![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
59 Cards in this Set
- Front
- Back
- 3rd side (hint)
|
1. What is the prevalence of palpable and non-palpable thyroid nodules in adults? 2. How often are thyroid nodules malignant? 3. What is the percentage of malignant surgically excised nodules? 4. Why should an ultrasound be done on a palpable nodule? |
1. palpable: 4-7% non-palpable: 20-70% 2. <5%!!!! 3. 45-56% 4. 20% are subcentimeter on ultrasound (may not meet biopsy criteria) |
|
|
|
1. What nodule feature allows the patient to avoid FNA and why? 2. How does one identify the above feature? 3. Regarding incidental thyroid nodules, what imaging features caries a high risk of malignancy and warrants an FNA? |
1. hot/hyperfunctioning nodule (~5% of all nodules); they are rarely malignant 2. serum thyrotropin level (TSH) and if low followed by a radionuclide thyroid scan to confirm a "hot" nodule 3. PET avid nodules |
|
|
|
1. What are the advantages of palpation and US guided thyroid FNAs? 2. In which two situations should US-guided be used? 3. What gauge needles and why? 4. What is the dwell time of each pass? |
1. Palpation: reduced cost and logistical efficiency US-guided: certainty the nodule of interest is aspirated, reduced unsatisfactory FNAs, improved accuarcy 2. Nodule with cyst component >25% and nodules previously FNAd with unsatisfactory results 3. small 25 or 27 because the thyroid is so vascular 4. 2-5 seconds with rapid oscillations (3/sec) |
|
|
|
1. What number of passes is commonly recommended per nodule? 2. What histologic alterations occur due to FNA? 3. What are the advantages to thinlayer preparations? 4. Discuss two stain options and the advantages of each. |
1. 2-6 2. infarction of nodule (10%), pseudoinvasion, vascular proliferation and cytologic atypia 3. reduced blood ease in preparation of consistently well-fixed slides shorter screening time due to concentrated specimen 4. Romanowsky: air dried, good for extracellular material (colloid and amyloid) and cytoplasmic detail (granules) Papanicolaou: fixed, better nuclear features including inclusions, grooves and especially chromatin texture |
|
|
|
SEE TABLE 10.1 ON PAGE 269 FOR THYROID BETHESDA REPORTING |
SEE TABLE 10.1 ON PAGE 269 FOR THYROID BETHESDA REPORTING |
|
|
|
1. For what reasons is a thyroid FNA nondiagnostic? 2. What are the adequacy criteria? 3. What is the purpose of the size requirement in the above criteria? 4. What are the exceptions to the above criteria? 5. What is the frequency of nondiagnostic results? |
1. obscuring blood overly thick smears air drying of alcohol fixed smears 2. 6 groups of benign, well visualized follicular cells with each group composed of at least 10 cells 3. to allow determination (by evenness of nuclear spacing) of macrofollicles versus microfollicles 4. abundant colloid (even without enough follicular cells!) When a specific diagnosis can be rendered (e.g. Hashimito thyroiditis) Any atypia 5. 2-30% (macrophages only 15-30%) |
|
|
|
1. What is the malignancy rate for nondiagnostic and cyst fluid only cases? 2. How often is a repeat FNA (done for previously nondiagnostic specimen) diagnostic? 3. What percent of persistently nondiatnostic nodules are malignant? 4. What percent of thyroid FNAs are benign 5. What is the false negative rate for a benign cytology result? |
1. non-diagnostic (excluding CFO): 1-4% cyst fluid only: 4% 2. 50-88% 3. 10% 4. 70% 5. <1-3% |
|
|
|
1. What percent of patients receive a diagnosis in the suspicious category? list the subcategories and their risk of malignancy. 2. What percent of FNAs are classified as malignant and what is the most common diagnosis? 3. What are the two most common causes of false negative diagnoses? 4. What is the false positive rate for a malignant diagnosis? 5. What two tumors are responsible for false positives? |
1. 10-15% suspicious for follicular neoplasm: 15-30% suspicious for follicular neoplasm; hurthle cell type: 15-30% suspicious for malignancy: (subclassified into PTC, medullary, metastatic, lymphoma) 60-75% 2. 3-7% PTC! 3. PTC> follicular carcinoma 4. 1-3% 5. Follicular adenomas (including those with follicular hyperplasia) and hyalinizing trabecular tumors |
|
|
|
1. What 3 categories are considered "indeterminate" FNA categories to clinicians? 2. What testing modality is available to further classify these cases? 3. What is the most promising single marker and why? 4. What other markers are available? What is their PPV and NPV? 5. Name and describe another company and their test. |
1. Atypia of undetermined significance/follicular lesion of undetermined significance (AUS/FLUS) suspicious for follicular neoplasm suspicious for malignancy 2. Molecular tests! 3. BRAF seen in 44% of PTCs and almost NEVER in benign thyroid nodules 4. H-,K-,N- RAS point mutations and RET/PTC or PAX/PPARgamma rearrangments with NPV of 94% and PPV of 88% (Asuragen's Invorm Thyroid Panel) 5. gene expression classifier (Afirma/Veracyte) is optomized to detect benign nodules with a NPV of 95% for AUS, 94% for suspicious for follicular neoplasm and 85% for suspicious for maglinancy |
|
|
|
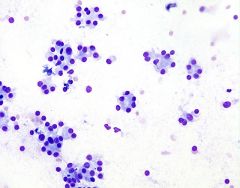
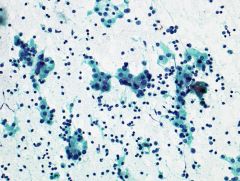
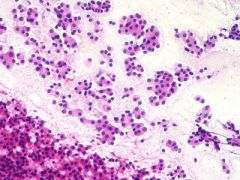
1. Describe the different appearances of colloid. 2. Describe the general findings of benign and neoplastic thyroid nodules. |
1. watery, thin and translucent; thick and opaque with sharp outlines; extremely thick and sticky "bubble gum" colloid 2. benign: high colloid:follicular cell ratio, low cellularity, with macrofollicles or fragments of them seen as flat sheets with evenly spaced follicular cells neoplastic: highly cellular with significant architectural atypia including cell crowding and overlap and formation of abnormal microfollicles, trabeculae or papillae |
|
|
|
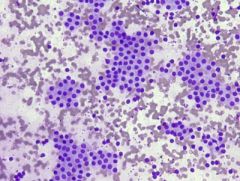
microfollicular archictecture 1. Describe this finding. 2. In what category should predominantly pattern be put? |
1. small circles of crowded follicular cells 2. Suspicious for follicular neoplasm or follicular variant of PTC |
|

|
Papillary architecture 1. Describe a papillae. 2. Of what lesion are these highly characteristic? 3. Why is examination of a slide on high magnification particularly important? |
1. abnormal cells surrounding a fibrovascular core often with a branching pattern 2. PTC of course 3. examination of nuclear changes of PTC because they can be subtle or incompletely displayed |
|
|
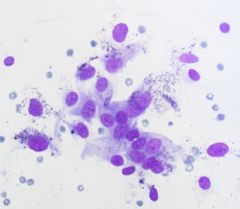
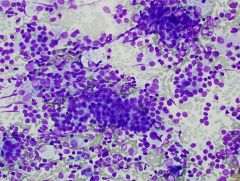
Hurthle cells 1. What is the diagnosis in the photo? 2. AKA? 3. Describe the formation of hurthle cells. 4. Describe the cytomorphology. 5. What pattern, while nonspecific, is almost never seen in benign nodules or PTC? List the entities. |
1. lymphocytic thyroiditis 2. oncocytes or oxyphilic cells 3. metaplastic follicular cells characterized by abundant mitochondria 4. polygonal with abundant finely granular cytoplasm that is green/orange on pap and smooth pale purple on romanowsky, nuclei may be enlarged and pale +/- nucleoli 5. predominantly noncohesive, isloated cells seen in lymphocytic thyroiditis, medullary carcinoma, hurthle cell neoplasms, poorly differentiated carcinoma, undifferentiated (anaplastic) carcinoma and lymphoma |
|
|
1. What are the most common benign thyroid nodules? 2. What patient population is most affected by one of the above? 3. How common is one of the above in the US? 4. How fast on average does the above grow? |
1. multinodular goiter (MNG) and follicular adenoma representing 70% 2. MNG is 5-15% more common in women 3. MNG prevalance is 4-7% in US which is less than iodine deficient areas 4. Nodules in MNG grow 4.5% per annually |
|
|
|
1. What is the histologic determination of MNG nodules? 2. What is different form MNG about follicular adenomas? 3. What are 3 histologic patterns seen in adenomas? 4. List other very uncommon patterns. 5. Which pattern is diagnosed as benign on FNA? |
1. adenomatous or adenomatoid which are NOT encapsulated 2. They are usually solitary (1-3cm in diameter but can be much larger), with a well defined fibrous capsule, with morphologically distinct follicular cells compared to normal thyroid 3. macrofollicular, microfollicular and trabecular 4. FA with papillary hyperplasia (kids/teens), SRC FA, mucinous FA, lipoadenoma, clear cell FA, and FA with bizzare nuclei 5. macrofollicular |
|
|
|
Benign follicular nodule 1. What is the recommended followup? 2. What is the cytomorphology? |
1. exams at 6-18 month intervals for 3-5 years 2. predominantly macrofollicles (fragmented flat sheets or intact spheres) low to moderate cellularity cohesive cells uniform evenly spaced cells coarse chromatin abundant colloid hurthle cells (minor component) macrophages and cyst lining cells |
|
|
1. What color is hemosiderin on pap and romanowsky stains? 2. Describe thick and watery colloid on smears and liquid based preps. 3. What colors does colloid stain? |
1. Golden brown on pap and dark blue on romanowsky 2. Thick: Smear: dense blobs wtih hyaline texture hard edges and cracking artifact LBP: similar to above Watery: more common!! Smear: thin, coverin large areas as a translucent film with bubbles, folds, cracks and circular "chicken wire" artifact LBP: folded tissue paper 3. pap: pale blue, pink ,pale green or orange Romanowsky: magenta or dark blue |
|
|
|
cyst lining cells 1. Describe these. 2. What is the DDX of benign follicular nodule? |
1. usually a minor population of elongated large cells with pale and grooved nuclei with a streaming, tissue culture arrangement, resembling reparative epithelial cell changes 2. suspicious follicular nodule suspicious hurthle cell nodule PTC |
|
|
1. What percent of follicular adenomas are aneuploid? 2. What molecular alteration is relatively specific for follicular carcinoma that is almost never seen in adenomas, MNG or PTC? 3. What is the drawback to the above? 4. When should the diagnosis of suspicious for hurthle cell neoplasm be used? |
1. 25% making DNA quantitation by flow cytometry not useful 2. t(2;3) resulting in PAX-8/PPARgamma gene fusion 3. Low sensitivity, only 26% by FISH 4. When the sample is exclusively composed of hurthle cells particularly when many isolated cells are present |
|
|
|
Chronic lymphocytic thyroiditis 1. AKA? 2. What is the patient population? 3. What is the ultrasound appearance and lab findings? 4. What autoantibodies are most commonly found? 5. What is the cytomorphology? |
1. Hashimoto thyroiditis 2. 95% women peak indicence between 40-60 years 4. anti thyroid peroxidase (microsomal antigen) and anti thyroglobulin 5. mixed population of lymphocytes tingle body macrophages lymphohistiocytic aggregates hurthle cells +/- follicular cells (with occasional mild nuclear pallor and grooves) scant colloid |
|
|
1. What is the DDX of Hashimoto thyroiditis? 2. Which patient population is affected by primary thyroid lymphoma? 3. What types of lymphoma are seen? 4. When is flow cytometry recommended and why? |
1. reactive lymph node MNG with prominent hurthle cell changes primary thyroid lymphoma hurthle cell neoplasm PTC 3. Extranodal marginal zone lymphoma or DLBCL or a mix of the two 4. in the right clinical context and morphology only (rapid growth, large nodule, monomorphic or atypical lymphoid population) because Hashimoto can contain clonal B-cell subpopulations that are NOT lymphoma (but are kappa/lambda restricted or have IgH rearrangement on PCR) |
|
|
|
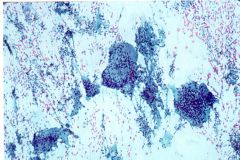
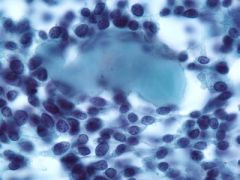
Subacute thyroiditis 1. AKA? 2. What is the cytomorphology? 3. What is the clinical presentation and natural history? |
1. de Quervain thyroiditis 2. multinucleated giant cells rare granulomas lymphocytes 3. painful enlargement of the gland due to granulomatous reaction damaging follicles, self limited lasting several months |
|
|
1. Describe the cells that characterize de Quervain thyroiditis. 2. What is the "hallmark" feature of this disease and what is the pitfall? 3. What is the cytologic DDX? |
1. Multinucleated giant cells are prominent and numerous. They are very large with bizarre angular shapes and densely granular rather than vacuolated cytoplasm, sometimes with ingested colliod droplets 2. granulomas, HOWEVER are rare and difficult to find 3. sarcoidosis, tuberculosis |
|
|
|
1. How does Riedel disease manifest and what is the major DDX? 2. What is the main DDX and how are the two differentiated? |
1. unknown cause, with hard thyroid mass clinically mimicking undifferentiated (anaplastic) carcinoma; dense fibrosis replaces thyroid and extends into the surrounding structures 2. the fibrosing variant of hashimoto's thyroiditis which is excluded with clinical correlation and becauue Reidels lacks germinal centers, hurthle cells |
|
|
|
Amyloid goiter 1. What is the patient population? 2. What appears very similar to amyloid? explain the difference. 3. What thyroid cancer is often accompanied by amyloid? |
2. colloid! amyloid contains stretched and distorted fibroblast nuclei 3. Medullary carcinoma! |
|
|
1. What is black thyroid and what is the cause? 2. Describe the cytomorphology. 3. What stain highlights these cells and what implication does that make? |
1. striking dark brown pigmentation of the thyroid follicular cells in patients on long term tetracycline antibiotics (e.g. minocycline) 2. abundant dark brown pigment granules within the cytoplasm of follicular cells, darker than hemosiderin 3. Fontana masson stain; the pigment may be a type of melanin |
|
|
|
1. What two types of radiation are used as treatment regimens and for what disease? 2. What cytmorphologic changes can the above cause? 3. What is the DDX? 4. What other treatments can cause similar changes in follicular cells? |
1. External: low dose for benign diseases and high does for malignancies like Hodgkins Systemic 131 iodine: treats hyperthyroidism (e.g. graves, MNG, funtioning thyroid carcinoma) 2. sheets (macrofollicle fragments) enlarged cells with normal N:C ratio hurthle cell change cytoplasmic vacuolization marked nuclear atypia (size variation, hyperchromasia, smudged chromatin, grooves, pseudoinclusions, naked nuclei) 3. follicular carcinoma PTC anaplastic carcinoma 4. methimazole and carbimazole used to treat Graves disease |
|
|
|
1. Which diagnostic terms regarding follicular lesions worse than benign nodules? 2. What does it imply? 3. How does this category differ from other thyroid lesions? |
1. suspicious for a follicular neoplasm and follicular neoplasm 2. a nodule with significant architectural alterations of follicular cells raising the possibility of follicular carcinoma which triages the patient for surgery 3. It's diagnostic of other categories (PTC, hashimoto) but is considered a screening test for follicular carcinoma |
|
|
|
1. How common is follicular carcinoma? 2. List three differentiated thyroid carcinomas. 3. How does follicular carcinoma behave compared to PTC? 4. What are the subtypes of follicular carcinoma? 5. What proportion of "suspicious for follicular noeplasm" will be malignant? Name the tumors. |
1. second most common malignant thyroid cancer at 10-15% 2. PTC, hurthle cell carcinoma and follicular carcinoma 3. More aggressively with tendency to metastasize to lungs and bones >> regional lymph nodes 4. minimally invasive (excellent prognosis) and widely invasive (poor prognosis) 5. 15-30%; 55-67% are follicular variant of PTC and others follicular carcinoma |
|
|
|
1. What percent of cases reported as "suspicious for follicular neoplasm" will be non-neoplastic? 2. Why would a patient with follicular carcinoma need a total thyroidectomy? |
1. 35% will be adenomatoid nodules in MNG 2. because any residual thyroid tissue will collect the 131Iodine in the uptake studies instead of the metastases for which they are really looking! |
|
|
|
Suspicious for follicular neoplasm 1. What is the cytomorphology? 2. Which cases are excluded from this category? 3. What is the DDX? 4. What variant of follicular carcinoma is indistinguishable from other metastatic tumors? Name them. |
1. marked cellularity prodominantly microfollicles and/or trabeculae enlarged crowded overlapping follicular cells scant colloid 2. those with nuclear features of PTC 3. benign follicular nodule PTC parathyroid adenoma/carcinoma 4. clear cell variant and RCC and parathyroid tumors |
|
|
Suspicious for follicular neoplasm, hurthle cell type 1. How common is this? 2. With what is this variant associated that typical follicular carcinoma is not? 3. What is an unusual change sometimes seen in the colloid of these cases? 4. What percent of cases are non-neoplastic on excision? 5. What percent of cases are malignant neoplasms? |
1. 3-4% of all thyroid cancers 2. 30% have lymph node metastases! 3. basophilic transformation with concentric calcification resembling psammoma bodies 4. 10-26% non-neoplastic usually MNG or Hashimoto thyroiditis 5. 15-45% malignant and the remainder are adenomas |
|
|
1. What is the cytomorphology of a hurlthe cell neoplasm? 2. In an effort to reduce unnecessary lobectomies, what stricter cytologic criteria have been suggested? 3. What is the DDX? 4. What cells are ABSENT in this diagnosis? |
1. pure hurthle cell population noncohesive cells prominent nucleolus pseudopsammoma bodies 2. additional (to the above criteria) cytologic (small or large cell dysplasia) and architectural (crowding marked dyshesion) abnormalities 3. Hashimitos MNG macrophages PTC metastatic RCC medullary carcinoma parathyroid adenoma/carcinoma granular cell tumor 4. Abundant lmphocytes and normal follicular cells |
|
|
|
1. What features of hurthle cells suggests neoplasm versus reactive? 2. Which preparation can make hurthle cells resemble other cells? which ones and why? 3. When can one downgrade to a diagnosis of AUS (with a comment) in this setting? 4. How can medullary carcinoma be distinguished? |
1. Monomorphism and macronucleoli 2. LBP, the hurthle cells resemble macrophages because their granular cytoplasm appears microbacuolated (pseudovacuolization) 3. If the nodule is small <2.5cm and the patient has Hashimoto because it is likely a hyperplastic nodule OR in a patient with multiple nodules (likely to represent hurthle cell transformation in adenoamtoid nodule) 4. Medullary has no nucleoli and the cytoplasmic granules are red on romanowsky stain whereas hurthle cells are blue and medullary is calcitonin positive |
|
|
|
1. How common is PTC? 2. What is the patient population? 3. What is the reason behind the characteristic nuclear grooves and pseudoinclusions? 4. What type of metaplasia is common within these tumors? |
1. the most common thyroid malignancy accounting for 80% of all thyroid cancers 2. 4:1 female to male ratio usually between 20-50 years (does occur in kids though) 3. PTC cells have profound change in the nuclear skeleton making them less stiff and more deformable 4. Squamous |
|
|
|
1. What is the most common PTC variant and what is notable about is histologic findings? 2. List other variants with brief descriptions. 3. Which two are more agressive? |
1. follicular which has NO papillary structures 2. macrofollicular oncocytic Warthin-like (strongly associated with Hashimotos) clear cell diffuse sclerosing (young adults, abundant squamous metaplasia and psammoma bodies) tall cell (3x tall as wide) columnar cell solid cribriform (FAP/Gardner syndrome) with faciitis like stroma 3. tall cell and columnar |
|
|
|
1. For what immunostains are PTCs reactive? 2. List molecular alterations found in this tumor? 3. What is the prognosis for patients with PTC? |
1. keratins, thyroglogulin, TTF-1 and PAX-8 2. RET/PTC chimeric onncogene resulting from rearrangements of RET on chromosome 10q11.2 rearrangements of TKR gene point mutations in RAS point mutations in BRAF 3. excellent, thyroidectomy is often curative , 10 year survival >90% |
|
|

|
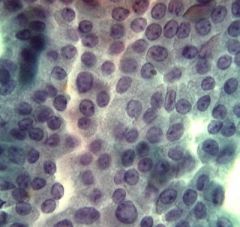
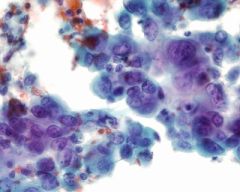
PTC 1. What is the cytomorphology? 2. Which variant is likely to have squamoid morphology that may confuse the diagnosis? 3. What "abnormal" collagen is associated with PTC? |
1. sheets papillae microfollicles (follicular variant) nuclear changes (powdery chromatin, grooves, pseudoinclusions, nucleolus, membrane thickening and irregularity) nuclear crowding/molding variable cytoplasm (scant, squamoid, hurthle like or vacuolated) psammoma bodies histocytes and multinucleated giant cells 2. diffuse sclerosing 3. "bubble gum" colloid with abnormal viscosity that may form long strands or dense blobs |
|
|
1. Hos common are psammoma bodies in PTC? 2. Which variant has the most numerous psammoma bodies? 3. How are the above different from dystrophic nonspecific calcifications? 4. What is a significant cause of false negative diagnoses in PTC? 5.Which two benign lesions also contain psammoma bodies? |
1. seen in 50% of resected tumors 2. diffuse sclerosing 3. PTC psammoma bodies are laminated 4. cystic degeneration 5. MNG and hurthle cell |
|
|
Tall cell variant PTC 1. What cytologic features suggest this tumor? 2. What other aggressive variant can be recognized and how? 3. What is the DDX of PTC? 4. Which variant of PTC is particularly difficult to distinguish from a benign follicular nodule? |
1. PTC nuclei plus abundant elongated granular cytoplasm and prominent nucleoli resembling huthle cells 2. Columnar cell due to elongated columnar cells with scant cytoplasm and crowded cigar shaped nuclei 3. benign follicular nodule follicular neoplasm hashimoto thyroiditis I131 treatment effect cyst lining cells hyalinizing trabecular adenoma 4. macrofollicular variant |
|
|
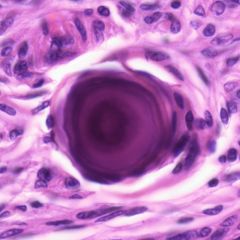
1. What are findings that indicate nonspecific nuclear holes rather than the characteristic pseudoinclusions of PTC? 2. What is hyalinizing trabecular adenoma? 3. What are cytologic clues to the above diagnosis? 4. What are histologic clues to the above diagnosis? |
1. small, not sharply etched, white (rather than color of cytoplasm) and irregular in shape 2. a rare controversial entity that may be a variant of PTC, which has all the nuclear features 3. whorling, parallel array of elongated cells, amorphous hyaline material (not amyloid!), cytoplasmic yellow bodies (green with pap stain), and perinucleolar clear zone 4. encapsulation, marked intratrabecular hyalinization and trabecular architecture |
|
|
|
1. What is the treatment for a diagnosis of suspicious for PTC? 2. What is the PPV of a malignant diagnosis? 3. What are the 3 major groups of thyroid malignancies? |
1. Resection! and 60-75% prove to be PTCs while the rest are usually follicular adenomas 2. 97-99% 3. well differentiated (PTC, follicular hurthle cell) poorly differentiated undifferentiated (anaplastic) |
|
|
|
1. Describe the poorly differentiated category of thyroid cancers. (PTDCs) 2. How common are they? 3. How do these patients present and what is the prognosis ? |
1. in between the well and anaplastic based on intermediate degree of nuclear and architectural atypia 2. account for 4-7% of thyroid carcinomas 3. commonly with nodal, pulmonary, and bone metatases; prognosis is between the other two categories (much worse than well differentiated) with a 5 year survival of 50% |
|
|
|
1. What are the three principal histologic patterns of the PDTCs? 2. Which immunostains are positive in this group? 3. What is the cytomorphology? |
1. insular, trabecular and solid 2. TTF-1 thyroglobulin and PAX-8 3. highly cellular noncohesive trabeculae, microfollicles or solid spheres monomorphous round nuclei mitoses, necrosis |
|
|
|
PDTC insular type 1. What stain is used to support a diagnosis of PDTC and why? 2. What tumor does this most resemble and what are differences in the cytomorphology and IHC? |
1. KI67 because in well differentiated tumors the MIB1 index is <10% whereas in PDTC it's 10-30% 2. Medullary thyroid carcinoma but PDTC has microfollicles with colloid and are thyroglogulin + and calcitonin - |
|
|
Anaplastic thyroid carcinoma 1. How common is this and what is the prognosis? 2. Describe the histologic features. 3. How often are these associated with a differentiated thyroid cancer? 4. What is the IHC profile? |
1. <5% of malignant thyroid tumors and is one of the most rapidly fatal of ALL cancers, accounts for >50% of thyroid cancer related deaths 2. spindle and epithelioid cells mixed with pleomorphic or ostoclast type giant cells with extensive necrosis and mitoses (MIB-1 index >30%) +/- neutrophilic component 3. 1/3 of cases 4. + keratins and PAX-8 - TTF-1 and thyroglogulin! |
|
|
1. What is the 5 year survival rate for anaplastic carcinoma? 2. What is the cytomorphology? 3. What is the DDX? |
1. 0-15% 2. many noncohesive cells large cells epithelioid or spindle shaped marked nuclear pleomorphism (irregular membranes, macronucleoli clumped chromatin) multinucleated giant cells (both pleomorphic tumor type and osteoclast type) 3. atypia of cyst lining cells I131 treatment effect medullary thyroid carcinoma sarcoma metatatic carcinoma |
|
|
|
1. What distinguishes cyst lining atypia from undifferentiated carcinoma? 2. How common is primary SQC of the thyroid? |
1. the nuclei of cyst lining cells while enlarged have smooth nuclear membranes, fine chromatin and small nucleoli 2. <1% of thyroid cancers |
|
|
|
1. How common is medullary thyroid carcinoma? 2. What are the cells of origin and what is their function? 3. In what two forms and patient populations does this occur? |
1. accounts for 5-10% of thyroid cancers 2. parafollicular C cells (rather than follicular cells) that secrete calcitonin which regulates calcium 3. sporadic: 80-90%, average age 50 years MEN syndrome: kids |
|
|
|
1. What percent of MTC secrete calcitonin? 2. List and describe 2 types of MEN syndrome in which theses tumors occur. 3. What percentage of patients with MTC present with regional mets? |
1. 90% 2. MEN 2a: Sipple sydrome, MTC, pheochromocytoma and parathyroid adenoma or hyperplasia MEN 2b: mucosal neuroma syndrome, MTC, pheochromocytoma, multiple mucosal neuromas and marfanoid habitus 3. up to 50% |
|
|
|
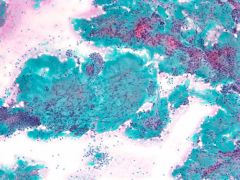
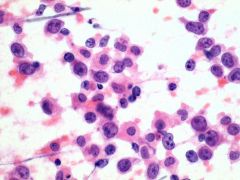
Medullary thyroid carcinoma 1. What is the histologic appearance 2. How often are amyloid deposits present in this tumor? 3. For which stains is MTC positive and negative? |
1. highly variable, sheets, nests or ribbons and cells can be polygonal round plasmacytoid or spindled. the nuclei can be round or oval and do NOT have prominent nucleoli 2. 80% 3. calcitonin, TTF-1, CEA and chromogranin and thyroglobulin negative |
|
|
1. What is the treatment for MTCs? 2. What is the cytomorphology? 3. What type of stain is needed to see the characteristic cytoplasmic feature? |
1. total thyroidectomy with lymph node dissection 2. numerous noncohesive cells or loose clusters epithelioid, plasmacytoid, and/or spindled cells nuclei rounded or elongated with granular chromatin and inconspicuous nucleoli, pseudoincusions in 50%, multiple nuclei red cytoplasmic granules (70% of cases) amyloid 3. Romanowsky to see red granules |
|
|
|
1 What stain is used to definitively identify amyloid and what is the appearance? 2. What is the DDX of MTC? 3. What metastatic tumor can be particularly hard to differentiate form MTC? 4. How should calcitonin stain? |
1. congo red shows apple green dichroism with polarized light 2. undifferentiated carcinoma hurthle cell neoplasm PTC PDTC metastatic tumor 3. melanoma! 4. Cytoplasmic |
|
|
|
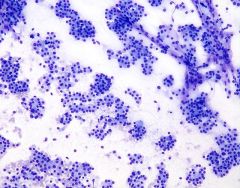
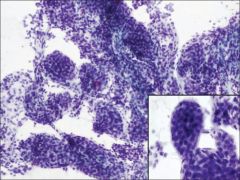
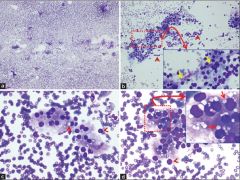
DLBCL of the thyroid 1. How common is primary thyroid lymphoma? 2. In what patient population is it seen? 3. Describe the clinical setting for the above patients. |
1. 5% of thyroid cancers 2. older aged women almost always in the setting of Hashimoto thyroiditis (RR is 40:1 while for general population it is 80:1) 3. a rare complication of hashimoto arising 20-30 years after onset at a mean age of 65yrs |
|
|
1. What are the 3 general categories of thyroid lymphoma? 2. What is the cytomorphology? 3. What is the main DDX? |
1. extranodal marginal zone B cell lymphoma DLBCL mixture of the above two 2. Extranodal marginal zone: small lymphoid cells, centrocytes, plasma cells monocytoid B cells with interspersed large lymphoid cells DLBCL: large lymphoid cells, centroblasts, immunoblasts, Burkitt like cells 3. Hashimoto thyroiditis |
|
|
|
1. What are the most common metastases to the thyroid and how common are they? 2. How often are thyroid metastases the first manifestation of an occult malignancy? 3. For what findings is the category AUS/FLUS reserved? |
1. lung, esophagus, breast and kidney; 0.1-0.3% of thyroid aspirates 2. 25-50% 3.cells (follicular, lymphoid or other) that have architectural and or nuclear atypia that is more marked than benign but insufficient to be classified as suspicious for follicular neoplasm, suspicious for malignancy or malignant |
|
|
|
1. What is often a factor in AUS/FLUS cases? 2. List 9 AUS cytomorphologic patterns. 3. How often is AUS diagnosed and what is the target range? 4. What is the malignancy risk for AUS nodules? |
1. compromised specimen 2. a. Sparsely cellular with a predominance of microfollicles b. Sparsely celluar with a predominance of hurthle cells c. Interpretation of atypia hindered by prep artifact d. Cellular hurthle sample in patient with Hashimoto or MNG e. Focal nuclear atypia but otherwise benign f. Atypical cyst lining cells g. Focal marked anisonucleosis h. Atypical lymphoid infiltrate i. Other 3. 2-29% with a goal of <7% 4. 5-15% |
|
|
|
SEE TABLE 10.2 ON PATE 292 FOR AUS CYTOMORPHOLOGIC PATTERNS |
SEE TABLE 10.2 ON PATE 292 FOR AUS CYTOMORPHOLOGIC PATTERNS |
|
|
|
Parathyroid 1. What is the cytromorphology of a parathyroid lesion? 2. For what is this tissue often mistaken? 3. What clinical finding can help differentiate a parathyroid lesion? 4. What IHC is helpful? |
1. cellular with cohesive sheets, ribbonlike cords and occasional microacini, and/or isolated cells and naked nuclei, with nuclei having coarse chromatin and small prominent nucleoli, with abyndant granular cytoplasm with intracytoplasmic vacuoles 2. follicular lesions of thyroid. 3. hypercalcimia 4. thyroglobulin and PTH |