![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
102 Cards in this Set
- Front
- Back
- 3rd side (hint)
|
Cell |
Basic building block of all living things, all body functions depend on the integerity of cells |
|
|
|
Pathophysiology |
the systemic study of functional changes in cells, tissues, and organs altered by disease and or injury |
|
|
|
Mitrochondria |
Where ATP is produced |
|
|
|
ATP |
Energy production-requires adaquate oxygen to produce |
|
|
|
Ribosomes |
Responsible for protein synthesis and enzyme synthesis |
|
|
|
Nucleus |
Where all the genetic information is contained, largest organell, primary function is cell division |
|
|
|
golgi apparatus |
A refining plant; directs traffic, packages ribosomes into vesicles |
|
|
|
What are some descriptors of human cells? |
Highly complex Most have high metabolic rates |
|
|
|
Oxidative Phosphorylation |
major means of energy production, occurs in mitochondria |
produces ATP |
|
Basement membrane |
All cells bound together by |
|
|
|
What dose a basement membrane allow? |
Provides a pathway for diffusion of nutrients and other water soluble molecules between the blood and tissue cells |
|
|
|
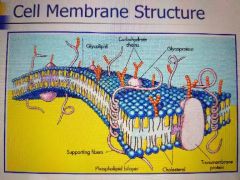
Phospholipid bilayer |
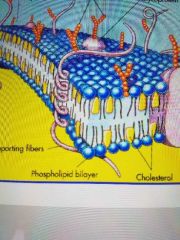
Has a phosphorus head (blue circles) and a lipid tail (yellow white part between the two levels) |
|
|
|
Phospholipid layer contains what 2 parts? |
hydrophobic and hydrophilic |
Water loving and water hating |
|
|
Phosphorus is hydrophilic, true or false? |
True |
|
|
|
If the phospholipid bilayer is made up of a hydrophilic and a hydrophobic layer what does that mean? |
Water cannot easily diffuse through the membrane |
|
|
|
Plasma membraine |
Insoluable to most molecules that dissolve in water, because of the lipid layer |
|
|
|
Are oxygen and carbon dioxide lipid soluble? |
Yes, so they exchange readily through the lipid layer |
|
|
|
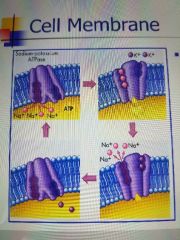
Active transport |

Used to control the concentration of ions, intracellular and extracellur (ICF vs ECF); Na, K, amd Ca |
|
|
|
Active transport requires what? |
Energy, ATP from Oxidative phosporylation |
|
|
|
Oxidative phosphorylation uses what to produce energy? |
carbs, fats and protein |
|
|
|
Anaerobic glcolysis |
Less efficenct energy production when not enough O2 to do oxidative phosphorylation. Takes place in the cytoplasm |
|
|
|
What is a byproduct of anaerobic glycolysis? |
pyruvic acid which turns into lactic acid |
|
|
|
Lactic acid produces what? |
Muscle cramps |
|
|
|
Is cellular injury reverible? |
Depends on how entensive the injury is, but can be irreversible |
|
|
|
Necrosis |
results in an inflammatory process |
|
|
|
Apotosis |
Programmed cell death, normal cell death. Occurs in pathologic and physiologic states |
|
|
|
Apotosis is mangaged by? |
The DNA in our cells and and does not produce any inflammation |
|
|
|
Physiologic example of apoptosis? |
endometrium after pregency and breast size during lactation |
|
|
|
pathologic atrophy example of apoptosis? |
prostate shrinks after castration |
|
|
|
key difference about Apoptosis? |
Cell death without inflammation, so not damaging to the rest of the body |
|
|
|
Charactristics of a apoptosis cell death? |
genetically controlled program inherented in any nucleated cell in the body when activated leads to a well ordered sequence of events that leads the the descruction of the cell without damaging any surround tissue |
|
|
|
Causes of cell injury? |
Ischemia Hypoxia physical agents (trauma, temp extremes, etc) chemicals and drugs microbiologic agents immunologic reactions genetic defects nutiritional imbalances |
|
|
|
Free radicals |
Also called Activated oxygen species, injurious to cells, cause an inflammatory process, and may cause some cells to die |
|
|
|
Additional mechanisms of cell injury? |
ATP depletion O2 depletion generation of too many free radicals loss of Ca homeostasis Defects of plasma membrane permeability mitocondrial damage |
|
|
|
Free radicals definition |
extremely unstable, highly reactive chemical species with a single unpaired electron. |
|
|
|
What can free radicals damage? |
The lipid portion of the membrane |
|
|
|
Common causes of free radicals? |
Ionizing radiation Normal phiological reactions Metabolism of exogenous (anything not made in the body) chemicals |
|
|
|
Free radical degradation is |
Unstable with spontaneous decay; and Vit A, C and E are antioxidants block the formation of free radicals |
|
|
|
Ischemic injury key points |
REVERSIBLE W/IN LIMITS aerobic and anerobic energy production halted cells produce free radicals that are not rapidly degraded INJURES TISSUES FASTER THAN HYPOXIA |
|
|
|
Hypoxic injury key points |
REVERSIBLE W/IN LIMITS switch to anaerobic glycolysis which leads to decrease ATP, increase lactic acid, decrease in glucose stores. Low pH + low ATP = ribosomes detach from endoplasmic reticulum, which wreaks havoc and cells can begin to die |
|
|
|
Ribosome detachement results in |
decreased protein synthesis |
|
|
|
Results of ischemic and hypoxic injury |
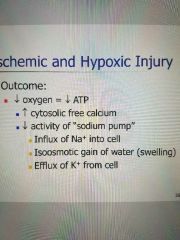
Decrease in O2=Decrease in ATP Increased calcium within the cell outside the mitochondria, wreaks havoc and can result in celluar death. Decrease activity of the Na pump (Na in the cell, K out of cell, causes cell to swell) |
|
|
|
What are the sources and effect of increase cytosolic calcium? |
Sources: mitochondria, endoplasmic reticulum (ER), interstitial fluid external to the cell Effect: activates intracellular enzymes |
|
|
|
How can you tell if some is an enzyme? |
If it ends with an "ASE" it is an enzyme |
|
|
|
Mechanicsms of irreversible injury: |
Inablility to reverse mitochondrial dysfuntion Profound disturbances in membrane function is a central factor |
|
|
|
Irreversible cell injury if followed by? |
Necrosis (sequence of morphologic changes that follow cell death in living tissue) enzumatic digestion of cell; then inflammatory process will occur |
|
|
|
Characteristics of cellular aging |
Reduced mitochondrial function reduced synthesis of structrual, enzymatic and receptor proteins diminished capacity for nutrient uptake dimished capacity for DNA repair |
|
|
|
Cellular aging |
normal wear and tear of life |
|
|
|
Theories of aging |
Excess production of free radicals Inability to naturally remove radicals at a sufficient rate Radicals cause cell and tissue damage |
|
|
|
Can adaptation happen under normal circumstances? |
Yes, adaptation can happen as both normal or abnormal changes, both physiologic and pathologic |
|
|
|
Atrophy (definition) |
shrinkage in size of cell by loss of cell substance |
|
|
|
Results of atrophy |
diminished cell function, organ atrophy, Apoptosis |
|
|
|
Atrophy can be caused by |
biochemical mechanisms (decreased synthesis of cell materials and/or increased cell catabolism-breaking down of the cell) histologic (cell) changes- decreased cell size, increased autophagic vacuoles within the cell. Normally autophagic vacuoles contain debries to prevent damage to the cell |
|
|
|
Additional causes of atrophy |
Decreased workload loss of innervation loss of endocrine stimulation diminished blood supply inadequate nutrition aging |
|
|
|
Hypertrophy |
Increased size of cells and size of organ without in increase in the number of cells. Prominent in organs incapable of mitosis (such as the heart). Increased synthesis of structural proteins and nuclear DNA, increased organelles within the cells |
|
|
|
Example of physiologic hypertrophy |
Skeletal muscles-like gaining muscle mass from excercise |
|
|
|
Example of pathologic hypertrophy |
myocardium in HTN, CHF, HLH, etc |
|
|
|
Causes of hypertrophy |
Increased functional demand Specific hormonal demand (as in pregnancy) |
|
|
|
Hyperplasia |
Increase in the number of cells in an organ or tissue; can ofter occur wih hypertophy |
|
|
|
Causes of physiologic hyperplasia |
Hormonal-like breasts during pregnancy compensatory-after a partial hepatectomy your liver with partially regenerate due to pyerplasia |
|
|
|
pathologic causes of hyperplasis |
Psoriasis, endometriosis, BPH |
|
|
|
Is hyperplasis cancerous? |
No, but can be a fertial soil for cancer |
|
|
|
Metaplasia |
A reversible change where one adult cell type is replaced by another adult cell type. Often a protective mechanism but can lead to cancers later. New cells are better able to withstand enviromental stress |
|
|
|
Examples of metaplasia |
Gastric metaplasia-d/t chronic GERD Squamous metaplasia-d/t smoking |
|
|
|
Dysplasia (definition) |
Deranged cell growth with loss of uniformity of cells. Changes in size, shape, or organization of mature cells |
|
|
|
Dysplasia is caused by |
chronic irritation, inflammation, hormone stimulation |
|
|
|
Dysplasia is a non-neoplastic (non-tumor) proliferation, true or false? |
True, may or may not progress to cancer |
|
|
|
Dysplasia is often caused from |
chronic irriation/inflammation |
|
|
|
Pleomorphism |
Many different types and shapes, for dysplasia |
|
|
|
How is dysplasia graded? |
Mild, moderate, severe, carcinoma-in-situ |
|
|
|
Which dysplasia's are potentially reversible? |
mild to moderate, need to remove inciting stimulus |
|
|
|
Neoplasia |
New growth, uncontrolled. Can indicate cancer, but not necessarily |
|
|
|
Benign and malignant describe what |
the biological behavior of the tumor |
|
|
|
Biological behavior is characterized by |
Degree of differentiation of the tumor Rate of growth Rate of cell death |
Regarding tumors |
|
|
Benign tumors mean |
remain localized, won't spread, more ammenable to surgical removal |
|
|
|
Types of benign tumors |
Fibroma-Fibrous tissue tumor Lipoma-fat tissue tumor Adenoma-glandular tumor chondroma-cartilaginous tumor Leiomyoma-smooth muscle tumor |
|
|
|
Malignant |
adhere's to and destroys adjacent structures |
|
|
|
Examples of malignant tumors |
Sarcoma Carcinoma Lymphoma |
|
|
|
What does differentiation tell us |
The more the resemble (well-differentiated) they are to their cell of origin the better. The more agressive neoplasms are those that are poorly differentiated or undifferentiated, can't tell what they were |
|
|
|
anaplasia |
Undifferentiated cells, feature of most malignant tumors Cellular pleomorphism (lots of different types of cells), hyperchormatic nuclei-increased variation in size and shape of nuclei, high nucleus to cytoplasm ratio, bizarre nuclei, and giant cells |
|
|
|
In general benign and well-differerntiated tumors grow |
slowly. Exceptions can be made depending on blood suply, site, and hormonal stimulation |
|
|
|
In general, Malignant and poorly differentiated tumors grow |
fast. Exceptions can be made depending on blood suply, site, and hormonal stimulation |
|
|
|
How do benign tumors usually grow |
by slow expansion, but may be lethal depending on location |
|
|
|
Malignant tumors usually grow by |
infiltrating and may destroy surrounding tissue |
|
|
|
What does a metastasis indicate |
malignancy |
|
|
|
Metastasis (defination) |
discontinuous spread of the tumor |
|
|
|
Methods of metastasis spreading |
seeding-invading a natural body cavity lymphatic spread hematogenous (blood) |
|
|
|
ABC's of skin lesions |
A= Asymmetrical B= Borders (uniform better) C= Color (uniform better) D= Diameter >6mm needs to be looked at |
|
|
|
Morbidity and mortality factors |
Metastases Rupture into major vessels compression of vital organs organ failure infection |
|
|
|
What are 3 pathways for inclusions to build up in the body? |
Can't metabolize fast enough, something is slowing the metobolism down, or we lack the the process/enzyme to metabolize it out |
|
|
|
Endgenenous inclusions |
Normal or abnormal substance cannot be metabolized (storage dz) Normal substance produced at normal or increased rate of metabolism inadaquate for removal (fatty liver) |
|
|
|
Steatosis |
Fatty change in liver |
|
|
|
Causes of Steatosis |
ETOH abuse, toxins, anoxia, obesity, DM, protein malnutrition |
|
|
|
How does steatosis progress |
Excess hepatic triglycerides, they exceed capacity of liver to form lipoproteins; defect in any of the 6 steps to the livers function will lead to accumulations of lipids |
|
|
|
Signs of steatosis |
Liver-increased weight, yellow color fat vacuoles within cytoplasm of hepatocytes |
|
|
|
Atherosclerosis |
Macrophages and smooth muscle cells filled with fat vacuoles |
|
|
|
Xanthomas |
Accumulations of cholesteral in the skin, often around the eye, often genetic |
|
|
|
Exogenous inclusion examples of inclusions |
Black lung (anthracosis) |
|
|
|
Hemosiderosis |
Systemic iron overload, mainly in the cells of the liver, pancreas, heart and endocrine organs |
|
|
|
Gout |
Defect in purine metabolism Causes hyperuericemia, or high levels of uric acid in the blood. Can be due to high production of uric acid, abnormal retention of uric acid or both. Uric acid becomes insoluble and forms crystals that deposit in various joints |
|
|
|
Dystrophic calcification |
Occurs with normal serum Ca, but an absence of calcium metabolism. Deposits occur in areas of necrosis or injury and can be intracellular or extracellular |
|
|
|
Metastatic calcification |
Occurs with hypercalcemia, hyperparathyroidsim, bone catabolism w/ bone tumors, Vit D intoxication, renal failure. Affects vessels, kidneys, lungs, gastric mucosa |
|