![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
89 Cards in this Set
- Front
- Back
|
How do you analyze arterial blood gas values? |
1. pH - acidosis vs. alkalosis 2. CO2 3. HCO3 |
|
|
What does the CO2 value tell you? |
- If it is high, the patient either has respiratory acidosis (pH <7.4) or is compensating for metabolic alkalosis (pH >7.4) - If it is low, the patient either has respiratory alkalosis (pH >7.4) or is compensating for metabolic acidosis (pH <7.4) |
|
|
What does the HCO3 value tell you? |
- If it is high, the patient either has metabolic alkalosis (pH >7.4) or is compensating for respiratory acidosis (pH <7.4) - If it is low, the patient either has metabolic acidosis (pH <7.4) or is compensating for respiratory alkalosis (pH >7.4) |
|
|
True or false, the body does not compensate beyond a normal pH? |
True - for example, a patient with metabolic acidosis will eliminate CO2 to help restore a normal pH If respiratory alkalosis is a compensatory mechanism (and not a rare, separate primary disturbance), then the pH will not correct to greater than 7.4 Over-correction does not occur! |
|
|
What are the common causes of respiratory acidosis? |
- COPD - Asthma - Drugs (e.g., opioids, benzos, barbiturates, alcohol, other respiratory depressants) - Chest wall problems (paralysis, pain) - Sleep apnea |
|
|
What are the common causes of metabolic acidosis? |
- Methanol / ethylene glycol - Uremia - Diabetic ketoacidosis, diarrhea - Propylene glycol - Isoniazid - Lactic acidosis (sepsis, shock, bowel ischemia) - Ethanol - Salicylate / aspirin overdose |
|
|
What are the common causes of respiratory alkalosis? |
- Anxiety - Hyperventilation - Aspirin / salicylate overdose |
|
|
What are the common causes of metabolic alkalosis? |
- Diuretics (except carbonic anhydrase inhibitors) - Vomiting - Volume contraction - Antacid abuse / milk-alkali syndrome - Hyperaldosteronism |
|
|
What type of acid-base disturbance does aspirin overdose cause? |
- Respiratory alkalosis - Metabolic acidosis |
|
|
Aside from the acid-base disturbance, what other signs are associated with an aspirin overdose? |
Coexisting tinnitus, hypoglycemia, vomiting, and history of "swallowing several pills" |
|
|
Treatment for aspirin overdose? |
Alkalinization of the urine with bicarb speeds up excretion (remember metabolic acidosis with respiratory alkalosis |
|
|
What happens to the blood gas of patients with chronic lung conditions? |
Respiratory Acidosis - pH may be alkaline during the day (breathing better when awake) - After an episode of bronchitis or other respiratory disorder, the metabolic alkalosis that compensates is no longer a compensatory mechanism and becomes the primary disturbance (elevated pH and HCO3) |
|
|
What is a long term complication of sleep apnea and other chronic lung conditions? |
Right-sided heart failure (cor pulmonale) |
|
|
Should you give bicarb to a patient with acidosis? |
Almost never - first try IV fluids and correction of underlying disorder; if all other measures fail and pH remains <7.0, bicarb may be given |
|
|
What metabolic disturbance is associated with a patient in an asthma attack? |
Slightly alkalotic due to breathing off CO2 |
|
|
The blood gas of a patient with asthma has changed from alkalotic to normal, and the patient seems to be sleeping. Is the patient ready to go home? Management? |
- This means the patient is probably crashing - pH is initially high in patients with asthma because they are eliminating CO2 - If the pt becomes tired and does not breath appropriately, CO2 will begin to rise and pH will normalize - Eventually pt becomes acidotic and requires emergency intubation if appropriate measures are not taken (fatigue secondary to work of breathing is indication for intubation) * Prepare for possible elective intubation and continue aggressive medical tx with beta-2 agonists, steroids, O2 |
|
|
List the signs and symptoms of hyponatremia? |
- Lethargy - Seizures - Mental status changes or confusion - Cramps - Anorexia - Coma |
|
|
What are the ways to classify hyponatremia? |
- Hypovolemic - Euvolemic - Hypervolemic |
|
|
What are causes of hypovolemic hyponatremia? |
- Dehydration - Diuretics - Diabetes - Addison disease / hypoaldosteronism (high K+) |
|
|
What are causes of euvolemic hyponatremia? |
- SIADH - Psychogenic polydipsia - Oxytocin use |
|
|
What are causes of hypervolemic hyponatremia? |
- Heart failure - Nephrotic syndrome - Cirrhosis - Toxemia - Renal failure |
|
|
How is hypovolemic hyponatremia treated? |
Normal saline |
|
|
How is euvolemic hyponatremia treated? |
Water / fluid restriction |
|
|
How is hypervolemic hyponatremia treated? |
- Water / fluid restriction - Diuretics may be needed |
|
|
How do you treat SIADH? What if first tx fails? |
1. Try water restriction 2. Use Demeclocycline --> induces nephrogenic diabetes insipidus |
|
|
What happens if hyponatremia is corrected too quickly? |
Overly quick correction may cause brainstem damage (central pontine myelinolysis) |
|
|
How can you decrease the risk for central pontine myelinolysis when treating hyponatremia? |
- Hypertonic saline should be avoided unless the pt has seizures from severe hyponatremia, then only briefly and cautiously - NS is better choice 99% of time |
|
|
What is the ideal rate of correction for chronic severe symptomatic hyponatremia? |
0.5 - 1 mEq/L/hr |
|
|
What causes spurious (false) hyponatremia? What does this mean about the amount of sodium? |
- Hyperglycemia - Hyperproteinemia - Hyperlipidemia - The lab value is low, but the total body sodium is normal; do not give extra salt or saline |
|
|
How does hyperglycemia relate to a false hyponatremia?
|
Once glucose is >200 mg/dL, Na decreases by 1.6 mEq/L for each rise of 100 mg/dL in glucose |
|
|
What causes hyponatremia in post-op patients? |
- Most common is combination of pain and narcotics (causing SIADH) with overaggressive administration of IV fluids - Rare cause is adrenal insufficiency; in this instance, K+ is high and BP is low |
|
|
What is the classic cause of hyponatremia in pregnant patients about to deliver? Mechanism? |
Oxytocin, which has an ADH hormone-like effect |
|
|
What are the signs/symptoms of hypernatremia? |
Basically the same as signs/symptoms of hyponatremia: - Mental status change or confusion - Seizures - Hyperreflexia - Coma |
|
|
What can cause hypernatremia? |
- Most common is dehydration (free water loss) - Watch for diuretics, diabetes insidious, diarrhea, renal disease, iatrogenic causes (too much hypertonic IV fluid) - Rare: sickle cell disease (due to renal damage and isosthenuria - inability to conc. urine), hypokalemia and hypercalcemia (impair kidney's concentrating ability) |
|
|
How is hypernatremia treated? |
Water replacement, but pt is often severely dehydrated, so NS is frequently used Once hemodynamically stable, often switched to 1/2 NS Do NOT use D5W for hypernatremia |
|
|
What are the signs/symptoms of hypokalemia? |
- Muscular weakness --> paralysis, ventilatory failure, ileus, hypotension - EKG --> loss of T wave or T wave flattening, U waves, premature ventricular and atrial complexes, ventricular and atrial tachyarrhythmias |
|
|
What is the effect of pH on serum K+? |
- Changes in pH cause changes in serum K+ as a result of cellular shift - Alkalosis causes hypokalemia - Acidosis causes hyperkalemia |
|
|
Why would you give bicarb to a severely hyperkalemic patient? |
Alkalosis causes K+ to go into cells (and can cause hypokalemia) |
|
|
If the pH and K+ level is deranged and you fix the pH, do you need to correct the K+? |
No, usually by correcting the pH the K+ will return to normal too as the K+ is often due to the pH derangement
|
|
|
What is the relationship between digoxin and potassium? How does this affect management of a patient taking digoxin? |
- Heart is particularly sensitive to hypokalemia in patients taking digoxin - K+ levels should be monitored carefully in all patients taking digoxin, especially if they are also taking diuretics (common occurrence) |
|
|
How should K+ be replaced? |
Hypokalemia should be corrected slowly - Oral replacement is preferred, but if K+ must be given IV for severe derangement, do not give more than 20 mEq/hr - Put pt on EKG monitor when giving IV K+ because potentially fatal arrhythmias may develop |
|
|
When hypokalemia persists even after administration of significant amounts of K+, what should you do? |
Check Magnesium - When Magnesium is low, body cannot retain K+ effectively - Correction of Magnesium level allows K+ level to return to normal |
|
|
What are the signs/symptoms of hyperkalemia? |
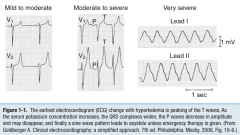
- Weakness and paralysis - EKG --> tall peaked T waves, widening of QRS, prolongation of PR interval, loss of P waves, sine wave pattern - Arrhythmias --> asystole, ventricular fibrillation |
|
|
What are potential causes of hyperkalemia? |
- Renal failure (acute / chronic) - Severe tissue destruction (because K+ has high intracellular conc.) - Hypoaldosteronism (watch for hyperreninemic hypoaldosteronism in diabetes) - Medications (stop K+ sparing diuretics, beta blockers, NSAIDs, ACE inhibitors, ARBs) - Adrenal insufficiency (assoc. w/ low Na+ and low BP) |
|
|
What should you suspect if an asymptomatic patient has hyperkalemia? Management? |
Was the lab specimen hemolyzed - hemolysis can cause a a false hyperkalemia result because of intracellular K+ concentrations REPEAT the test |
|
|
How should you manage an asymptomatic patient that has hyperkalemia (and not due to hemolysis)? |
- Obtain EKG to look for cardiotoxicity - Best tx: decrease K+ intake and administer oral sodium polystyrene resin (Kayexalate) - If K >6.5 or cardiac toxicity (more than peaked T waves), immediate IV therapy needed |
|
|
What should you do if a patient with hyperkalemia has K+ > 6.5 or cardiac toxicity (more than peaked T waves)? |
IV therapy needed immediately: 1. Calcium gluconate - cardioprotective, although it does not change K+ levels 2. Sodium bicarb (alkalosis causes K+ to shift inside cells) 3. Glucose with insulin (insulin forces K+ inside cells and glucose prevents hypoglycemia) - Beta-2 agonists also drive K+ into cells and can be given if other choices are not listed - If pt has renal failure (high Cr) or initial tx is ineffective, prepare to institute emergent dialysis |
|
|
What are the signs/symptoms of hypocalcemia? |
- Neurologic findings --> tetany - Chvostek sign - Trousseau sign - Depression - Encephalopathy - Dementia - Laryngospasm - Convulsions / seizures - EKG --> QT interval prolongation |
|
|
What is Chvostek sign? |
Tapping the facial nerve at the angle of the jaw elicits contraction of the facial muscles |
|
|
What is Trousseau sign? |
Inflation of a tourniquet or BP cuff elicits hand muscle (carpopedal) spasms |
|
|
What EKG finding is associated with hypocalcemia? |
QT interval prolongation |
|
|
What should you do if the calcium level is low? |
- Remember hypoproteinemia (low albumin) of any etiology can cause hypocalcemia because the protein-bound fraction of calcium is decreased ** First check albumin and/or the ionized or free calcium level to make sure "true" hypocalcemia is present |
|
|
How will a patient present who has low calcium due to hypoproteinemia? |
Asymptomatic because the ionized (unbound, physiologically active) fraction of calcium is unchanged |
|
|
How do you correct hypocalcemia for hypoalbuminemia? |
For every 1 g/dL decrease in albumin below 4 g/dL, correct the calcium by adding 0.8 mg/dL to the given calcium value |
|
|
What causes hypocalcemia? |
- DiGeorge syndrome - Renal failure - Hypoparathyroidism - Vitamin D deficiency - Pseudohypoparathyroidism - Acute pancreatitis - Renal tubular acidosis |
|
|
How does a patient with hypocalcemia due to DiGeorge syndrome present? |
Tetany 24-48 hours after birth; absent thyme shadow on x-ray |
|
|
How does renal failure lead to hypocalcemia?
|
Kidneys are involved in vitamin D metabolism which is essential for calcium absorption
|
|
|
How does a patient with hypocalcemia due to hypoparathyroidism present? |
Post-thyroidectomy patient; all four parathyroids may have been accidentally removed |
|
|
How does a patient with hypocalcemia due to pseudohypoparathyroidism present? |
Short fingers, short stature, mental retardation, normal levels of parathyroid hormone with end-organ unresponsiveness to parathyroid hormone |
|
|
What is the relationship between low calcium and low magnesium? |
It is difficult to correct hypocalcemia until hypomagnesemia (of any cause) is also corrected |
|
|
How does pH affect calcium levels?
|
Alkalosis can cause symptoms similar to hypocalcemia through effects on the ionized fraction of calcium (alkalosis causes calcium to shift intracellularly) |
|
|
What is a common scenario to explain alkalosis presenting with symptoms of hypocalcemia? |
Hyperventilation / anxiety syndrome --> pt eliminates too much CO2 --> alkalosis --> premolar and extremity tingling Treat by correcting pH; reduce anxiety if hyperventilation is the cause |
|
|
What is the relationship between calcium and phosphorus? |
- Phosphorus and calcium levels usually go in opposite direction (when one goes up, the other goes down) - Derangements in one usually cause problems with the other |
|
|
Clinical significance of inverse relationship between calcium and phosphorus levels? |
Pt with chronic renal failure, in whom you must not only try to raise calcium levels (with vitamin D and calcium supplementation), but also restrict / reduce phosphorus |
|
|
What are the signs / symptoms of hypercalcemia? |
Often asymptomatic and discovered by routine lab test When symptomatic, remember - "Bones, Stones, Groans, Psychiatric Overtones": - Bones: osteopenia, pathologic fractures - Stones: kidney stones, polyuria - Groans: abdominal pain, anorexia, constipation, ileus, nausea/vomiting - Psychiatric overtones: depression, psychosis, delirium/confusion |
|
|
Abdominal pain and hypercalcemia may be associated with what? |
- Abdominal pain can be caused by hypercalcemia - Peptic ulcer disease (increased incidence with hypercalcemia) - Pancreatitis (increased incidence with hypercalcemia) |
|
|
What ECG finding is associated with hypercalcemia? |
QT interval shortening |
|
|
What can cause hypercalcemia? |
- Hyperparathyroidism (most common out-patient) - Malignancy (most common in-patient) - Vitamin A or D intoxication - Sarcoidosis - Thiazide diuretics - Familial hypocalciuric hypercalcemia - Immobilization - Hyperproteinemia |
|
|
Most common cause of hypercalcemia in the out-patient setting? |
Hyperparathyroidism |
|
|
Most common cause of hypercalcemia in the in-patient setting? |
Malignancy |
|
|
How should you first evaluate hypercalcemia? |
Check parathyroid hormone level to differentiate hyperparathyroidism from other causes |
|
|
How do you diagnose familial hypocalciuric hypercalcemia? |
Low urinary calcium, which is rare with hypercalcemia |
|
|
How does hyperproteinemia (high albumin) cause hypercalcemia? |
Increase in protein-bound fraction of calcium, but patient is asymptomatic because the ionized (unbound) fraction is unchanged |
|
|
Why is asymptomatic hypercalcemia usually treated? |
Prolonged hypercalcemia can cause: - Nephrocalcinosis (due to calcium salt deposits in kidney) - Urolithiasis (due to calcium salt deposits in kidney) - Renal failure (due to calcium salt deposits in kidney) - Bone disease (due to loss of calcium) |
|
|
How is hypercalcemia treated? |
1. IV fluids 2. Furosemide (loop diuretic) to cause calcium diuresis Other treatments: - Phosphorus administration (use oral phosphorus; IV administration can be dangerous) - Calcitonin - Bisphosphonates (eg, etidronate, often used in Paget disease) - Plicamycin - Prednisone (especially if malignancy induced) Identify and treat underlying cause |
|
|
Why shouldn't you use thiazide diuretics in a patient with hypercalcemia? |
Thiazide diuretics increase serum calcium levels |
|
|
How do you treat hypercalcemia caused by hyperparathyroidism?
|
Surgery |
|
|
In what clinical scenario is hypomagnesemia usually seen? Why? |
Alcoholism - magnesium is wasted through kidneys |
|
|
What are the signs/symptoms of hypomagnesemia? |
Similar to hypocalcemia - prolonged QT interval on ECG and possibly tetany |
|
|
In what clinical scenario is hypermagnesemia seen? |
- Classically iatrogenic in patients who are pregnant and treated for pre-eclampsia with magnesium sulfate - Renal failure |
|
|
What are the signs/symptoms of hypermagnesemia? |
Sequentially: - Decrease in deep tendon reflexes - Hypotension - Respiratory failure |
|
|
How do you treat hypermagnesemia? |
* Stop magnesium infusion! - Remember ABCs (airway, breathing, circulation) - Intubate patient if necessary - If patient is stable, start IV fluids - Furosemide can be given next if needed, to cause magnesium diuresis - Last resort is dialysis |
|
|
In what clinical scenarios is hypophosphatemia seen? |
- Uncontrolled diabetes (especially diabetic ketoacidosis) - Alcoholic patients |
|
|
What are the signs/symptoms of hypophosphatemia?
|
- Neuromuscular disturbances (encephalopathy, weakness) - Rhabdomyolysis (especially in alcoholics) - Anemia - WBC dysfunction - Platelet dysfunction |
|
|
What is the IV fluid of choice in hypovolemic patients? |
Normal Saline or Lactated Ringer solution (regardless of other electrolyte problems) First fill the tank, then correct the imbalances that the kidney cannot sort out on its own |
|
|
What is the maintenance fluid of choice for adult patients who are not eating? |
1/2 NS + 5% Dextrose Usually KCl 10-20 mEq is added to a L of IV fluid each day to prevent hypokalemia (assuming that patient had a a normal baseline potassium) |
|
|
What is the maintenance fluid of choice for children <10 kg who are not eating? |
1/4 NS + 5% Dextrose Usually KCl 10-20 mEq is added to a L of IV fluid each day to prevent hypokalemia (assuming that patient had a a normal baseline potassium) |
|
|
What is the maintenance fluid of choice for children >10 kg who are not eating? |
1/3 - 1/2 NS + 5% Dextrose Usually KCl 10-20 mEq is added to a L of IV fluid each day to prevent hypokalemia (assuming that patient had a a normal baseline potassium) |
|
|
Should anything be added to the IV fluid for patients who are not eating?
|
Usually KCl 10-20 mEq is added to a L of IV fluid each day to prevent hypokalemia (assuming that patient had a a normal baseline potassium) |