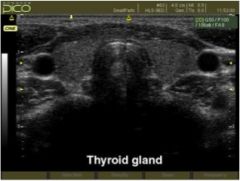
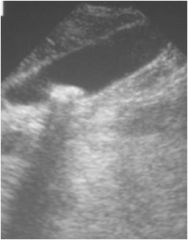
What does this ultrasound show?
|
1 enlarged parathyroid gland
|
|
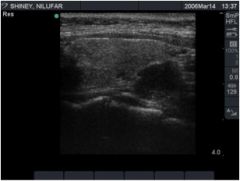
Might this patient have MEN-1?
|
This ultrasound shows 1 enlarged parathyroid gland. MEN-1 patients typically have 4 gland hyperplasia.
|
|
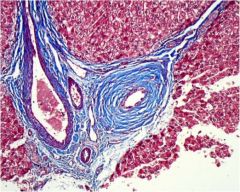
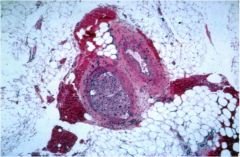
This paraganglionoma was removed from a patient's heart. What hormones might this tumor secrete?
|
Catecholamines (paraGANGLIONoma)
|
|

For 3rd year: should you operate on this patient?
|
No
|
|

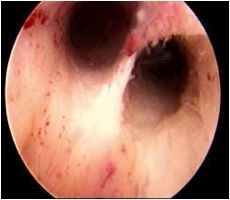
What is seen in this esophagus on endoscopy?
|
Barrett's esophagus
|
|
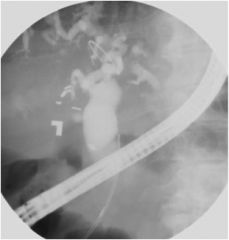
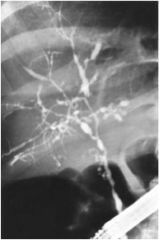
What does this endoscopic retrograde cholangiopancreatography (ERCP) show?
|
Dilated bile ducts, in this case due to an obstructing tumor on the head of the pancreas
|
|
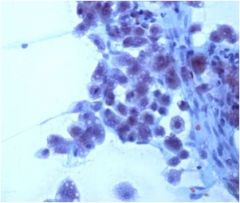
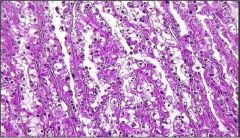
A liver nodule is aspirated. Diagnosis?
|
Hepatocellular carcinoma
|
|
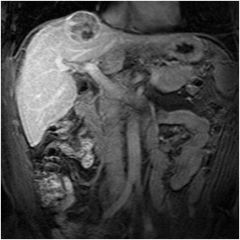
Diagnosis?
|
Hepatocellular carcinoma
|
|
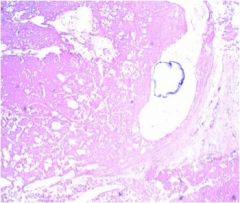
What viruses can cause this liver pathology?
|
This is hepatocellular carcinoma, caused by HBV or HCV
|
|
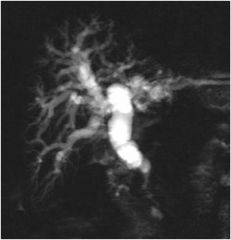
What does this magnetic resonance cholangiopancreatography (MRCP) show?
|
Dilated bile ducts, in this case due to an obstructing tumor in the head of the pancreas
|
|
Name the completed operation and 1 indication.
|
Nissen fundoplication for severe, medically intractable GERD
|
|
Is this a normal or abnormal pancreas?
|
Abnormal - this is pancreatic adenocarcinoma
|
|

Name this and 2 other extraintestinal manifestations of IBD.
|
This is pyoderma gangrenosum. Other EIMs include primary sclerosing cholangitis (PSC), ankylosing spondylitis, uveitis, episcleritis, erythema nodosum, etc.
|
|
Is this rectum normal or neoplastic?
|
This is rectal adenocarcinoma
|
|
Diagnose this rectal biopsy.
|
Rectal adenocarcinoma
|
|

This CT shows a colon abnormality. Does this patient have ulcerative colitis or Crohn's disease?
|
Ulcerative colitis. The mucosa is diffusely inflamed, no cobblestoning, strictures or skip lesions
|
|
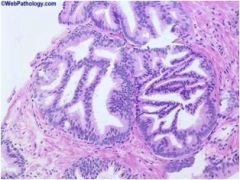
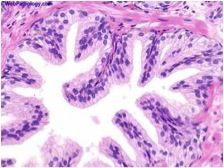
Is this prostate normal or abnormal?
|
These are atypical glands, which have a 50% chance of co-occurring cancer if found on biopsy.
|
|

Gleason grades
|
YAY!
|
|
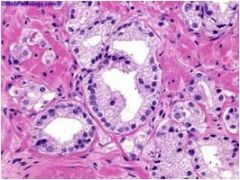
This is high grade prostatic intraepithelial neoplasia (HGPIN). What histopathologic features characterize this diagnosis?
|
Normally formed glands composed of abnormal (dysplastic) cells
|
|
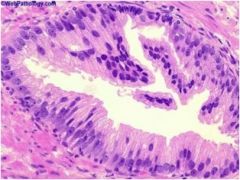
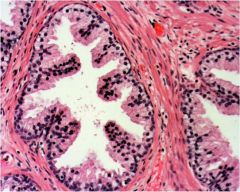
Is this prostate normal?
|
No, this is high grade prostatic intraepithelial neoplasia (a form of dysplasia)
|
|

This CT is from a 19 YO male. What is the most likely origin of the mass?
|
testicular cancer
|
|
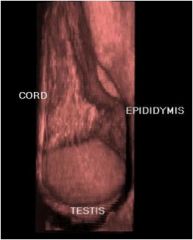
Is this testicular ultrasound normal or not?
|
Normal
|
|
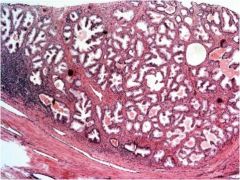
Diagnose this prostate.
|
Benign prostatic hyperplasia
|
|

Diagnosis?
|
hydrocele
|
|
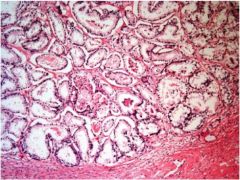
Is this prostate normal or not?
|
normal
|
|

What has happened to this testicle?
|
testicular torsion
|
|

What is the most likely diagnosis if this man's urethra has narrowed to a slit?
|
benign prostatic hyperplasia
|
|

Diagnosis?
|
BPH
|
|
Is this benign prostatic hyperplasia or prostate cancer?
|
BPH
|
|
Is this gleason grade 1, 3, or 5?
|
gleason 1
|
|
Is this gleason grade 1, 3, or 5?
|
gleason 3
|
|
Is this gleason grade 1, 3, or 5?
|
gleason 5
|
|
Is this prostate normal or not?
|
Normal
|
|
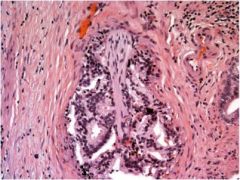
What hallmark feature of prostate cancer is shown here?
|
perineural invasion
|
|
Is the prostate cancer on the left or the right?
|
right
|
|
Is this tissue normal prostate or prostate cancer?
|
prostate cancer
|
|

What organ is this? What are the two dark spots in the middle of the white circles?
|
This is the penis. The dark spots are the cavernosal arteries within the corpora cavernosa.
|
|

Why does this man probably have androgen deficiency?
|
He's elderly.
|
|
What is his karyotype?
|
47XXY (Klinefelter's)
|
|
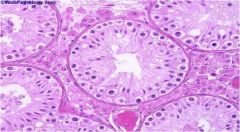
Why is this man infertile?
|
This man has a complete lack of germ cells - has Sertoli cells only.
|
|

If this Caucasian patient has congenital absence of the vasa deferentia, what gene is most likely mutated?
|
CFTR
|
|
Why is this man infertile?
|
The maturation of his sperm is arrested.
|
|
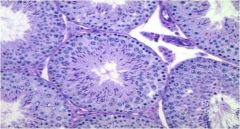
Why is this man infertile?
|
This is a normal testicular biopsy. He must have a problem downstream (eg obstruction, abnormal motility, etc.)
|
|

What study has been performed? What is the normal result?
|
This is a seminal vesiculography. You inject dye into the seminal vesicle and the bladder should light up, otherwise there's an obstruction. This result is normal.
|
|

What is this person's genotype?
|
46XY, Kallman's syndrome (lack of GnRH, anosmia)
|
|

Why might this individual present for medical attention?
|
Infertility, Klinefelter's syndrome (47XXY)
|
|

What feature of Klinefelter's syndrome is shown on the left?
|
Testicular atrophy
|
|
Diagnosis?
|
Pretibial myxedema from hyperthyroidism
|
|

This patient has familial hypercholesterolemia. What are these?
|
corneal arcus (top), xanthomas (bottom)
|
|
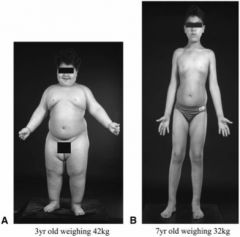
What hormone has been replaced in this boy?
|
Leptin
|
|

The mouse on the right has a congenital deficiency of what hormone?
|
Leptin
|
|
|
What 2 benign breast lesions have the highest risk of developing into invasive carcinoma?
|
Atypical ductal and atypical lobular hyperplasia
|
|
|
What is the most common type of breast cancer?
|
Invasive ductal (70-80%) followed by invasive lobular (5-10%)
|
|
|
Which breast neoplasia must be surgically excised, as it is premalignant: lobular carcinoma in situ or ductal carcinoma in situ?
|
DCIS (12% progress to cancer). LCIS is a marker for risk of breast cancer, but cancer does not develop from LCIS.
|
|
|
Which is associated with ulcerative colitis: pANCA or ASCA?
|
pANCA is associated with UC and colonic Crohn's disease. ASCA is associated with small bowel Crohn's.
|
|
|
Which is associated with a better prognosis in sporadic colorectal cancer: microsatellite instability or chromosomal instability?
|
Microsatellite instability
|
|

Diagnosis?
|
appendicitis
|
|
Diagnosis (small bowel)?
|
celiac disease
|
|
Diagnosis?
|
cholelithiasis
|
|

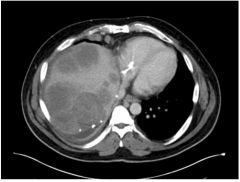
Diagnosis?
|
Cirrhosis with hepatocellular carcinoma
|
|
Diagnosis?
|
colon cancer, "apple core" lesion
|
|

Is this obstruction in the colon or small bowel?
|
colon
|
|
This is a section of colon. What is this?
|
diverticulum
|
|
Diagnosis?
|
fatty liver
|
|
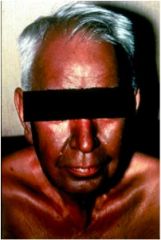
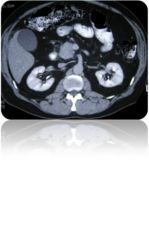
Diagnosis?
|
hemochromatosis
|
|
Diagnosis?
|
Normal abdomen!
|
|

Diagnosis
|
pancreatic calcifications, secondary to chronic pancreatitis
|
|

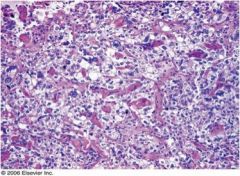
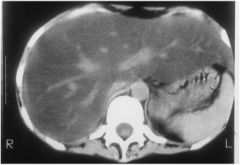
Diagnosis?
|
Pancreatic phlegmon (solid mass of swollen, inflamed pancreas often containing patchy areas of necrosis)
|
|
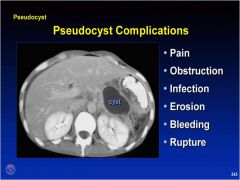
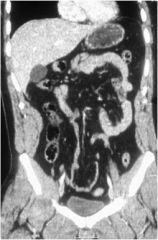
What disease most likely precipitated this pancreatic pseudocyst?
|
acute pancreatitis
|
|

Diagnosis?
|
Pneumoperitoneum secondary to perforation
|
|

Is this obstruction in the colon or small bowel?
|
small bowel
|
|
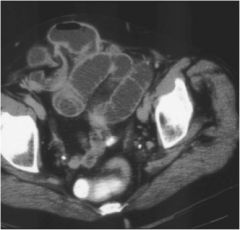
Diagnosis?
|
Small bowel obstruction
|
|

Is this ulcerative colitis or Crohn's disease?
|
ulcerative colitis, "lead pipe" colon
|