![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
70 Cards in this Set
- Front
- Back
- 3rd side (hint)
|
What is Pulmonary Oedema? |
An accumulation of fluid in the lung tissue and alveoli. |
|
|
|
A common cause is congestive heart failure is |
PO |
|
|
|
what are the two categories of PO? |
Two broad cateogories: - Cardiogenic PO - Non-Cardiogenic PO |
|
|
|
how much water does a healthy lung contain? |
A normal healthy lung contains very little water or fluid. |
|
|
|
what are alveoli in the lungs lined with and why? |
Alveoli are lined by a thin layer of water molecules so gases will notdiffuse across dry surfaces |
|
|
|
how is the lungs kept dry then? |
It is kept dry by the lymphatics which drain the fluid from theinterstitial space and the balance of forces from: - capillary hydrostatic pressure, - capillary oncotic pressure, - permeability of the capillaries. |
|
|
|
what does surfactatnt lining the alveoli do? |
Surfactant lining the alveoli repels water, keeping fluid from enteringthe alveoli. |
|
|
|
what are Predisposing factors for Pulmonary Oedema? |
- Heart Disease - ARDS - Inhalation of toxic gases |
HAI "chinese seving PO soup said Hai" |
|
|
Pulmonary edema is caused by a complication of what? |
- a myocardial infarction (heart attack) - mitral or aortic valve disease - cardiomyopathy, or other disorders characterized by cardiacdysfunction. |
|
|
|
what is the pathophysiology of PO? |
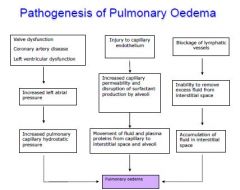
1 Fluid backs up into the capillaries of the lungs. 2 Increased pressure in these capillaries forces fluid out of thecapillaries and into the air spaces (alveoli). 3 This interferes with the exchange of oxygen and carbon dioxide inthe alveoli. |
|
|
|
what are the various mechanisms contributing to PO? |
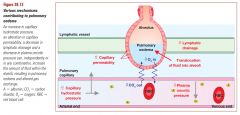
low lymphatic drainage low plasma oncotic pressure high capillary permeability high capillary hydrostatic pressure translocation of fluid into alveoli |
|
|
|
how serious is PO? |
PO is a medical emergency! Hospitalization and immediatetreatment are required. |
|
|
|
what are the symptoms of PO?
|
1 Dysponoea 2 inability to lie down 3 decreased oxygen content of blood 4coughing(pink frothy sputum in severe cases.) 5 inspiratory crackles and wheezes 6 fast heart rate, pale appearance and sweating 7white fields on X rays |
|
|
|
what is dysponoea? |
extreme shortness of breath, severe difficult breathing |
|
|
|
dwhat is ecreased oxygen content of the blood due from? |
due to increased distance of diffusion distances in thelungs and waterlogged alveoli. |
|
|
|
Coughing – pink frothy sputum in severe cases is due to? |
colour due to capillary haemorrhages |
|
|
|
Inspiratory crackles and wheezes in PO is due to? |
due to water in the alveoli |
|
|
|
Fast heart rate, pale appearance and sweating in PO due to? |
due to activation of the sympathetic nervous system |
|
|
|
White fields on X rays in PO due to? |
due to water in lungs. |
|
|
|
what are tests that can be done to test for PO? |
1. Blood oxygen 2. A chest X-ray 3. An ultrasound of the heart (echocardiogram) |
|
|
|
what may the tests show on result of person with PO? |
1. Blood oxygen levels (low) 2. A chest X-ray may reveal the following: - Fluid in or around the lung space - Enlarged heart 3. An ultrasound of the heart (echocardiogram) may reveal thefollowing: - Weak heart muscle - Leaking or narrow heart valves - Fluid surrounding the heart |
|
|
|
what is the AIM of the treatment for person with PO? |
The aim of treatment is to remove fluid from the lungs, to improveoxygenation of the blood and to correct the underlying cause of theoedema. |
|
|
|
what is the treatment for person with PO? |
Treatment involves both physical and chemical treatments anddepends on the cause of the oedema. |
|
|
|
what is the physical treatment for person with PO? |
Oxygen is given in high concentrations, by a mask or throughendotracheal tube using mechanical ventilation.Patient is put in the sitting position to reduce venous return. |
|
|
|
what is the chemical treatment for person with PO? |
Morphine - Reduce pain - Reduces sympathetic activity, thereby reducing afterload,preload, venous return, ventricular dilation and pressuresin the ventricles and thus reduces congestion in thepulmonary circulation. Medications include: Potent Loop Diuretics and ACE inhibitors |
|
|
|
how do potent loop diuretics work for treating PO? |
- To remove fluid. - Rapidly reduce blood volume and to dilate arterioles,thereby reducing afterload and hence the work of the heart. - Help removal of oedema from the lungs by increasing theexcretion of salt and water by the kidneys. |
|
|
|
how do ACE inhibitors work for treating PO? |
ACE inhibitors - Decrease salt and water retention and vasoconstriction. - Reducing afterload, preload, cardiac work and otherparameters - and other medications to treat the underlying cardiacdisorder. |
|
|
|
describe the blood flow in the pulmonary circulation |
Blood flows from the right ventricle through the pulmonary artery. (RV to PA) Blood reaches the capillaries surrounding alveoli where gas exchangeoccurs.(BRCSAWGEO) Oxygenated blood returns by pulmonary veins to the left ventricle whereit is pumped into systemic circulation.(PV to LV pumped into SC) |
|
|
|
what are sites of exchange and bring blood within reach of every cell |
capillaries |
|
|
|
what are ideally suited to enhance diffusion? |
capillaries |
|
|
|
how are capillaries ideally suited to enhance diffusion?
|
1. Diffusing molecules only travel short distances between blood andcells. Capillary walls are very thin, narrow and have extensivebranching
2. Tremendous number of capillaries – enormous surface area forexchange 3. Blood flows slowly through capillaries. Due to the extensivebranching that slows the velocity of blood flow. |
|
|
|
The speed at which blood travels is slower through where compared to elsewhere in the circulatory system? |
The speed at which blood travels is slower through the capillaries thanelsewhere in the circulatory system. |
|
|
|
what are the forces that act on the capillaries? |
Starling forces – four forces that influence fluid movement acrosscapillary walls. 1. Capillary blood pressure (Pc) 2. Plasma colloid osmotic pressure (oncotic pressure) πP 3. Interstitial fluid hydrostatic pressure (PIF) 4. Interstitial fluid-colloid osmotic pressure (πIF) |
|
|
|
To calculate the net exchange pressure... |
To calculate the net exchange pressure we have to take intoconsideration the outward pressures and the inward pressures that areexerted on the wall of the capillary.
Net exchange pressure = (Pc + πIF) - (πP + PIF) basically NEP= (outward pressure) - ( inward pressure) |
|
|
|
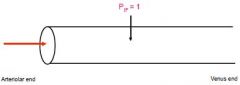
what ios the Capillary blood pressure (Pc) |
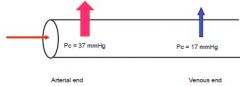
it is the fluid or hydrostatic pressureexerted on the inside of the capillary walls by the blood. Forces higher at arterial end than venous end of capillary |
|
|
|
what is the Plasma colloid osmotic pressure (oncotic pressure) πP |
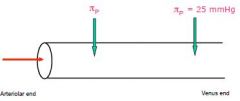
it is the forcecaused exerted by the plasma proteins.
- Plasma colloid osmotic pressure averages 25 mmHg. - Pressure moves fluid into the capillaries. Plasma proteins remain inside the capillary, very low concentration ofplasma proteins are found in the interstitial fluid surrounding thesystemic tissues. |
|
|
|
what is the Interstitial fluid hydrostatic pressure (PIF) |
it is the pressure exerted on theoutside of the capillary wall by the interstitial fluid. Pressure tends toforce fluid into the capillaries - 1 mmHg |
|
|
|
what is the Interstitial fluid-colloid osmotic pressure (πIF) |
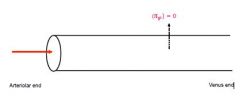
in normal conditionsdoes not contribute significantly to bulk flow (0 mmHg). The small fraction of plasma proteins that leak across the capillary wallsinto the interstitial fluid are normally returned to the blood via thelymphatics. |
|
|
what are the defentiions and formular to calculate the Net ecxhange pressure (NEP) |
Capillary blood pressure (Pc) Plasma colloid osmotic pressure (oncotic pressure) πP Interstitial fluid hydrostatic pressure (PIF) Interstitial fluid-colloid osmotic pressure (πIF) the formular used is Net exchange pressure = (Pc + πIF) - (πP + PIF)(outward pressure) - ( inward pressure) |
|
|
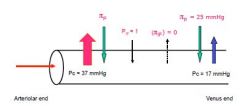
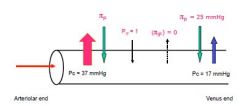
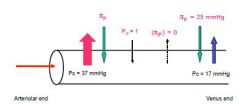
now calculate the NEP |
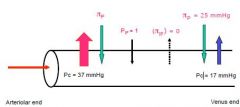
NRP = (Pc + πIF) - (πP + PIF) aka (outward pressure) - ( inward pressure) Forces at arteriolar end = (37+0) - (25 + 1) = 37 – 26 = 11 mmHg Net Outward Pressure (Ultrafiltration) meaning (pushes fluid (protein free) out of the capillary) Forces at the venular end = (17+0) - (25 + 1) = 17 - 26 = 9 mmHg Net Inward Pressure(Reabsorption) meaning (pushes fluid back into the capillary) Note when calculating reabsorption the value you calculate will actually be -9 mmHg.This negative value means that the fluid is moving in the opposite direction i.e. back intothe capillaries |
|
|
|
describe the Pulmonary vs Systemic Circulation
|
The pulmonary circulation – increases the oxygen content of the blood. The systemic circulation – decreases the oxygen content of the blood. |
|
|
|
both the polmonary and systemic circulation recieve an amount of blood equal to the |
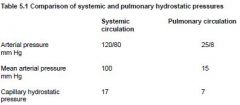
cardiac output, however the pulmonary circuit is much shorter and pressures in the pulmonary circulation are much lower |
|
|
|
what are the 3 reasons for the lower pressure in pulmonary circulation? |
1. The pressure in the right ventricle which forces blood through thepulmonary semilunar valve into the pulmonary artery is less thanthat in the left ventricle which forces blood through the semilunaraortic valve into the aorta. 2. The pulmonary artery and its branches are wider than the aorta andits branches. 3. The pulmonary vessels have thinner, less elastic walls so there isless resistance to blood flow. |
|
|
|
The exchange of fluid between capillaries and the interstitium dependson the |
relative magnitudes of a number of opposing forces |
|
|
|
Forces producing the outward movement of fluid from the blood are... |
1. The hydrostatic pressure of the blood.
2. The oncotic pressure (osmotic pressure) of proteins in the interstitium. 3. A negative interstitial pressure. |
|
|
|
Forces producing a movement of fluid into the blood are.. |
1. The oncotic pressure (osmotic pressure) of proteins in theinterstitium. |
|
|
|
Normally only small amounts of plasma proteins leak out of the bloodbecause they are |
large molecules |
|
|
|
where do large molecules leak out of more? |
Slightly more of the large mlecules leak out of pulmonary capillaries than capillarieselsewhere.
|
|
|
|
In contrast, water and salts |
exchange freely between the blood andinterstitial fluid. |
|
|
|
A lymph pump system is mainly responsible for |
negative interstitialpressure. |
|
|
|
In the lungs there is normally very little interstitial fluid as... |
as it is efficientlyremoved by the lymph pump and by evaporative loss in expired air. |
|
|
|
If oedema fluid accumulates in the interstitium then this may... |
force water into the alveoli |
|
|
|
The air in the alveoli is separated from the blood in the alveolarcapillaries by what 4 things?
|
1. A single layer of Type I and Type II alveolar epithelial cells andalveolar macrophages that form the wall of the alveoli. The Type IIalveolar cells produce surfactant. 2. Basement membrane of the alveolar epithelial cells. 3. Basement membrane of the endothelial cells which line thecapillaries. 4. A single layer of endothelial cells of the capillary (endothelium). |
|
|
|
when does Pulmonary oedema increase the diffusion distance?
|
when fluidaccumulates in the interstitium and separates the basementmembranes. |
|
|
|
what are the key features of the pulmonary microcirculation?
|
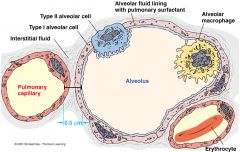
The key features of the pulmonary microcirculation are:1. The pulmonary capillaries (and the alveoli) have very thin wallswhich minimises the barrier to diffusion. 2. In the alveolar walls, the capillaries form a dense network which is acontinuous thin film of blood. This provides a large capillary surfacearea. 3. The pressures in the pulmonary circuit are much lower than in thesystemic circulation and the pulmonary vascular resistance is verylow. The pressure is just sufficient to perfuse the apical areas ofthe lungs in the erect healthy adult. |
|
|
|
what is Not a very useful tool clinically because it is not possible tomeasure all six of the unknown values? |
starling forces |
|
|
|
are Bedside determination of the interstitial hydrostatic and oncoticpressures possible? |
Bedside determination of the interstitial hydrostatic and oncoticpressures is not possible. |
|
|
|
The clinician is limited to assessments based on plasma proteinconcentrations as an indicator of |
capillary oncotic pressure. |
|
|
|
A chest X ray is more useful in |
assessing and monitoringpulmonary oedema and the fluid build up in the lungs. |
|
|
|
Three stages of Pulmonary Oedema are: |
Stage 1:
Fluid transfer is increased into the lung interstitium; because lymphaticflow also increases, no net increase in interstitial volume occurs. Stage 2: The capacity of the lymphatics to drain excess fluid is exceeded andliquid begins to accumulate in the interstitial spaces that surround thebronchioles and lung vasculature. Stage 3: As fluid continues to build up, increased pressure causes it to track intothe interstitial space around the alveoli.Fluid first builds up in the periphery of the alveolar capillary membranesand finally floods the alveoli |
|
|
|
During stage 3 the x-ray picture of alveolar pulmonary edema isgenerated and gas exchange becomes |
impaired. Additionally gravity exerts an important influence on the fluid mechanicsof the lung. |
|
|
|
Under normal circumstances more perfusion occurs at the lung basesthan at the apices; however, when pulmonary venous pressures riseand when fluid begins to accumulate at the lung bases the blood flow |
begins to be redistributed toward the apices |
|
|
|
Changes Leading to Pulmonary Oedema include: |
- Increased hydrostatic pressure of pulmonary capillary blood. - Damage to the alveolar capillary membrane. - Damage to the alveolar epithelial cells. - Damage to the endothelial cells lining the pulmonary capillaries. - Decreased plasma protein concentration. - Block of pulmonary lymphatics. - Pulmonary emboli. These changes may be due to problems with the heart(CARDIOGENIC) or other causes (NON-CARDIOGENIC) |
|
|
|
cardiogenic pulmonary oedema is maindly die to |
an increase in hydrostatic pressure of pulmonarycapillary blood secondary to left heart failure. |
|
|
|
In Cardiogenic Pulmonary Oedema The oedema fluid is...
|
plasma protein poor in comparison to noncardiogenicpulmonary oedema. |
|
|
|
in Cardiogenic Pulmonary Oedema it Involves the formation of fluid due to |
due to increases in plasmahydrostatic pressure or reduction in lymph drainage. |
|
|
|
Non-Cardiogenic Pulmonary Oedema involve |
Disorders that cause leakiness of the alveolar-capillary membraneare often associated with inflammation. |
|
|
|
symptoms of Non-Cardiogenic Pulmonary Oedema |
- near-drowning experience - mechanical ventilation using positive pressureand high tidal volume. - Pulmonary emboli. |
|
|
|
- near-drowning experience - mechanical ventilation using positive pressureand high tidal volume. - Pulmonary emboli. all cause |
These disorders cause ARDS. |
|
|
|
Non-Cardiogenic Pulmonary Oedema Involves |
endothelial damage by bacterial toxins or mechanicalforces. - This causes an immune response and fluid is plasma proteinrich. |
|