Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
72 Cards in this Set
- Front
- Back
|
what is the obturator sign? what diagnosis is it associated with?
|

a/w appendicitis
obturator sign = pain upon flexion and internal rotation of the hip |
|
|
what is Rovsing’s sign? what diagnosis is it associated with?
|

a/w appendicitis
Rovsing's sign= pain in the RLQ upon palpation of the LLQ |
|
|
Early in the course of acute appendicitis, are vital signs usually abnormal?
|
no - early in its course, vital signs including temperature may be normal. Once perforation has occurred, the rate of low-grade fever (<38 C) increases to about 40%.
|
|
|
what is the psoas sign? what diagnosis is it associated with?
|

a/w appendicitis
psoas sign = pain upon extension of the hip. |
|
|
explain what rebound in the setting of acute appendicitis means
|
Rebound is usually elicited only after the appendix has ruptured or infarcted.
|
|
|
In establishing a differential diagnosis of abdominal pain, the onset of PAIN prior to the occurrence of N/V is more often suggestive of
|
surgical etiology of the pain, such as small bowel obstruction
|
|
|
what bug should you think of in patients with sickle cell anemia who present with abdominal pain and diarrhea?
|
salmonella (not shigellosis)
|
|
|
Radiation of pain to the scapula is suggestive of
|
acute choleycystitis (NOT hepatitis)
|
|
|
Diverticulitis pain is generally located
|
in the LLQ
|
|
|
Describe the pain patterns a/w with peptic ulcer disease (PUD)
|
pain that is worse preceding a meal
non-radiating, burning epigastric pain pain that awakens a patient in the middle of the night relief of abdominal pain with antacids note: unrelenting pain over a period of weeks should suggest an alternative diagnosis |
|
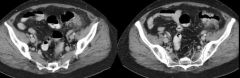
A 78 year old female presents to the E.D. with a sensation of LLQ abdominal pain, accompanied by some irregular bowel movements and loss of appetite. Her abdominal CT (two images) is shown in the Figure. What is the most likely diagnosis?
|
A patient with this general picture is most likely to have diverticulitis, which is revealed on the CT scan as diverticular disease with inflammation (wall thickening and stranding).
|
|
|
A mother brings her 6 week old boy to the emergency room. She states the baby has been vomiting everything she’s tried to feed him for the past 12 hours. She states that he usually eats readily and completes an entire feeding, but he is unable to keep anything down. The emesis is non-bloody and non-bilious, however it is projectile in nature. What is the most likely condition in this patient?
|
pyloric stenosis
The answer is C. Hypertrophic pyloric stenosis typically presents in the second to sixth week of life and is four times more common in males than females. Infants with hypertrophic pyloric stenosis typically are vigorous eaters but shortly afterward regurgitate the entire feeding contents in a projectile fashion. The emesis is non-bilious. The classic finding on exam is an “olive” palpable in the abdomen, and diagnosis is typically via ultrasound. Intussusception typically presents between the ages of 5 and 12 months. Gastroenteritis is characterized by diarrhea as well as vomiting. Neither constipation nor appendicitis typically present with protracted vomiting, though the latter condition tends to present atypically in young children (and elderly adults). |
|
|
46yo F c/o abrupt onset of intermittent severe pain in L flank & abdomen that woke her from sleep. She is pacing & appears extremely uncomfortable. She has never experienced this type of pain previously and denies fevers or other symptoms. Renal calculus is suspected. Some questions -
What is the best diagnostic test (KUB, IVP, Helical CT, U/S)? How helpful is a Urinalysis? |
Helical CT scan is greater than 95% sensitive and specific for renal calculi
Helical CT scan has been shown to be both highly sensitive and specific in the diagnosis of renal calculi. It is the preferred modality for evaluation in many centers. Although urinalysis typically demonstrates hematuria in patients with renal calculi, hematuria is not specific enough to confirm the diagnosis, and imaging is warranted in all first-time presenters. KUB detects approximately 60-70% of calculi (though studies addressing this issue are somewhat methodologically flawed). Ultrasound is not reliable for detecting small calculi, but is 85-94% sensitive and 100% specific at demonstrating hydronephrosis. IVP is contraindicated in patients with renal insufficiency due to the dye load necessary to perform the study. |
|
|
50 yo M p/w 1 day of gradually worsening, intermittent, LLQ pain a/w loose stools. No fevers or bloody bowel movements. Similar sxs in the past were self-limited. Vital signs wnl. PE shows mild tenderness in LLQ, +BS and no masses or peritoneal signs. His PCP can see him tomorrow in his clinic. What should be done next in the E.D.?
|
Discharge home on high-fiber diet, laxatives and stool softeners
This patient has classic diverticulosis (saclike protrusions of colonic mucosa through the muscularis) without signs of acute diverticulitis (inflammation of diverticula). Usually these patients can be managed as outpatients with a high-fiber diet and treatments to decrease intestinal spasm. If the patient develops fever or pain increases he may need further evaluation to rule out abscess formation. Diverticulitis is treated with antibiotics, bowel rest and analgesics. |
|
|
You are treating a 25yoM with the recent diagnosis of Crohn’s disease in the ED. Regarding Crohn’s disease, you know that:
|
There is a small increased risk of colon cancer
Although Crohn’s disease may involve the entire bowel tract, the rectum is rarely involved. Involved areas are typically non-contiguous (known as “skip lesions”) and the inflammation involves all of the layers of the bowel wall--resulting in many of the complications of Crohn’s such as abscess and fistula formation, intestinal obstruction, and perforation. The risk of colon cancer is only slightly elevated above baseline. In contrast, Ulcerative colitis begins in the rectum and may spread to the upper parts of the colon but never involves the small intestine. The ulcerations are contiguous and involve only the colonic mucosa. The incidence of colon cancer may be increased up to 30 times over baseline. |
|
|
53yo obese woman presents to ED, accompanied by three of her children, c/o severe abdominal pain that began this afternoon after lunch. PE reveals marked RUQ tenderness. Likely findings on this patient would include:
|
This woman is likely suffering from acute cholecystitis. Predisposing factors include female gender, obesity, increased age and increased parity. Inflammation of the gallbladder causes RUQ pain and sonographic Murphy’s sign (inspiratory arrest, due to pain, while the ultrasound probe is positioned over the gallbladder). Pain may radiate to the right scapula. Lab studies usually show leukocytosis with or without a left shift, and aminotransferases and bilirubin are usually within normal limits.
|
|

25yo F p/w epigastric pain radiating straight through to the back. Labs are notable only for markedly elevated amylase and lipase. An abdominal X-ray is taken (see Figure). What's the dx?
|
The most likely explanation for her symptoms is gallstone-related pancreatitis
The X-ray reveals stones in the gallbladder. These particular stones are not likely the cause of pancreatitis, but the demonstration of gallstone disease raises the likelihood that the patient’s pancreatitis is indeed due to gallstones. In the U.S., the most common etiologies of pancreatitis include gallstones (45%) and alcoholism (35%). Alcoholic pancreatitis may occur in young patients as well as in older abusers of alcohol. Many other drugs, infectious agents, and conditions are associated with the development of pancreatitis. A few examples include hypertriglyceridemia, trauma, pregnancy, pancreatic carcinoma, atherosclerotic emboli, and scorpion bites. |
|
|
45yo F p/w RUQ pain & fever. The pain is worse after eating. On PE she has a (+) Murphy's sign. Most likely dx?
|
Cholecystitis
RUQ pain, fever and a Murphy’s sign suggests cholecystitis. Cholelithiasis presents with similar pain, but is not associated with fever or a Murphy’s sign |
|
|
47yo M presents, confused, to the ED. He has limited ability to give a history. On PE of the skin, it is noted that there are erythematous changes to both palms. Also, the face and arms are characterized by a number of superficial, tortuous arterioles which fill from the center outwards. The examination of the abdomen reveals violaceous lines radiating from the umbilicus, and there are generally increased venous markings on the abdominal wall (see Figure). What is the most likely diagnosis?
|
liver disease
The patient’s palmar erythema, spider angiomata, and caput medusa (due to recanalization of the umbilical vein) are all characteristic of hepatic disease. The figure demonstrates abdominal wall venous engorgement, as well as ascites (another clue to the patient’s liver disease). |
|
|
A 57-year-old homeless woman with a history of schizophrenia presents to the emergency department complaining of nausea and severe abdominal pain for 48 hours. The patient is not cooperative with an upright abdominal image, so a flat plate (as shown in the Figure) is obtained. Which of the following is the most likely operative finding in this patient?
|
small bowel obstruction
Dilated loops of small bowel with air-fluid levels (which are not well-seen on a flat plate) indicate small bowel obstruction. KUB is not often useful in the diagnosis of appendicitis, ruptured spleen, gallstone disease, or a rectus sheath hematoma (which is an abdominal wall condition most likely seen in anticoagulated patients with trauma or coughing). Despite this woman’s history of schizophrenia and possibly diminished ability to relate a clear story of her pain, her complaint of abdominal pain must be taken seriously with a high suspicion for underlying pathology. |
|
|
All of the following factors predispose to cecal volvulus EXCEPT:
A. marathon running B. pregnancy C. age 25-35 D. prior abdominal surgery E. severe chronic constipation |
constipation DOES not lead to volvulus
Cecal volvulus occurs as a result of abnormal fixation of the right colon and increased mobility of the cecum. Depending on the degree of rotation around the mesenteric axis, cecal volvulus can lead to twisting of the mesentery and its blood vessels. Cecal volvulus occurs most commonly in people 25-35 years old and should be suspected in cases of bowel obstruction without known risk factors. Prior abdominal surgery and pregnancy predispose to obstruction or cecal volvulus; however, chronic constipation is not known to predispose to cecal volvulus. Interestingly, marathon runners have been found to have a higher incidence of cecal volvulus, perhaps from having a thin, flexible mesentery that more easily permits rotation of the cecum around the mesenteric pedicle. |
|

A 57 year old ill-appearing man presents with fever, chills, abdominal pain, nausea and vomiting. His abdominal CT is shown in the Figure. Which of the following is LEAST correct regarding this patient’s condition?
|
Answer: Emergent percutaneous drainage in the emergency department is indicated
The patient has a hepatic abscess, typically caused by gram negatives, anaerobic Streptococci or Entameoba histolytica. Laboratory findings include elevations of WBC, bilirubin, alkaline phosphatase and serum aminotransferases. CXR may demonstrate a right-sided effusion and elevation of the right hemidiaphragm. Treatment with triple coverage antibiotics such as gentamicin, metronidazole and ampicillin should be instituted immediately, however consultation with a general surgeon, interventional radiologist, or gastroenterologist is necessary for definitive treatment, which is drainage of the abscess. |
|
|
Which of the following pairings of referred pain and causal disease is least likely to be encountered?
A. thoracic back pain—pancreatitis B. epigastric pain—myocardial infarction C. inguinal pain—ureteral colic D. shoulder pain—ruptured spleen E. sacral pain—ovarian torsion |
The answer is E. Ovarian torsion may cause lower abdominal pain, pelvic pain, adnexal tenderness, and cervical motion tenderness, but it is not known to cause sacral pain.
|
|
|
A 72 year old man with a history of diverticulosis presents with vague abdominal pain for the past day. His physical exam is notable for normal vital signs, left lower quadrant abdominal tenderness without rebound or guarding, and guaiac positive brown stool. Work-up including KUB and abdominal/pelvic CT scan reveals diverticulitis without perforation. Of the following choices, which is the most appropriate management of this patient?
|
The answer is E. For mild episodes of diverticulitis in which there is no evidence of perforation or peritonitis, there is no indication for immediate surgical intervention. Conservative management with intravenous fluids and antibiotics as well as bowel rest is typically first attempted. Although colon carcinoma may be a precipitating factor in the development of diverticulitis, barium enema should be avoided in the acute period due to high risk of bowel perforation. Although some patients with mild cases of diverticulitis may be discharged home with conservative treatment, the elderly are at higher risk of perforation and should be admitted. Guaiac positive stool in seen in up to 50% of patients with diverticulitis. There is no reason to suspect acute blood loss requiring transfusion in diverticulitis.
|
|
|
Regarding esophageal perforation, which of the following is INCORRECT:
A. Over 90% of spontaneous esophageal perforations occur in the proximal esophagus. B. Over 80% of esophageal perforations are iatrogenic, usually as complications of upper endoscopy, dilation, or sclerotherapy. C. Esophageal perforation has been reported as a complication of nasogastric tube placement, endotracheal intubation, and esophagotracheal Combitube intubation. D. Iatrogenic perforations of the esophagus usually occur in the proximal esophagus or esophagogastric junction. E. Esophageal perforation may result from forceful vomiting, coughing, childbirth or heavy lifting. |
The answer is A. Over 90% of spontaneous esophageal perforations occur in the distal esophagus, whereas iatrogenic perforations are frequently at the pharyngoesophageal junction or the esophagogastric junction. Foreign body or caustic substance ingestion, severe blunt injury or penetrating trauma, and carcinoma are other causes of esophageal perforation.
|
|
|
Working in the ED, you have identified a bony object wedged in the
mid-esophagus of a 45 year old patient. Failure to promptly remove a foreign body impacted in the esophagus could result in: |
Esophageal perforation and mediastinitis
Working in the ED, you have identified a bony object wedged in the mid-esophagus of a 45 year old patient. Failure to promptly remove a foreign body impacted in the esophagus could result in: A. The rapid development of xerostomia B. Epiglottal edema and airway obstruction C. Esophageal perforation and mediastinitis D. Barrett’s esophagitis The answer is C. The complications of esophageal foreign bodies are rare but serious. They include esophageal erosion and perforation, mediastinitis, esophagus-to-trachea or esophagus-to-vasculature fistula formation, stricture formation, diverticuli formation, and tracheal compression (from both the esophageal foreign body and resultant edema or infection). Air trapping is a sign of a foreign body of the airway. Rarely, airway foreign bodies act as one-way valves that could cause hyperinflation of a lung segment, with resultant bleb rupture and pneumothorax formation. |
|
|
A mother brings her 35 year old son to the emergency department because of tremor and mutism for the past three days. His mother found him in his room this morning lying stiffly in his bed, soiled with urine and feces. He appears confused and will not respond to questions. He was diagnosed with schizophrenia last year and has been on several medications. Last month after his most recent hospital admission for schizophrenia, he was discharged with a prescription for haloperidol. On physical exam, he is visibly diaphoretic and has vital signs as follows: T 102.7, BP 140/98, P 112, R 12. His neuromuscular exam shows extremely rigid extremities, and his laboratory values are notable for a white blood cell count of 15000/mm3 and abnormally elevated creatine phosphokinase levels. What is the most likely explanation for these findings?
|
Neuroleptic malignant syndrome (NMS) is an idiosyncratic, life-threatening reaction to antipsychotic medications, with haloperidol being the most common cause. It is characterized by elevated temperatures, "lead pipe" muscle rigidity, altered mental status, choreoathetosis, tremors, and autonomic dysfunction (e.g., diaphoresis, labile blood pressure, incontinence, dysrhythmias). While this patient’s temperature is only 102.7, students should note that any patients with temperatures greater than 105 most likely have non-infectious etiologies for temperature elevation. NMS is thought to be due to too much D2 blockade in the substantia nigra and hypothalamus. Treatment consists of stopping the causative agent and providing supportive care. Medications such as dantrolene, bromocriptine, amantadine, and lorazepam are also often used.
|
|
|
25yo M returns to the ED, 24 hours after being released from the hospital with a new diagnosis of schizophrenia. He has recently started to take haloperidal for his psychotic symptoms. In the ED he is noted to have involuntary contractions of the muscles of the face, a protruding tongue, deviation of the head to one side, and sustained upward deviation of the eyes. Vital signs are stable, and initial labs show no electrolyte or hematological abnormalities. Of the following choices, the preferred medication for this condition is:
|
Tx: diphenhydramine
Acute dystonia, the most common adverse effect seen with neuroleptic agents, occurs in up to 5% of patients. Dystonic reactions, which can occur at any point during long-term therapy and up to 48 hours after administration of neuroleptics in the emergency department, involve the sudden onset of involuntary contraction of the muscles in the face, neck, or back. The patient may have protrusion of the tongue (buccolingual crisis), deviation of the head to one side (acute torticollis), sustained upward deviation of the eyes (oculogyric crisis), extreme arching of the back (opisthotonos), or rarely laryngospasm. These symptoms tend to fluctuate, decreasing with voluntary activity and increasing under emotional stress, which occasionally misleads emergency physicians to believe they may be hysterical in nature. Dystonic reactions should be treated with IM or IV benztropine (Cogentin®), 1 to 2 mg, or diphenhydramine (Benadryl®), 25 to 50 mg. Intravenous administration usually results in near-immediate reversal of symptoms. Patients should receive oral therapy with the same medication for 48 to 72 hours to prevent recurrent symptoms. |
|
|
A 70yo M with acute delirium requires administration of haloperidol for agitation. Which of the following is a recognized side effect of haloperidol?
|
prolonged QT interval
Potential side effects of haloperidol include acute dystonia, prolonged QT interval, Parkinsonism, and akathisia. |
|
|
what's a recognized AE of lithium?
|
Nephrogenic diabetes insipidus
|
|
|
A 19 year old woman is brought to the emergency department by her friends because she has been saying that she is a superhero and trying to run into traffic to prove that she is indestructible. The friends report that she has been using drugs but they do not know which ones. Which of the following pairs of ocular finding and recreational drug is commonly observed?
|
Sympathomimetics (cocaine, amphetamines) cause DILATED pupils.
Opiates (heroin) cause pinpoint pupils. Internuclear ophthalmoplegia is a/w multiple sclerosis. |
|
|
A 42 year old former custodial worker presents stating, “I think that people can hear what I am thinking.” In the emergency department, he becomes extremely agitated and threatening, and his psychoses become more severe. In choosing an antipsychotic medication, which of the following would be the most appropriate choice?
|
Haloperidol
Haloperidol is the most studied high potency antipsychotic agent used in agitated patients. Typical dosing is 5-10 mg IM every 10-30 minutes. Peak serum levels occur in about 30 minutes after IM dosing. Unlike thioridazine, haloperidol does not cause respiratory depression, has negligible anticholinergic side effects, and rarely causes hypotension. Although benzodiazepines can be used in the agitated patient, respiratory depression can occur, and close monitoring is essential. |
|
|
20yo college student is brought to ED by campus police after he was found by his roommate saying people in the TV were trying to kill him. Which of the following criteria is NOT an indication for admission?
A. lacks capacity to cooperate with treatment B. inadequate psychosocial support C. demonstrates risk for suicide D. first-time psychiatric episode |
The answer is D. For an acute psychiatric episode, the first goal is medically stabilizing the patient. Subsequently, a patient who presents without previous history of a psychiatric episode does not necessarily need to be admitted. This, of course, depends on the identity and severity of the condition, and whether it can be treated in the emergency department.
|
|
|
55yo M p/w new onset agitation and confusion. Which of the following PMHx would suggest a psychiatric (non-organic) cause?
A. H/o COPD B. H/o DM only C. H/o hypothyroidism only D. H/o alcohol abuse only |
The answer is C. Although hyperthyroidism may result in an agitated state, hypothyroidism is not generally associated with violent behavior. All other answers are potentially treatable medical problems that could account for the presentation of an agitated or violent patient. After assuring the safety of all parties involved, the emergency department physician should rule out organic causes of agitation.
|
|
|
35yo M is placed on his back on the gurney in physical restraints for violent behavior. Which life-threatening complication can arise?
|
Metabolic Acidosis (not Rhabdo)
Bruises and abrasions are the most common complication of physical restraints. After restraint application, patients need to be monitored frequently and positions changed to prevent neurovascular complications such as circulatory obstruction, pressure sores, and rhabdomyolysis. Positional asphyxia can arise when patients are placed into the prone or hobbled position. Protracted struggle against restraints can promote a significant metabolic acidosis that has been associated with cardiovascular collapse. Patients who continue to struggle with physical restraints should be chemically restrained as well. |
|
|
Which medication is ideal for the agitated or combative patient?
|
Haloperidol
Drugs with a relatively short half-life allow for more careful monitoring of chemically restrained patients. Patients may be given multiple administrations of the restraining agent as needed. Antipsychotics (such as haloperidol) and benzodiazepines (such as lorazepam) exhibit most of these characteristics and are commonly used in combination in the emergency department. The use of 5 mg of haloperidol IV/IM with 2 mg of lorazepam IV/IM, repeated every 30 minutes as needed, is recommended for the combative patient who does not have contraindications to these medications. Half doses should be used in the elderly. |
|
|
19yoM is brought in to ED by EMS after being found obtunded in his apt by a friend. No additional history is available. On arrival, the patient is minimally responsive with sonorous respirations and a palpable rapid pulse. The most appropriate initial diagnostic test would be
|
Fingerstick glucose
Hypoglycemia is a common and readily treatable cause for altered mental status. An ABG is unlikely to be diagnostic and more likely to reflect secondary abnormalities caused by respiratory depression. While a urine drug screen may show positives, it cannot quantitate the amount of a substance or the time period in which the exposure occurred so a positive screen may not reflect cause and effect. An EKG, while a part of a toxicology evaluation, is not an appropriate initiate screening test for an unstable patient until airway and readily reversible causes have been addressed. |
|
|
27yo M is found unresponsive in his car in the hospital parking lot and brought in by security. During your initial evaluation you find him to be cyanotic with pulse ox 82% on room air with a RR of 4 bpm & P120 bpm. Pupils are 1mm bilaterally. Your team is having difficulty finding a vein for an IV line due to extensive scarring of his arms. You are suspicious of an overdose, which medication would you want to rapidly administer as a potential antidote in this situation?
|
Naloxone
The patient has stigmata of an opiate overdose with hypopnea, cyanosis, and miotic pupils. In addition, intravenous drug users often use up their veins. While hypoglycemia can definitely cause a depressed mental status and needs to be assessed, it should not result in respiratory depression or miotic pupils. Thiamine is utilized to prevent Wernicke’s encephalopathy particularly in malnourished patients who present with hypoglycemia but is not an antidote per se. Flumazenil can be used to temporarily reverse the respiratory depression caused by benzodiazepines but also carries with it the risk of precipitating withdrawal and uncontrollable seizures in chronic benzodiazepine users. As a result, it is not recommended for routine use in patients with altered mental status. |
|
|
A 53 year-old known alcoholic presents with agitation, vomiting and altered mental status. His fingerstick glucose is 148. His serum ethanol level is undetectable and his head CT is normal. An ABG shows a pH of 7.21, pCO2 of 34, pO2 of 98 on room air. His basic chemistry panel includes a sodium of 136, potassium 4.1, chloride 108, bicarbonate 14, BUN 12, creatinine 1.1. What substance are you concerned that he may have ingested?
A. Methanol B. Ethylene glycol C. Isopropyl alcohol D. Salicylates |
The answer is C. The patient is presenting with a non anion gap metabolic acidosis. Isopropyl alcohol is metabolized via alcohol dehydrogenase to acetone which accumulates and causes significant ketosis but not an anion gap. Other toxic alcohols such as methanol and ethylene glycol are ultimately metabolized to formic and glycolic acids which cause toxic effects and an anion gap metabolic acidosis. Salicylates result in an anion gap metabolic acidosis with a superimposed respiratory alkalosis. The following mnemonic can be used to recall the common causes of an increased anion gap metabolic acidosis: CAT MUDPILES;
C - cyanide A - alcoholic ketoacidosis T - toluene M - methanol U - uremia D - diabetic ketoacidosis P - paraldehyde I - isoniazid/iron L - lactate E - ethylene glycol S - salicylates Isopropyl alcohol causes a ketosis without an acidosis. |
|
|
In treating hepatitis secondary to alcoholic liver disease... what's an imp pearl to keep in mind?
|
Thiamine first!!!
Thiamine should be administered prior to glucose to avoid precipitating acute Wernicke’s encephalopathy Alcoholics often have low thiamine levels due to poor nutrition, and low glucose levels due to the suppression of gluconeogenesis by alcohol. However, thiamine should always be replaced prior to glucose to avoid the potential complication of precipitating Wernicke’s encephalopathy. Magnesium levels may appear normal on laboratory testing, but alcoholics typically have low magnesium stores and should be given magnesium empirically unless contraindications for magnesium exist. Alcoholics should also be evaluated for gastritis and overall nutritional status and should be referred appropriately. |
|
|
A 45 year old man is brought to the E.D., with markedly altered mental status as reported by someone who stays with him at a homeless shelter. The patient is very confused and obtunded, and unable to provide a cogent history; the person who brought him to the E.D. notes the patient has a “drinking problem.” The patient’s vital signs are normal, except for a respiratory rate of 22. As he lays in the stretcher, his appearance is as depicted in the Figure. Of the following choices, which physical finding is most likely to be present on physical examination?
|
upon elevation of the arms to 90-degrees (in 0-degrees abduction), and pronation of the hands with fingers spread, wrists and interphalangeal joints are characterized by jerky alternations of extension and flexion
This patient has marked ascites (which may incidentally account for his mild tachypnea due to impairment of respiratory excursion). The most likely explanation given the limited information available is liver disease, and asterixis (“liver flap”) as described in choice D is a likely marker of advanced hepatic failure. |
|
|
60yo M p/w new onset confusion. What finding suggests a functional, as opposed to an organic etiology?
|
auditory hallucinations
The other choices (disorientation, abnormal vital signs, acute onset) are all characteristic of organic confusional states. Hallucinations can occur with both organic and functional causes of confusion. Hallucinations associated with organic confusion may be visual, tactile, or auditory. Hallucinations in patients with functional disease tend to be auditory. |
|
|
Delirium is defined as:
|
a global inability to relate to the environment and process sensory input
|
|
|
Delusions are defined as
|
false beliefs that are not amenable to arguments or facts to the contrary
|
|
|
75yo F is brought to ED by a family member with a history of progressive forgetfulness and confusion. She has a history of dementia. The most common cause of dementia in the elderly patient is:
|
Alzheimer's disease
Most dementia is Alzheimer’s type. The second most common cause of dementia is vascular dementia, which accounts for 10 to 20% of all dementias. Primary degenerative dementias include Alzheimer’s disease, vascular dementia, subcortical dementias involving the basal ganglia and thalamus (e.g., progressive supranuclear palsy, Huntington’s chorea, Parkinson’s disease), and Pick’s disease, also known as dementia of the frontal lobe type. Smaller percentages are attributable to causes such as anoxic encephalopathy, hepatolenticular degeneration, tumors, and slow virus infections |
|
|
65yo M is brought to the ED after he was found wandering on the street. He is unkempt and confused. A diagnosis of delirium, rather than dementia, is more likely if which of the following is true?
|
there is a change in the level of consciousness
Patients with delirium have disturbances in consciousness, cognition, and perception. These disturbances tend to occur over a short period of time (hours to days). The delirious patient may be somnolent or agitated. Thought process may be mildly disturbed or grossly disorganized. The clinical presentation may be subdued or explosive, and the course can fluctuate over minutes to hours. The patient’s sleep-wake cycle may be altered or reversed; agitation is often present during the night. An acute confusional state can also be one of the protean manifestations of a metabolic or nutritional abnormality, including hepatic encephalopathy, acute renal failure, and diabetic ketoacidosis or hyperosmolarity. |
|
|
80yo nursing home pt brought to ED with an acute onset of confusion. Which of the following metabolic abnormalities is the most likely explanation?
|
hypernatremia
The differential diagnosis of acute confusional states is lengthy. It includes many metabolic/nutritional abnormalities including hypoglycemia, hypo-/hypernatremia, and hypercalcemia. Hypokalemia alone, however, is not a common cause of altered mental status. |
|
|
Which factor is LEAST reliable in differentiating between organic and inorganic causes of confusion?
A. Presence of attention deficit B. acute versus chronic onset C. Vital sign abnormalities D. Signs of trauma |
Presence of attention deficit
Presence of an attention deficit is common to all confusional states. All the other options may be used to differentiate organic versus non-organic causes of confusion. Characteristics of organic causes include acute onset, abnormal vital signs, fluctuating level of consciousness, possibly signs of trauma, and/or focal neurologic signs. Inorganic (functional) causes commonly illustrate chronic onset, stable vital signs, absence of trauma or focal neurologic symptoms, and/or delusions and illusions. |
|
|
Facts about hypertensive emergencies:
|
Hypertensive encephalopathy is a true medical emergency, and can cause coma and death over hours; however, encephalopathy due to hypertension is more likely reversible than encephalopathy from other causes. Avoidance of overzealous blood pressure lowering is particularly critical for patients with strokes. Laboratory analysis can be important in cases of hypertension in pediatric patients (for whom renal/renovascular or pheochromocytoma may be identified) and in pregnant patients (for whom laboratory testing can help establish diagnoses such as the HELLP syndrome).
|
|
|
29yo F is found seizing by her husband and is rushed to the ED. She is noted to have a BP of 162/112, is still seizing, and looks puffy all over. Her husband tells you that they are expecting their first child in a few months. Which of the following is the next best step in this patient’s care?
|
Control the seizures with magnesium sulfate.
|
|
|
Which of the following is NOT a feature of febrile seizures?
A. generalized tonic-clonic seizure B. duration less than 15 minutes C. a/w a rapid rise in body temperature D. occurs in children ages 3 months to 5 years E. associated with postictal state of 30 minutes |
The answer is E. Febrile seizure is not associated with a postictal period. The child usually rapidly regains alertness. Intracranial mass or infection should be a concern if the duration of seizure is greater than 15 minutes or if altered mental status persists after the cessation of seizure activity.
|
|
|
47yo M w h/o alcohol abuse presents to ED after having a seizure. His past includes both seizures and blackouts. His last alcoholic drink was the previous evening. This morning he experienced palpitations, diaphoresis, and dizziness before losing consciousness and having a seizure lasting under a minute. Which of the following is a true statement with regard to alcohol and its association with seizures?
|
Fact: In people with an underlying seizure disorder, excessive alcohol intake is a risk-factor for seizure due to increased likelihood of head injury, predisposition to metabolic disorders, and lowered seizure threshold.
Fact: Alcohol intake itself can precipitate seizures due to the neurotoxic effects of alcohol and its metabolites. Fact: Cessation of alcohol can precipitate seizures as part of the alcohol withdrawal syndrome (all of the above were true...) |
|
|
A patient with a ventriculo-peritoneal shunt presents to the E.D. with lethargy and vomiting. A CT scan obtained emergently (see the Right image in the Figure) is compared with a CT scan (see the Left image in the Figure) from a month ago. What is the diagnosis?
|
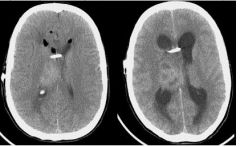
hydrocephalus and shunt malfunction
|
|
|
68yo diabetic male, previously living independently, is brought in by his family. He has been acting abnormally for two days. The family reports he is awake all night and sleepy during the day. He is confused about where he is and the time of day, and sometimes doesn’t recognize his daughter and son-in-law. At other times he appears and acts almost normally.
Which of the following is true regarding his condition? |
Patients can be agitated and combative, or calm and quiet in this condition.
The scenario describes a patient with delirium, a condition in which patients may be agitated and combative, or calm and quiet. The most common cause of delirium in the elderly is medications, accounting for 22-39% of cases. Infection and metabolic abnormalities are other common causes, and delirium may be the first indication that an infection is present. An elderly patient with delirium resulting from an infection may have a normal temperature, a low temperature, or a high temperature. Delirium is characterized by an acute onset of a disturbance in level of consciousness, cognition and attentiveness. It has a fluctuating course, and alterations in sleep-wake cycles are common. Dementia, in contrast, has a slower course, that is gradually progressive over months to years, and consciousness is preserved. In addition to correcting the underlying cause, it is important to minimize stimulation, because the patient with delirium has difficulty processing stimuli. |
|
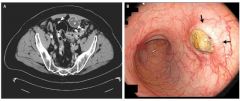
The chest X-ray in the Figure was taken in an intoxicated patient who is conversant, but an unreliable historian. The X-ray findings are best described as indicating:
|
esophageal foreign body
The film reveals a classic appearance of a round foreign body (in this case, a pull-top from a beer can) in the esophagus. The foreign body appears to lie outside the tracheal shadow. There is no sign of mediastinal air (which would be expected with penetrating trauma). The X-ray reveals no signs of mediastinitis, but the risk of esophageal perforation and ultimate mediastinitis prompts endoscopic intervention in this patient. |
|
|
25yo M brought to ED by his family, with a c/o feeling depressed for the past week. In obtaining the history, which of the following statements regarding this patient would support a diagnosis of major depression?
|
The patient has a history of Crohn’s disease
Depression is more common in patients with history of other medical illnesses, some of which may actually cause depressive symptoms. As compared with major depression, dysthymic disorder is a more chronic, and less severe, form of depressive illness. |
|
|
42yo M with end stage liver disease due to chronic hepatitis C infection arrives to the ED in stable condition after an unsuccessful suicide attempt by bilateral wrist laceration. He reports no h/o depression or psych disorder. Aside from his liver disease, for which he takes interferon alpha and ribavirin, he reports that he is in good health and takes no other medications. Which of the following factors increased this patient’s risk of new-onset suicidal ideation?
|
interferon alfa therapy
Interferon alfa, an important cytokine in the early immune response to viral infection, has both antiproliferative and antiviral properties. It is the only therapy approved by the Food and Drug Administration for hepatitis C infection. Interferon alfa has been associated with high rates of central nervous system side effects, including anhedonia, fatigue, anorexia, impaired concentration, sleep disturbance, and suicidal ideation. Clinicians should always look up the side effects of their patients’ medications, especially unfamiliar drugs. This can both expedite diagnosis of drug-induced complications and prevent them with appropriate pretreatment. Pretreatment with a selective serotonin reuptake inhibitor appears to be an effective strategy to minimize depression induced by interferon alfa. Chronic hepatitis C infection and end-stage liver disease can both be difficult diseases to live with, however, these conditions are not known to significantly increase a patients’ risk for new suicidal ideation. Depression is not a known side effect of ribavirin treatment. Although males have a higher percentage of successful suicide attempt than females, females have a much higher incidence of suicide attempt and ideation than males overall. |
|
|
Which clinical scenario is use of chemical restraint indicated?
|
Patient’s behaviors and actions pose an imminent harm to self
|
|
|
Which psychiatric disorders is a/w the greatest increased risk of committing suicide?
|
panic disorder (more than depression, schizophrenia, PTSD)
Most people who commit suicide suffer from either alcoholism or a diagnosable psychiatric illness. 15-20% of people with major depression and 10% of people with schizophrenia will commit suicide. Up to 40% of people with panic disorder will attempt suicide at some point in their lives. PTSD also carries an increased risk. |
|
|
When using the “SAD PERSONS” scale to determine suicide risk, which factor conveys the least amount of points?
|
separated, divorced or widowed
Being separated, divorced or widowed is an important but less significant factor in determining suicide risk and so is assigned 1 point on the suicide scale. All the others are high-risk factors and are each assigned 2 points on the suicide scale. A score of 6 or more has a sensitivity of 94% and a specificity of 71% compared with formal psychiatric evaluation to identify the need for hospitalization in patients who present immediately after a suicide attempt. |
|
|
"Silent Suicide" is defined as:
|
an act of slowly killing oneself by nonviolent means, such as starvation or non-compliance with essential medical treatment
|
|
|
Toxicological screening is indicated in which patient with suicidal ideation?
|
Patient who ingested a “bottle” of tylenol
Routine toxicological screening is unnecessary in the evaluation of suicidal patients in whom there are no clinical indications for such testing. With the exception of acetaminophen, essentially all patients with dangerous overdoses and poisoning will demonstrate clinical signs within several hours of ingestion. History, physical examination, and risk determination of suicide, however, is part of the routine evaluation of the suicidal patient. |
|
|
Suicide risk is increased in this patient population:
|
Patients who are elderly and Caucasian
|
|
|
A 22 year-old man, recently released from hospital with a newly diagnosed psychiatric disorder, was found dead at his home from an overdose of medications prescribed by his doctor. Of the following drugs, which one (taken in isolation), would be most likely to be associated with fatal outcomes in an overdose scenario?
|
amitriptyline
|
|
|
An 18 year old hockey player is hit in the mouth with a puck, fracturing a maxillary canine tooth. He brings the severed piece of tooth with him. On physical exam, the tooth is fractured halfway between the tip and the gumline. The root of the tooth is still firmly intact. The exposed fracture site has a yellowish tinge without blood. Of the following choices, which is the most appropriate management for this patient?
|
Immediate dental consult to avoid abscess formation
Ellis II dental fracture involves enamel and dentin. The fracture site typically has a yellowish tinge. Ellis III dental fractures are characterized by exposure of pinkish pulp and often blood. These fractures require immediate dental consultation to prevent abscess formation. |
|
|
A 22 year old man is punched in the nose during a fight. He presents to the emergency department with obvious nasal bone deformity. Pressure controls the bleeding. Physical exam reveals no maxillary bone or orbital rim tenderness, intact vision and extraocular movement. The oropharynx and mandible are unremarkable. Nasal inspection reveals a swollen, ecchymotic, tender nasal septum. Which of the following is the most appropriate initial step?
|
Incision and drainage of the septal hematoma followed by nasal packing
Notes: don’t need to consult plastics, can drain hematoma before doing imaging if on PE you don’t suspect more serious facial fractures |
|
|
A 24 year old woman is playing racquetball and sustains a direct blow from the ball to the right eye. She presents to the emergency department complaining of eye pain and double vision. On exam, her right eye does not track properly with upward gaze. This finding suggests which of the following injuries?
|
Inferior (NOT superior) orbital wall fracture
|
|
|
A 32 year old man is struck several times in the head with a baseball bat. Upon emergency medical service arrival, he is mildly confused, vomits once, and complains of a severe headache. The emergency medical technicians establish two large-bore IVs. Prior to arrival at the emergency department, he loses consciousness and begins to seize. He is actively seizing when he is brought into the trauma bay. What should be the first step in the management of this patient?
A. Administration of 2 liters NS bolus B. Administration of phenytoin 1000mg IV C. Rapid sequence intubation using paralytic agent D. Administration of mannitol 50 g IV E. Emergency craniotomy |
C. Rapid sequence intubation using paralytic agent
The airway should be managed as the first priority in this patient. The other maneuvers may be helpful but are secondary to securing an airway and providing oxygenation/ventilation. Airway comes first! |
|
|
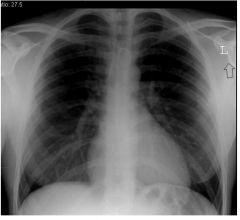
A 46 year old man is brought in by EMS after a motor vehicle collision in which he was an unrestrained driver. Although he has no obvious injury to his head or neck, he complains of chest pain and appears very short of breath. His vital signs are: T 99.2 F, BP 85/57, HR 123, RR 36, SpO2 95% on non-rebreather. The CXR demonstrates a
tension pneumothorax. Of the following, which is the most appropriate next step in this man’s care? A. Placement of a chest tube followed by a chest xray to determine proper placement B. Placement of a needle decompression device, followed by repeat CXR C. Transfusion of 2 units of O-negative packed red blood cells D. Performance of a chest CT scan to further delineate the pathology |
Placement of a needle decompression device, followed by repeat CXR
This patient needs emergent chest decompression and this is rapidly done by needle thoracostomy. A chest CT may be performed, but only once he is stabilized. A formal chest tube will be placed, but placement may not be rapid enough and he may decompensate in the meantime. Transfusion of blood does nothing to correct the physiology of a tension pneumothorax |
|
|
The most sensitive bedside test for nerve injury in a finger after trauma is:
|
two-point discrimination
Light touch is a good screening test, but two-point discrimination is more sensitive and should be used routinely in evaluating injuries to digits. The O’Riain wrinkle test involves placing the digit in warm water and looking for wrinkling of the digital pulps. Presence of wrinkling indicates the nerve is intact. |
|
|
Ottawa ankle rules
|
Ottawa ankle rules are a validated (for adults) set of physical exam findings to determine if an ankle X-ray is needed after an injury
- If any of the first 4 answers is present or if there is tenderness over the navicular or base of the 5th metatarsal, an X-ray should be obtained (1) inability to walk 4 steps at the time of the injury (2) inability to walk 4 steps in ED (3,4) tenderness over medial & lateral malleolus |
|
|
what do you need to know about thoracentesis from the anterior approach (needle decompression)?
|
- second intercostal space along the midclavicular line (NOT midaxillary line)
- If a lateral approach is needed, the recommended insertion site is the 4th or 5th intercostal space in the midaxillary line. The lateral approach poses a greater risk of parenchymal injury. - The needle should always be inserted over the superior edge of the rib as the neurovascular bundle runs along the inferior margin - After the needle is inserted into the pleural space, a rush of air confirms the presence of a tension pneumothorax. - If a tension pneumothorax is confirmed via needle decompression, then a thoracostomy tube should be placed as soon as possible. - An upright chest X-ray should always be performed following a thoracentesis to confirm the successful relief of a tension pneumothorax and the absence of hemothorax or other complications. |