![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
93 Cards in this Set
- Front
- Back
|
What is meant by V/Q matching? |
Ventilation (in L/min) must match the cardiac output (in L/min). Both are approximately equal to 5L/min in humans so that V/Q ≈ 1
|
|
|
Describe the 8 variables quantifying lung volumes. Which ones can be measured with a spirometer? |
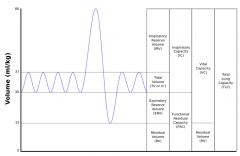
RV, FRC and TLC cannot |
|
|
Why is the Functional residual capacity (FRC) larger than zero? |
Because, during expiration, lung membranes move inwards and chest wall moves outward, creating a negative pressure (< atmospheric pressure) in the intrapleural space which prevents the lung from collapsing.
|
|
|
Name two pathologies that alter FRC and explain how and why they alter it. |
Lung fibrosis ⇒ Increased elastic recoil ⇒ FRC ➘ Emphysema ⇒ Loss of alveolar tissue ⇒ Reduced elastic recoil ⇒ FRC ➚ |
|
|
Name 3 functions of the dead space |
➚ air T°C Filters air ➚ air humidity |
|
|
Define dead space |
Part of the airway not contributing to gas exchange |
|
|
Define anatomical dead space |
all airways upstream from respiratory bronchioles (~ 150mL) |
|
|
Define alveolar dead space |
alveoli that have lost blood supply and hence cannot participate in gas exchange |
|
|
Define physiological dead space |
anatomical dead space + alveolar dead space |
|
|
Formulate alveolar ventilation as a function of tidal volume, dead space and respiratory rate |
VA = (VT - VD - VDA) x RR where VT is tidal, VD is anatomical dead space and VDA is alveolar dead space |
|
|
How does the dead space relate to measurable quantities? |
Bohr’s equation: Vdead/VT = (PaCO2 -PeCO2)/PaCO2, where PaCO2 is the arterial partial pressure of CO2 (the one reaching the alveoli) PeCO2 is the expired partial pressure of CO2. |
|
|
Using Bohr's equation, how can one measure the physiological, anatomical and alveolar dead space? |
Bohr’s equation: Vdead/VT = (PaCO2 -PeCO2)/PaCO2 If PeCO2 is taken as the average over expiration, then Vdead is physiological. Anatomical is taken as the difference between the two. |
|
|
Define minute ventilation |
Tidal volume x Respiratory rate |
|
|
Define alveolar ventilation |
(tidal volume - dead space) x respiratory rate |
|
|
Name two measurable factors that alveolar ventilation depends on and explain how they relate to alveolar ventilation. |
VA = K x VCO2/PCO2 where VCO2 is the amount of CO2 expired every minute and PCO2 is alveolar (or, equivalently arterial) |
|
|
How is CO2 mostly transported in arterial and venous blood? |
As HCO3
|
|
|
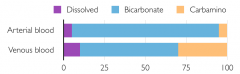
What are the three ways in which CO2 can be transported in the blood? |
HCO3 Dissolved Carbamino haemoglobin |
|
|
In which of arteries or veins is the proportion of CO2 carried as HCO3 higher? What about dissolved CO2? And CO2 as carbamino Hb? |
|
|
|
Name 4 types of hypoxia |
Hypoxic hypoxia: low O2 content in air (e.g. altitude) Anaemic hypoxia: low O2 carrying capacity in blood Circulatory hypoxia: low cardiac output Histotoxic hypoxia: tissues cannot use the O2 delivered to them |
|
|
Express the total amount of gas diffusing at alveoli in a given time as a function of gas properties and blood gas barrier geometry. |
Proportional to A∆t/T x D x (Pin-Pout) where A: Surface area T: Thickness ∆t: Time interval D: Diffusivity of the gas (proportional to solubility) (Pin-Pout): Difference of pressure between alveoli and capillary |
|
|
How does fibrosis affect diffusion at blood-gas barrier? Why? |
Amount of gas diffusing is proportional to: A∆t/T x D x (Pin-Pout) Fibrosis ⇒ thicker blood-gas barrier (T➚) ⇒ V ➘ |
|
|
How does exercise affect diffusion at blood-gas barrier? Why? |
Amount of gas diffusing is proportional to: A∆t/T x D x (Pin-Pout) Exercise ⇒ Cardiac output ➚ ⇒ ∆t ➘ ⇒ V ➘ |
|
|
How does high altitude affect diffusion at blood-gas barrier? Why? |
Amount of gas diffusing is proportional to: A∆t/T x D x (Pin-Pout) Alveolar PO2 ➘ (e.g. high altitude) ⇒ Pin ➘ ⇒ V ➘ |
|
|
What two forces are applied to walls of extra-alveolar vessels? |
Extra-alveolar vessel walls are subjected to two opposite forces: 1) Smooth muscles of the extra-alveolar vessels tend to pull the vessel walls towards each other. 2) Alveolar tissue actively pulls on them to keep them open during lung expansion. |
|
|
How is resistance to blood flow affected by pulmonary blood pressure? Why? |
Resistance decreases when the pressure increases due to : 1) Distension of the capillaries due to increased flow 2) Recruitment of additional capillaries when pressure increases. |
|
|
Why isn't the expiratory reserve volume not zero? |
Because there is an optimum lung volume at which resistance of pulmonary blood vessels is minimum. |
|
|
What determines the blood flow in an area of the lung where the alveolar pressure is higher than the venous pressure? |
The difference between arterial (Pa) and alveolar (PA) pressure: Pa-PA |
|
|
What determines the blood flow in an area of the lung where the alveolar pressure is lower than the venous pressure? |
The difference between arterial (Pa) and venous (Pv) pressure: Pa-Pv |
|
|
Where is perfusion the largest in the lung when a subject is standing up? Why? |
At the base of the lung because arterial pressure increases more than the alveolar pressure as we move down the height of the lung since blood vessels form a continuous tree within which hydrostatic pressure exists. |
|
|
What happens to blood flow in areas that receive less oxygen? |
Hypoxic vasoconstriction PO2 ➘ ⇒ Vasoconstriction ⇒ Resistance ➚ ⇒ Blood flow ➘ |
|
|
What phenomenon explains that, at birth, pulmonary vascular resistance goes down rapidly to allow more blood to reach the lungs? |
Hypoxic vasoconstriction
|
|
|
How can alveolar PO2 be measured? |
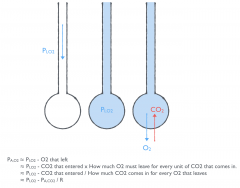
Using alveolar gas equation. |
|
|
Name four causes of hypoxia |
Hypoventilation Challenges to diffusion Shunts V/Q mismatch |
|
|
Name two causes of CO2 retention |
Hypoventilation V/Q mismatch |
|
|
Name 5 causes of hypoventilation |
1. Medulla impairment (e.g. morphine) 2. Spinal cord impairment (e.g. dislocation) 3. Poliomyelitis damaging anterior horn cells 4. Nerve impaired (e.g. damage to the phrenic nerves or Guillain-Barré syndrome) 5. Disease of the neuromuscular junction (e.g. myasthenia gravis) 6. Muscle disease (e.g. muscular dystrophy) 7. Damage to chest wall (e.g. trauma) 8. Obstruction of the respiratory tract |
|
|
Name 2 pulmonary causes of right-left shunts |
Pneumonia Pulmonary oedema (Non-pulmonary: Congenital heart disease) |
|
|
Which hypoxia can be reversed with 100% O2? |
All but shunts |
|
|
How is ventilation distributed in the lung? |
V is higher at the base because intrapleural pressure is less negative at the base and thus apical alveoli are more expanded and have less capacity for further expansion during inspiration. |
|
|
How is V/Q distributed in the lung? |
Q is more affected than V by gravity so that V/Q increases from the base to the apex of the lung. |
|
|
For each of the following quantities, state whether they increase, decrease or remain constant from base to apex of the lung: PO2 PCO2 PN2 O2 concentration CO2 concentration pH O2 inflow [ml/min] CO2 outflow [ml/min] |
Most can be explained by V/Q distribution: PO2 ➚ PCO2 ➘ PN2 ➘ O2 concentration ➚ CO2 concentration ➘ pH ➚ Flows are lower at apex because blood flow is lower: O2 inflow [ml/min] ➘ CO2 outflow [ml/min] ➘ |
|
|
Where in the lung is TB most likely to occur? Why? |
TB is more likely to be present at the apex because the bacteria thrives more in an environment with high O2. |
|
|
Name one pathology that results in a large V/Q ratio and one that results in a low V/Q ratio |
Emphysema: high V/Q (because Q≈0 due to capillaries being destroyed) Bronchitis: low V/Q (because V≈0 due to inflammation of the airway causing obstruction) |
|
|
What two configurations of blood gas can occur in low V/Q? What drives the transition from one to the other? |
Acute: PO2 ➘, PCO2 ➚ Chronic: PO2 ➘, PCO2 normal (PO2 can never return to normal because a low V/Q cannot easily be compensated by a high one) Acute to chronic is driven by chemoreceptors sensing high PCO2 leading to hyperventilation. However, the reverse transition may occur in patients who trade-off the discomfort of hyperventilation for acidosis. |
|
|
Why is the lung important in metabolism? |
Because it receives all the blood. |
|
|
Name two metabolic functions of the lung |
Conversion of Angiotensin I to Angiotensin II Inactivation of bradykinin, serotonin, PG E1, PG E2, PG F2α and noradrenaline |
|
|
Define compliance |
Compliance = ∆V/∆P |
|
|
Name two factors that guarantee lung compliance |
Collagen and elastin (not only through fibers extension but also through changes in geometry) Surfactants |
|
|
Define surface tension and explain how it is related to pressure and radius of a sphere. |
Surface tension is the force applied orthogonally to a unit length of liquid, in the plane of that liquid. Laplace's law: P = 4T/r |
|
|
What produces surfactants? |
Type II pneumocytes |
|
|
Name 3 functions of surfactants |
Stabilises the lung by making the surface tension increase with the relative area Increase compliance of the lung Reduces the chances of alveolar oedema |
|
|
Where in the lung is the intra-pleural pressure highest? |
At the base (when upright position) |
|
|
Draw the volume of alveoli as a function of intrapleural pressure and indicate where on the curve the apex and base of the lung are. |

|
|
|
What is the alveolar volume at the base of the lung when working at RV (instead of FRC)? |

Volume is null because intrapleural pressure at the base of the lung becomes positive so that alveoli collapse.
|
|
|
How does the intrapleural pressure evolve as we breath? |
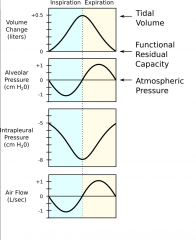
Decreases (more negative) during inspiration to allow the alveoli to dilate. Increases (less negative) during expiration to follow the contraction of the alveoli. |
|
|
How does the intrapleural pressure evolve if we exhale forcedly? |
Increases even more so that part of the lung (at the base) may even have positive pressure. |
|
|
What airways are the principal determinant of airway resistance? |
Most of the resistance comes from medium-sized airways because they are a trade-off between number of airways in parallel (the lower the higher the resistance) and the airway radius (the lower the higher the resistance). |
|
|
How and why does airway resistance vary with lung volume? |
Resistance is inversely proportional to lung volume, because as they expand, alveoli pull on airways through radial traction (exactly as they pull on blood vessels) |
|
|
Name three factors that affect airway resistance. |
Lung volume ➚ ⇒ Resistance ➘ β2-adrenergic receptors ⇒ Resistance ➘ Pollutants (e.g. cigarette smoke) ⇒ Reflex constriction of airways ⇒ Resistance ➚ |
|
|
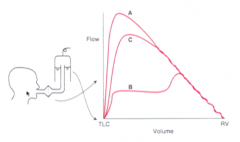
Draw the flow-volume curve during forced expiration. |
|
|
|
What explains the effort-independent region of the flow-volume curve? |

Dynamic compression of airways If intrapleural pressure is positive, then flow is defined by PA-Pintra and not PA-Patm.
|
|
|
How does the point of dynamic compression collapse move in COPD? |
Increase in resistance of small airways ⇒ Increase the spacial rate of decrease of intra-airway pressure so that the point of collapse moves distally towards the alveoli |
|
|
Effect of emphysema on compliance |
Emphysema ⇒ Loss of alveolar tissue ⇒ Reduced elastic recoil ⇒ Lung compliance ➚ |
|
|
Name three types of receptors that are involved in control of respiration and their action |
Central chemoreceptors: senses low pH and high PCO2 and increases RR
Peripheral chemoreceptors: senses PO2 (mostly) and also PCO2 and pH Pulmonary stretch receptors: respond to differences in volume of the lung Irritants receptors: cause bronchoconstriction in respond to irritants Juxta-capillary (J) receptors in alveoli wall: cause rapid shallow breathing |
|
|
Where are central chemoreceptors located? |
Pons and medulla |
|
|
Where are peripheral chemoreceptors located? |
Carotid bodies (signalling via CN IX) and, less importantly in the aortic bodies (signalling via vagus nerve). |
|
|
Compare central and peripheral chemoreceptors in terms of what they sense and their response. |
Central: senses mostly pH and PCO2; stronger slower response Peripheral: senses mostly PO2; weaker and faster response |
|
|
Name four receptors in the lung that control respiration |
Pulmonary stretch receptors Irritant receptors J receptors Bronchial C receptors |
|
|
What prevents the lung from hyperinflating? Which receptors are responsible for that? |
Hering–Breuer reflex mediated by pulmonary stretch receptors signalling to the pons and medulla |
|
|
Name two causes of reduced ventilatory response to CO2 |
Training (e.g. swimming) Increased work of breathing (e.g. obstruction) |
|
|
Why should you not give high flow O2 to patients with COPD? |
In COPD, ventilatory drive is mostly derived from the low PO2 and not the high PCO2 to which they accommodate. Therefore, high flow O2 should not be given to those patients as they may stop breathing. |
|
|
What is the first receptor to drive increased RR when pH is low? |
Peripheral chemoreceptors (central chemoreceptors are more effective but have slower onset) |
|
|
How does the volume of oxygen absorbed per minute [L/min] evolve with exercise power [Watts]? |

|
|
|
Two impacts of carbon monoxide on oxygen content in the blood. |
A.CO binds to haemoglobin reducing the capability of haemoglobin to bind other O2 B. CO increases affinity of O2 to haemoglobin thus reducing the delivery of O2 to tissues by haemoglobin |
|
|
Name three mechanisms through which aerosols deposit in airways. |
Impactation (due to turning point) for large particles Sedimensation (due to gravity) for medium particles Diffusion for small particles |
|
|
Name a representative site for the deposition of aerosols of different sizes: > 5µm, 1-5µm, < 1µm |
> 5µm: impactation in nasopharynx 1-5µm: sedimentation in small airways < 1µm: diffusion in alveoli |
|
|
Briefly outline how the mucociliary system works |
Superficial layer (gel layer) trap the particles Cilia move the gel by touching its base and beating at 20Hz. |
|
|
What produces the mucous in the respiratory tract? |
Mucous gland and goblet cells. |
|
|
Two microstructural features of bronchitis |
Mucous glands grossly hypertrophied thus increasing the thickness of the layer of mucous glands |
|
|
Name three pathologies that may affect the mucociliary function |
Too much mucous (e.g., bronchitis) Change in mucous composition (e.g. cystic fibrosis, asthma) Paralysis of cilia by toxic gas Congenital defect of ciliary motion |
|
|
How can one increase power of exercise past VO2max |
By anaerobic glycolysis |
|
|
Define anaerobic threshold
|
Exercise intensity at which lactate starts to accumulate in the blood |
|
|
Define VO2max |
Maximum rate of oxygen consumption |
|
|
What happens to ventilation [l/min] once the threshold VO2max has been reached? |
Ventilation increases even faster due to detection by chemoreceptors of low pH caused by lactate |
|
|
Name four pathological conditions with low V/Q ratio |
Pneumonia Bronchitis Asthma Pulmonary oedema |
|
|
Name two pathological conditions with high V/Q |
PE
Emphysema |
|
|
What type of acid-base state would you have if you were dropped from a pressurised plane at 4000m of altitude? Why? |
Acute response: Atmospheric pressure ➘ ⇒ Pressure of inspired O2 ➘ ⇒ PO2 ➘ ⇒ Hyperventilation ⇒ PCO2 ➘ ⇒ Respiratory alkalosis |
|
|
What happens to acid-base status and respiratory rate after 2 hours spent at 4000m of altitude? |
Alveolar gas equation: PA,O2 = PI,O2 - PA,CO2/R PI,O2 cannot change R is defined by tissues => Since PA,O2 cannot fall to negative values, there is hypoventilation to reduce PA,CO2. Mechanism: Chemoreceptors detect high pH and decrease RR to decrease pH |
|
|
What happens to Hb and Hb saturation after several weeks spent at 4000m of altitude? |
Hb ➚➚ and O2 saturation ➘ (~ 80%) ⇒ O2 concentration ➚ |
|
|
What happens to O2 dissociation curve at high altitude?
|
Shift to the right at moderate altitude and to the left at very high altitude (because of respiratory alkalosis) |
|
|
Name one physical damage that can occur in the lungs at high altitude. |
High altitude pulmonary oedema Uneven pulmonary vasoconstriction ⇒ Some capillaries are exposed to high pressure ⇒ Damage and leaks |
|
|
What can you do to a patient with CO poisoning? |
Hyperbaric therapy Pt put in high pressure chamber ⇒ PO2 ➚ ⇒ Solubility of O2 ➚ ⇒ O2 concentration ➚ regardless of Hb sat. |
|
|
How does alveolar size evolve along the height of the lung? Why? |
Alveolar size increases from base to apex due to the more negative intrapleural pressure at the apex. |
|
|
What airflow pattern leads to highest airway resistance? |
Turbulent |