![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
25 Cards in this Set
- Front
- Back
|
Unilateral hypertransradiance |
By anatomy: Wall: Mastectomy, Polands, Polio Pleura: Ptx Lung: Compensatory hyperexpansion, air trapping, bullae, Swyer James (post bronchiolitis), CLE Vascular: Pulmonary embolus |
|
|
Bilateral hypertransradiant |
Lungs: Emphysema, asthma, acute bronchiolitis (1 y/o), tracheal stenosis Heart: Oligaemia from congenital heart disease Vascular (pruning): PA stenosis, multiple PEs, PAH |
|
|
Unilateral Increased density |
Undisplaced mediastinum: Consolidation, Supine pleural effusion, Malignant pleural mesothelioma Displacement away: Pleural effusion, Diaphragmatic hernia Displacement towards: Collapse, Pneumonectomy, Lymphangitis (usually bilat, symmetrical, LNs, effusions), Agenesis, Hypoplasia |
|
|
Intrinsic tracheal/bronchial narrowing, stenosis occlusion |
From above to below: * Subglottic stenosis: Post-intubation, Wegener's * Tracheal cancer * Tracheobronchomalacia (end-expiration >70% narrowing) * Diffuse inflammatory: Sarcoid, Wegener's, relapsing polychondritis * Foreign body * Carcinoid/lung cancer. |
|
|
Extrinsic tracheal/bronchial narrowing, stenosis occlusion |
By anatomy: Lymph nodes Mediastinal tumours Enlarged LA Aortic aneurysm Anomalous origin left pulmonary artery from right pulmonary artery |
|
|
Organising pneumonia |

Infectious and non-infectious causes. Peripheral unilateral/bilateral patchy consolidation, often migratory. Subpleural/peribronchial distribution. Nodules, masses, ground-glass. May have bronchial wall thickening
|
|
|
Eosinophilic pneumonia |
Reverse pulmonary oedema (peripheral). Non-segmental, upper zones. |
|
|
Lobar pneumonia causes |
Strep: Most common. Klebsiella: Multilobar. Cavitation. Staph: Children. Pneumatoceles common. Empyema. TB: More common in primary. Strep Pyogenes. |
|
|
Bulging fissures |
Abundant exudates: Klebsiella, Strep, Myco. Abscess. Cancer. |
|
|
Unilateral pulmonary oedema |
Same side as pre-existing abnormality: lateral decubitus, aspiration, contusion, thoracocentesis, bronchial obstruction Contralateral: PA absence/hypoplasia, McLeod, PE, lobectomy, unilateral emphysema |
|
|
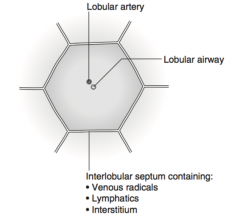
Pulmonary lobule |
|
|
|
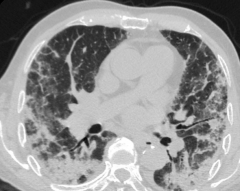
Alveolar proteinosis |
P = Crazy paving (smooth thickening of interlobular/intralobular septa in geographical areas of ground glass). |
|
|
Multiple small opacities (2-5 mm) |
* Disseminated cancer * Subacute hypersensitivy: centrilobular nodules, GG, thin-walled cysts. * Respiratory bronchiolitis: looks like hypersensitivity, but smoking related. * Lymphoma * Sarcoid * Multifocal pneumonia |
|
|
Multiple large pulmonary nodules |
V: AVMs I: Abscesses, Histo, Hydatid, RA nodules (Caplans) T A: Wegener's M: I: Sarcoid, Organising pneumonia N: Mets, Synchronous primaries |
|
|
Non-thrombotic pulmonary emboli |
* Septic: Endocarditis, lines * Catheter embolism * Fat * Air * Amniotic fluid * Tumour * Talc: drug users * Hydatid |
|
|
Calcification |
Localised: TB/histo/coccido In nodule: Cancer, Mets (OSarc, CSarc, mucinous adenocarcinoma colon/breast, papillary thyroid) Interstitial: Dissem ossification (branching, seen in eg busulphan, IPF, asbestos) Diffuse: Infection (TB, varicella), mitral stenosis, silicosis, mets, alveolar microlithiasis, lymphoma post Rtx |
|
|
Exotic causes of pleural effusion |
V: PE I: TB, mycoplasma T: Trauma, Postop, Asbestosis (may be sole) A: SLE, RA M I N: Bronchial CA, Mets, recurrence, Mesothelioma, Lymphoma |
|
|
Unilateral elevated hemidiaphragm |
Above diaphragm: Phrenic palsy, lobar collapse, splinting (eg rib fractures), hemiplegia, pleural disease (eg haemothorax) Diaphragmatic: Eventration, rupture Below diaphragm: subphrenic abscess |
|
|
Rib lesion with mass |
V I: TB TAMI N: Cancer, Mets, Myeloma, MesoT, Lymphoma, Fibrosarc, Neurofibroma |
|
|
Chest radiograph following trauma |
Anatomically. Soft tissues: Foreign bodies, Surgical emphysema Ribs: Simple fracture, flail Sternum: Fracture, SC dislocation Spine: Fracture Pleura: Ptx/haemotx Lung: Contusion, Lac, Haematoma, Aspiration, Oedema, ARDS, Fat embolism Trachea: Lac Diaphragm: Rupture Mediastinum: Aortic injury, haematoma, oesophageal rupture |
|
|
Signs of aortic injury |
* Widening of mediastinum * Abnormal aortic contour * Tracheal displacement to right * NGT displacement right of T4 * Thickening of R paraspinal stripe * Depression L mainstem bronchus * Loss of definition of AP window |
|
|
Drug induced lung disease |
There is a list in Chapman. |
|
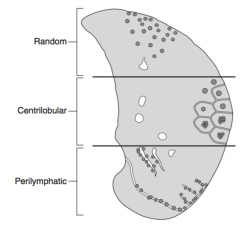
Nodules classification |
Centrilobular: > 5 mm from pleural surfaces, may be close to small vessels. Perilymphatic: Close to pleural surfaces, large vessels, interlobular septa Random. |
|
|
Mediastinal mass containing fat |
Teratodermoid Lipoma (rare) Liposarcoma: may have calcium. Thymolipoma: young ppl. Hamartoma |
|
|
Mediastinal cysts |
Congenital: bronchogenic, enteric, neuroenteric Pericardial cyst Thymic cyst Cystic tumours: lymphangioma, teratoma, teratodermoid Abscess Haematoma |