![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
242 Cards in this Set
- Front
- Back
|
Two Zones of the respiratory system? |

Conducting & Respiratory |
|
|
Conducting zone is comprised of the ________? |
Nose, larynx, nasopharynx, trachea, bronchi, bronchioles, and terminal bronchioles. |
|
|
Are conducting airways lined with anything? |
Yes, mucus and ciliated cells |
|
|
Walls of the conducting airway contain rough muscle, true or false? |
FALSE They contain smooth muscle |
|
|
The smooth muscle of the conducting airways is parasympathetic or sympathetic? |
Both. |
|
|
Sympathetic system effects of the smooth muscle in the conducting airways? |
B2 receptors on bronchial smooth muscle activate from epinephrine circulating around from adrenal medulla-- > leads to relaxation and dilation of airways |
|
|
Are there any B2 andronergic agnostic activating the bronchial smooth muscle in the sympathetic division? |
Yes, isoproterenol. |
|
|
Within the parasympathetic division, cholinergic neurons activate _________________? |
Muscarinic receptors within the smooth muscle. |
|
|
What happens to the lungs in the parasympathetic division? |
Muscarinic receptors that have been activated by AcetylCholine lead to contraction and constriction of the airways. |
|
|
B2 adrenergic agonists? |
Epinephrine, isproternol, & albuterol. Used to dilate airways (like for asthma) |
|
|
There is smooth muscle in the__________? |
Conducting zone structure and some of the bronchioles and alveolar ducts. |
|
|
Alveoli are ____________. |
Poaches at the terminal end of bronchioles, alveolar ducts, and alveolar sacs. They are thin and have a large surface area for diffusion. |
|
|
There are approximately 300 alveoli per lung, TRUE or FALSE? |
False, there are approx. 300 million |
|
|
What is exchanged through alveoli? |
Oxygen and Carbon dioxide. Exchanged through alveolar gas and pulmonary capillary blood. |
|
|
Exchange of O2 and CO2 through alveoli is slow, true or false? |
False, Occurs rapidly and efficiently. |
|
|
Alveolar cells are lined with? |
Epithelial cells and elastic fibers. |
|
|
Pulmonary blood flow comes from where? |
The right heart. Ejected from right ventricle and goes to the lungs from the pulmonary artery. |
|
|
Pulmonary blood flow process? |
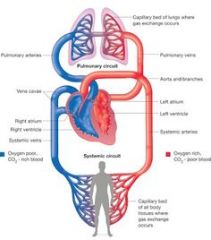
1) Blood goes from the right atrium down to the right ventricle 2) Blood goes out the pulmonary artery into the lungs (CO2 rich, O2 poor) 3) Blood is oxygenated and leaves through the pulmonary veins 4) Oxygenated blood flows through the left atrium and down tot he left ventricle 5) oxygenated blood travels through systematic arteries to the body |
|
|
What forms a dense network around the alveoli? |
Pulmonary capillaries! These carry the deoxygenated blood to the lungs. |
|
|
How is the regulation of pulmonary blood accomplished? |
Altering resistance of the pulmonary arteries. Which is controlled mainly by oxygen. |
|
|
Bronchial circulation is the________. |
Blood supply to the conducting airways & a VERY SMALL fraction on pulmonary blood flow. |
|
|
Tidal volume is _____________. |
Vt Normal, quiet breathing (inspiration and expiration) |
|
|
Volume of tidal volume is ________. |
Approx 200-500 mL Volume of air that fills alveoli AND the volume of air that fills the airway |
|
|
Inspiratory reserve volume? |
Approx. 3000 mL The additional air that can be inspired ABOVE tidal volume. |
|
|
Expiratory reserve volume is the _________. |
Additional air that can be expired BELOW tidal volume. Approx. 1200 mL |
|
|
Is there any air left after maximum expiration? |
Yes, it's residual volume. Approximately 1200 mL |
|
|
What are the different lung capacities? |
Inspiratory, vital, total lung capacity, and functional residual capacity. |
|
|
Inspiratory capacity (IC)? |
Tidal volume (500mL) + inspiratory reserve volume (3000mL) |
|
|
Functional Residual Capacity (FRC)? |
Expiratory Reserve Volume (1200mL) + Residual Volume (1200mL) Volume after normal tidal volume has expired. |
|
|
Equilibrium volume is the ________. |
Volume after normal tidal volume has expired. AKA Functional Residual Capacity |
|
|
Vital capacity (VS) is __________. |
Volume that can be expired AFTER maximal inspiration. Inspiratory capacity (3500mL)+ expiratory reserve volume (1200mL) OR approx. 4700mL |
|
|
What increases vital capacity volume? |
Body size, being male, and physical conditioning. Decreases with age. |
|
|
Total lung capacity (TLC)? |
All the lung volumes. Vital (4700) + Residual (1200) OR 5900mL |
|
|
Which capacities can not be measured by spirometry? |
FRC and TLC. |
|
|
How is FRC measured? |
Helium dilution and Body plethysmograph |
|
|
How does helium dilution work? |
1) Subj. breathes known helium amount which has been added to spirometer. 2) Helium is insoluble in the blood, so the concentration in the lungs becomes equal to that in the spirometer. 3) Amount of helium added to the spirometer and its concentration in the lungs is used to calculate the lung volume. 4) If measurement is taken after normal tidal volume is expired....it's the FRC. |
|
|
Boyle's Law on gases at constant pressure? |
Gas pressure multiplied by gas volume is constant (P X V = constant). |
|
|
Dead space can be both? |
Anatomic or physiologic. |
|
|
Anatomic dead space is the _________________. |
Volume of the conducting airways including the nose and/or mouth, trachea, bronchi, and bronchioles. Approx. 150mL |
|
|
Volume of alveoli? |
Approx. 350mL |
|
|
At the end of expiration the conducting airways are full of? |
Air that has already went through the gas exchange in the alveoli and pulmonary capillary blood. |
|
|
During inspiration of the next tidal volume? |
1) Alveolar air enters the alveoli first but it won't undergo gas exchange (already did) 2) Fresh air from inspired tidal volume (approx. 350mL) which will undergo gas exchange. 3) Rest of tidal volume (150mL) does not make it to alveoli and stays in conducting airways. 4) Leftover tidal volume air is first to be expired and does not have gas exchange. |
|
|
How can you sample alveolar air? |
Sample end-expiratory air (after leftover tidal volume air is expired). |
|
|
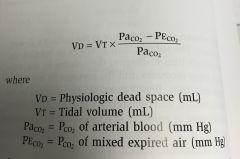
What is the physiologic dead space? |
Total volume of the lungs that does not participate in gas exchange. Anatomic dead space of the conducting airways plus a functional dead space in the alveoli. Ventilated alveoli that DOES NOT participate in gas exchange. |
|
|
Why doesn't ventilated alveoli participate in gas exchange? |
Mismatch of ventilation/perfusin defect. Ventilated alveoli are NOT perfused (blood flow) by pulmonary capillary blood. |
|
|
Example of anatomic dead space? |

|
|
|
The volume of the physiologic dead space is assumed by _______________. |
1) All CO2 in expired air comes from exchange of CO2 in functioning. 2) There is NO CO2 in inspired air 3) Physiologic dead space does not exchange nor contribute to CO2. |
|
|
Equation to calculate physiological dead space? |
|
|
|
Minute Ventilation? |
Total rate of air movement into and out of the lungs. Minute ventilation = Tidal volume X breaths/min |
|
|
Ventilation rate can be expressed as either________or __________. |
Minute ventilation or alveolar ventilation. |
|
|
Alveolar ventilation? |
Corrects for physiological dead space. Alveolar ventilation = (Tidal volume - physiologic dead space) X breaths/min |
|
|
Alveolar Ventilation Equation? |

|
|
|
What does the Alveolar Ventilation Equation look at? |
Inverse relationship between alveolar ventilation and alveolar PCO2. The excretion of CO2 in the expired air. |
|
|
Constant K equals? |
863 mm Hg |
|
|
BTPS is? |
Body temperature (310 K) Ambient Pressure (760 mm Hg) Gas saturated w/ water vapor |
|
|
The higher the alveolar ventilation the more______ is pulled out of the blood and the lower the ____ and ____. |
The more CO2 is pulled out. The lower the PaCO2 and PACO2. |
|
|
When CO2 production doubles then alveolar ventilation must _________. |
Double |
|
|
Why must alveolar ventilation double? |
Because CO2 production doubles and to maintain PACO2 (partial pressure of CO2 in the arteries and alveolar) at 40 mm Hg. |
|
|
Alveolar gas equation is used to? |
Used to predict PO2(pressure of oxygen) based on the alveolar PCO2 (alveolar pressure of Co2) |
|
|
There is more variation in Oxygen pressure than Carbon Dioxide pressure, true or false? |
True |
|
|
Forced Vital Capacity? |
Total vol. of air that can be forcible expired after a maximal inspiration FVC = forced vital capacity= maximal volumethat a person can consciously alter Air within the first second is called FEV1, and so on up to 3 seconds. |
|
|
A normal person can expel _______ % of their vital capacity? |
80% within the first second or forced expiration. |
|
|
How much can someone with asthma expel? |
FVC and FEV1 decreased, but FEV1 is decreased even more than FVC. |
|
|
Why might FEV1 decreased more than FVC, compared to a normal person? |
Increased resistance due to airway obstruction (e.g. asthma) In fibrosis however... FVC is decreased more than FEV1 but in general they are both decreased. |
|
|
The most important muscle for inspiration is the ___________. |
diaphragm |
|
|
During exercise, what other muscles might be engaged for inspiration? |
External intercostal muscles and accessory muscles |
|
|
What is expiration? |
Air being driven out of the lungs by the reverse pressure gradient between the LUNGS and the atmosphere UNTIL it reaches equilibrium again. |
|
|
Muscles involved for expiration? |
Abs (compress abdominal cavity and push diaphragm up) and internal intercostal muscles (pull ribs downward and inward) |
|
|
Ventilatory pump? |
muscles,bones, & connecting tissue (CT) |
|
|
Components of respiratory system? |
Neural, Ventilatory Pump, & the lungs |
|
|
Ventilatory Pump |
Changes volume of chest wall. Air moves in & out of the lung. Connective Tissue |
|
|
Functions of the ventilatory pump? |
•Createthe negative pressure that will bring in the gases (pleural space) •Distributethe gases through the system (workswith the conducting system) •Minimizeenergy expenditure (elastic components of the system) |
|
|
What does elastic tissue do? |
Allows components to expand and recoil. |
|
|
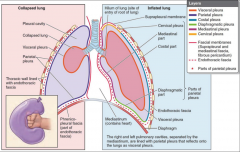
Pleura? |
Membarous surface that coats inside of chest wall |
|
|
Diaphragm contraction does? |
-Pushesdownwardand spreads out, increasing the vertical dimension of the chest cavity anddriving up abdominal pressure. -Thisincreasein pressure drives the abdominal contents down and out, which in turn increasesthe transverse size of the chest cavity. |
|
|
What happens during inhalation in the diaphragm? |
Inhalation –pleural pressure drops - lowers the alveolar pressure, and draws air in down the pressure gradient from mouth to alveoli. |
|
|
What happens during exhalation in the diaphragm? |
–duringquietbreathing is predominantly a passive phenomenon, as the respiratory muscles arerelaxed and the elastic lung and chest wall return passively to their restingvolume, the functional residual capacity. |
|
|
Inhalation basically means... |
pressure drops |
|
|
Quiet inspiration? |
Relaxed breathing •Diaphragmmoves 1 cm & ribs lifted by muscles •Intrathoracicpressure falls and air is inhaled |
|
|
Quiet expiration? |
Passive process...breathing out after breathing in. No muscle action. •Elasticrecoil & surface tension in alveoli pulls inward •Alveolarpressure increases & air is pushed out |
|
|
Labored breathing? |
Inhale Sternocleidomastoid,scalenes& pectoralis minor lift chest upwards as you gasp for air Exhale abdominalmm force diaphragm up–internalintercostalsdepress ribs |
|
|
Air gathers _______ from the other tissues during inspiration. |
Moisture |
|
|
Olfactory epithelium have __________. |
•Olfactorycells are bipolar neurons• •Non-motilecilia on olfactory vesicle• •Nogoblet cells• •Supportingcells• •Stemcells |
|
|
Which capacities and volumes are NOT able to be measured by spirometry? |
Residual volume (RV) cannot be measured by spirometry.Therefore, any lung volume or capacity that includes the RV cannot be measured byspirometry. Measurements that include RV are functional residual capacity (FRC) and totallung capacity (TLC). Vital capacity (VC) does not include RV and is, therefore, measurableby spirometry. Physiologic dead space is not measurable by spirometry and requiressampling of arterial PCO2 and expired CO2. |
|
|
Branches of bronchi? |
Two primary Lobar (secondary) Segmental (tertiary) |
|
|
True or False There is more smooth muscle and elastic fibers in smaller airways? |
TRUE |
|
|
Bronchioles? |
•Nocartilage, smooth muscle in wall is relatively abundant, still no openings intoalveoli |
|
|
Static lung mechanics is the_____? |
Area of lung physiology that deals with the relationships between pressure and volume oflung. |
|
|
Dynamic lung mechanics ______? |
•deal withthe relationships between pressure and flow. |
|
|
Ratio used for pulmonary function test? |
Ratio: Amount expelled in one second/ FVC |
|
|
Volume vs. capacity? |
Volume-single capacity Capacity-Sum of multiple volumes |
|
|
Total lung capacity? |
Sum of all the volumes |
|
|
Vital capacity vs. forced vital capacity? |
Inspiratory reserve volume (IRV), Expiratory reserve volume (ERV), and tidal volume (TV). [everything except reserve volume] Forced is the same thing but forced air.... |
|
|
Inspiratory capacity? |
Tidal volume & the inspiratory reserve volume |
|
|
Functional residual capacity? |
Expiratory & residual volumes |
|
|
The lung is an inelastic structure? |
FALSE |
|
|
What is an elastic structure? |
A structure whose volume is directly proportional to the pressure difference across the wall of the structure |
|
|
Transmural pressure is ____________. |
Internal pressure - external pressure |
|
|
Increased pressure = increased volume but then.... |
As air keeps coming in the ballon (lung) can't get any bigger...so pressure increases. |
|
|
High compliant? |
Lot of volume change for a little pressure change. |
|
|
At very low lung volume,the lung is ________. |
difficult to inflate |
|
|
At very high lung volume.... |
the lung is stiff |
|
|
Hysteresis is? |
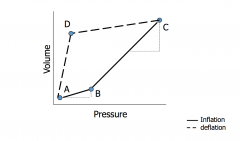
Nonlinear pressure-volume curve of the lung in which transpulmonary pressure at a given volume during inflation is less than the transpulmonary pressure at the same volume during exhalation. |
|
|
The lung is inflated by __________________. |
Changes in pressures inalveolar and pleural spaces relative to atmospheric pressure |
|
|
Alveolar pressure? |
Difference in pressure between the atmosphere and alveoli. Between 0 and positive. |
|
|
Pleural pressure? |
The difference between pressure in the pleuralspace and atmospheric pressure(parietal and visceral membrane). Thorax causes pressure changes. |
|
|
Pressure at the body surface? |
This is usually atmospheric pressure -BUT may change under specialconditions (underwater) |
|
|
Transmural pressure? |
= Alveolar or airway pressure - pleural pressure |
|
|
Pleura and pleural fluid? |
•Maintainspressure differential •Fluidlubricates •Fluidhelps maintain connection between visceral and parietal pleural |
|
|
What creates pressure in the lungs? |
Opposingtensions in the respiratory system |
|
|
When pressure in pleural cavity decreases the lungs_________. |
Expand and this makes the pressure in the alveoli drop (same amount of air but more space). |
|
|
During inspiration what happens to pressures? |
Pleural drops, alveolar drops initially and then rises, & lung volume increase |
|
|
During expiration what happens to pressures? |
Pleural increases, alveolar goes down, & lung volume goes down |
|
|
Injury does what to pleural? |
Becomes equal to atmospheric pressure so NO air flow. |
|
|
How does the chest wall and lungs interact? |
Chest wall (thorax) has a greater volume than lungs. Lungs want to collapse down and the chest wall wants to spring out, so they settle on an intermediate middle. |
|
|
Two type of factors that affect compliance? |
Physical factors and chemical/cellular factors. |
|
|
Physical factors that effect compliance? |
- Anatomy Shape and position of lung - Standing vs lying - Environmental ex. Gravity |
|
|
Chemical/Cellular factors? |
•Cellular secretions •Extracellular matrix |
|
|
Alveoli at the base of the lung... |
not as much gravity, more able to stretch, and exchange more air |
|
|
Why the curves for the lung lines (inspiration and expiration)? |
Effect of surface tension explainsthe difference in the curves between the standard curve of the lungs and fluid in the lungs |
|
|
Surface of alveoli is covered with _______. |
Surfactant |
|
|
Different types of the cell in the alveoli |
Alveolarepithelium: squamous cells (type I) and larger cells (type II - produce surfactant) SomeCT- including ELASTIC FIBERS - between alveolar basal lamina and endothelialbasal lamina Endotheliumof alveolar capillaries Lumenof capillary contains all components of circulating blood |
|
|
Type I cells line the _________. |
Airspace |
|
|
Surface tension is the ________ . |
Attraction between water molecules |
|
|
As surface tension _______, the surfactant becomes more __________. |
decreases, concentrated |
|
|
LaPlace's law? |
The larger the vessel radius, the larger the wall tension required to withstand a given internal fluid pressure. |
|
|
LaPlace Law formula? |
P=2T/r(radius of alveoli) |
|
|
Features of the alveoli pressure... |
Pressure required to inflate smalleralveoli is higher than large ones Air will flow from the small ones to thelarger ones |
|
|
Why don't alveoli's collapse on themselves? |
Surfactant reduces the surface tension Less pressure to maintain the alveoli |
|
|
The Birth process |
1) Lungs filled w/ fluid 2) Fluid coughed up and absorbed during birth. Blood flow increases to lungs. 3) Surfactant decreases surface tension and so less additional pressure is needed to expand the lungs |
|
|
What pressure is required to expand the lungs? |
40-100 cm H2O |
|
|
Small alveolus? |
concentratedsurfactant; surface tension is low so pressure expands it |
|
|
Large alveolus? |
diluted surfactant;surface tension is high so alveoluscontracts. |
|
|
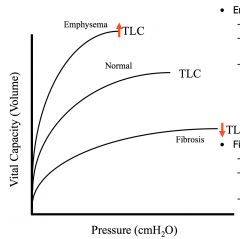
Emphysema? |
Category of obstructive lung disease. Elastic fibers degrade. Enlarged alveoli and reduced ability to recoil. Person can breathe air in but have trouble expelling it. Residual air increases and it becomes harder to let air in. |
|
|
In fibrosis... |
Increased fibrotic material, lungs become hard. Inflammatory response... Connective tissue that is inelastic increases. Lung can't expand. Lung collapses. Hard to get alveoli to expand. |
|
|
Differences in pressure between normal lung, emphysema, and fibrosis? |
|
|
|
Boyle's Law? |
pressure is a function of volume. They are inversely related. |
|
|
What influences how gases move through the airway? |
Shape and Diameter of airway, Rate of flow |
|
|
Two types of gas movements? |
–LaminarFlow: streamline movement of gas atlower velocities. Parallel movement. –TurbulentFlow: (R > 2100) Chaoticmovement that has rapid changes in pressure and velocity. Fluid (gas) is congested. |
|
|
•Airwayresistance greatest in the ______? |
mid-sized airway/bronchi |
|
|
Resistance is? |
Change in pressure and flow. |
|
|
General Gas Law Equation |
Pressure X Volume=Moles(mol) X Gas Contstant X Temeprature |
|
|
Dalton's Law? |
Partial pressure of gas = Barometric pressure X fractional concentration of gas |
|
|
What does Dalton's law mean? |
Partial pressure of a gas in a mixture is same as if it made up the entire substance. Glass of atmosphere pressure and the pressure of oxygen (21% of 760 mm Hg) is the same, even if it was a glass full of oxygen only instead. |
|
|
Henry's Law? |
Concentration of dissolved gas = Partial pressure of has x Solubility # of molecules is proportional to partial pressure of a substance. |
|
|
Henry's Law is involved in... |
looking at substance in the gas form and liquid form (e.g. Oxygen in the alveoli to the blood in the capillaries). |
|
|
At equilibrium the partial pressure of a _______ in the _____ phase equals the partial pressure in the ____phase. |
partial pressure of a gas in the liquid phase equals the partial pressure in the gas phase |
|
|
Fick's Law? |
Diffusion Volume of gas transferred = (Diffusion coefficient of gas X Surface area X partial pressure difference of the gas)/thickness of the membrane |
|
|
In emphysema, what happens to the diffusion capacity? |
Decreases because destruction of alveoli results in decreased surface area. |
|
|
In fibrosis, what happens to the diffusion capacity? |
decreases due to increased distance (membrane thickness) |
|
|
Effusion is? |
The process in which molecules flowthrough a membrane without colliding with other molecules. |
|
|
Smaller molecules effuse ______ than larger. |
faster |
|
|
Graham's law of effusion ignores what? |
The liquid of the alveolar-interstitial |
|
|
Which diffuses faster... CO2 or O2? |
CO2 |
|
|
Do all organs use O2 at the samerate? |
No. |
|
|
Which organs use O2 at a higher rate? |
Heart & brain use it at a higher rate. |
|
|
Mixed Venous |
Systemic carbon dioxide and pH (body organs) |
|
|
Kidney uses a lot of oxygen, true or false. |
False |
|
|
Each hemoglobin molecule binds _______ oxygen molecules. |
Four |
|
|
Alveolar air is not equal in compositionto atmospheric air. Why?
|
1.Dry air is moistened by air passages(water vapor increases) 2.Alveolar air is not completely replacedwith each breath 3.Carbon dioxide is constantly enteringalveolar air 4.Oxygen is constantly exiting alveolar air |
|
|
What are the differences between atmospheric air and alveolar air? |
Alveolar air is comprised of less oxygen and nitrogen, and has less pressure for both oxygen and nitrogen. Increased carbon dioxide and water, as well as pressures for both. |
|
|
Which vascular bed does hypoxia occur? |
Pulmonary |
|
|
Why is arterial pressure of CO2 lower than normal in an asthmatic? |
Hypoxemia causes them to hyperventilate |
|
|
What is mixed venous blood? |
Venous blood that has returned after going to organs |
|
|
Gas exchange during diffusion? |
Across the alveolar/capillary membrane it will occur as long as thepartial pressure difference is maintained. |
|
|
Perfusion and gas exchange? |
Exchangeof gas is limited by the blood flow that has “access” to the alveoli. |
|
|
Molecules must cross through what barriers? |
-from air to fluid - through membrane - layers of cytoplasm - interstitial space -capillary cell -plasma -into red blood cell |
|
|
Movement of oxygen and carton dioxide between alveoli and capillary is by_______. |
simple diffusion |
|
|
Partial pressure of Alveoli for oxygen is higher in the __________ than the ________. |
alveoli, than the capillaries |
|
|
3 different types of gas in the blood? |
1.Dissolved: exerts a partial pressure. Follows Henry’s Law. Nitrogen is the primary dissolvedgas (lowfraction of oxygen is dissolved). 2.Bound Gas: O2/CO2/CO bind to proteins (Hgb and plasmaproteins) 3.Chemically Modified: CO2 ismodified to become HCO3. Most CO2 is transported in the blood in thismethod. |
|
|
Each hemoglobin is comprised of? |
2 beta chains, 2 alpha chains, and four iron hemes (one for each chain), and one oxygen molecule on each iron heme (FOUR total) |
|
|
OxygenHemoglobin Dissociation Curve? |
deoxygenated blood doesn't have a ton of hemoglobin then there's a huge steep increase during oxygenated blood. Hemoglobin curve is not linear |
|
|
Hemoglobinis ____ saturated at venous partial pressure. |
72% saturated at venous partial pressures. It is delivering only 28% of its oxygen load under normal circumstances |
|
|
Variants of hemoglobin? |
•Methemoglobin: Fe component is Fe3+ (instead of 2+)•Cannot bindwith O2•Causesinclude nitrites and sulfonamides •FetalHgb (HbF): (2 gamma subunits, no beta) differ from adultà increased affinity for O2 (from placenta). •HgS(sickle cell): (defect of beta subunits) In deoxygenated state, HgS polymerize, causing a change in shape. |
|
|
*Oxygencarrying capacity of Hgb is? |
1.34 mL/g Hgb |
|
|
Formula for determine oxygen in the blood? |
•Theamount of oxygen in the blood =•[1.34 x Hb x(SaO2/100)] + 0.003 x PO2 SaO2 is saturation |
|
|
P50 is? |
•P50: is the Po2 at which hemoglobin is 50%saturated (i.e.,where two of the four hemegroups are bound to O2). |
|
|
Anincrease in P50 reflects a ________ in affinity. |
decrease |
|
|
A decrease in P50 reflects an _______ in affinity. |
increase |
|
|
PO2 of 60 gets you ______ saturation. |
90% |
|
|
Women tend to have _______ hematocrit. |
37/38-42 |
|
|
Anemic people have more or less oxygen in the blood. |
Less |
|
|
P50 is used as an indicator for what? |
affinity for O2 |
|
|
Decreased affinity is a ____ shift. |
Right |
|
|
Increased affinity is a _______shift. |
Left |
|
|
Decreased affinity means that? |
Hemoglobin releases oxygen easily. |
|
|
pH of tissues is? |
7.2 |
|
|
pH of lungs is? |
7.6 |
|
|
Shift to right indicate? |
Decreases affinity for oxygen. Increased CO2 Increased glycolysis Increased temperature Increased Hydrogen ions |
|
|
What moves airflow? |
Normal mechanical (bellows for a fireplace) and in the alveoli it is diffusion (short distances) |
|
|
V/Q means |
Ventilation/Perfusion of air in the lungs |
|
|
Shunt is? |
Non-Oxygenated blood |
|
|
How do shunts occur? |
Physiological dead space Physiological blood, bronchial blood flow or coronary circulation that drains left side of heart |
|
|
Right to Left Shunt? |
When blood from right heart bypasses lungs, so it doesn’t get oxygenated. Mostly seen in newborn and congenital defects. |
|
|
Left to Right Shunt? |
Bloodrecirculates through the lungs after being oxygenated. Highoxygen blood from left ventricle and it pushes it to the right to go back tothe lungs. So just recycled already oxygenated blood. Ex. Hole in the heart |
|
|
Physiologic Shunt can be increased by? |
Several pathologic conditions --> ventilation (V)/perfusion(Q)mismatch. |
|
|
Gasexchange is optimal in alveoli when? |
Ventilation is closely matched to blood flow or perfusion. |
|
|
Theideal ventilation (V) to perfusion (Q)ratio is between? |
Theideal ventilation (V) to perfusion (Q)ratio is between 0.8 to 1.0. This is based on the entire lung. |
|
|
If, anaverage adult male at rest breathes approximately 4,000ml – 4,500ml of gas perminute and the average cardiac output from the heart is 5,000ml per minute...what's the V/Q ratio? |
4,000/5,000=.8 |
|
|
Perfusion is? |
Rate of blood being sent to the body, cardiac output |
|
|
Ventilation/Perfusion mismatch examples? |
Mechanical (ventilator machine), Alveolar (poorly perfused), Anatomical (dead space) |
|
|
Examples of shunt? |
Perfusion without ventilation Lung obstruction (e.g. kid swallows a lung) Pneumonia (i.e. lung full of pus and mucous and the alveoli are plugged up, no air space available) |
|
|
Blood flow obstruction? |
Blood doesn't reach alveoli so ventilation is wasted, dead space ventilation |
|
|
Blocked ventilation causes? |
Increased CO2 and decreased oxygen Sleep Apnea is another example or certain opioids |
|
|
Blocked perfusion causes? |
Increased oxygen and decreased CO2 |
|
|
Thedifference between the expected and actual PaO2 iscalled the ________? |
Alveolar-arterial oxygen difference (A-aDO2 or A-a Gradient) Difference between oxygen in alveoli and arteries |
|
|
NormalA-a gradient is _________ |
<15 mm Hg |
|
|
Hypoxemia? |
abnormally low arterial oxygen tension in the blood. |
|
|
Levels for Hypoxemia? |
Normal is 80-100 mm Hg Severe <40 Elevated •Abnormal O2 transfer •Hypoxemia due to diffusion impairment, ventilation-perfusion inequalities, or shunt |
|
|
Hypoxia? |
underoxigenation, inadequate level of tissue oxygenation for cellular metabolism. |
|
|
Types of hypoxia? |
Hypoxic Hypoxia: altitude, V/Q mismatch, shunt, or hyperventilation Hyperemic Hypoxia: anemia Circulatory Hypoxia: poor blood flow Histoxic Hypoxia: poor use of oxygen by cells, e.g. poisoning. |
|
|
Hypoxemia with normal A-a gradient? |
Problem is not with oxygen transfer but instead the supply of oxygen in the alveolus. could be due to atmospheric pressure changes (being underwater, mountain, enclosed spaces) |
|
|
Hypoxemia with increased CO2? |
Increasedpartial pressure carbon dioxide decreases partial pressure of oxygen in alveoli Hypoventilation |
|
|
Hypercapnic Respiratory failure? |
•Decreasedminute ventilation •Suppressionof the neural drive to breathe•acuteor chronic hypoventilation and hypercapnia TOO much CO2 gets in the blood, either making too much or not getting rid of it •Drugs- narcotics/sedatives |
|
|
COPD or emphysema leads to? |
Lessexchange of oxygen and CO2, can become hypoxic and hypercapnic |
|
|
Asthma leads to? |
Inflammationleads to constrictionàless oxygen in alveoli. |
|
|
Fibrosis leads to? |
Lotof fibrosis in between capillaries and alveoli. Diffusion gets messed up, soCO2 can’t diffuse across thicker membrance |
|
|
When checking for a shunt if the pt is put on 100% oxygen, you should expect to see the PO2 at? |
700 mm Hg because 60 (of the 760) is deadpsce |
|
|
For every _____ mmHg below 700, estimate a ___ shunt. |
100 mm Hg below, a 5% shunt |
|
|
Have a patient that you give 100% oxygen to and their blood oxygen is 400 mmHg, is there a shunt and if so...what is it? |
Yes, because 400 is less than 700. 700-400 = 300 300/100=3 3*.05 = .15 or 15% = Shunt |
|
|
DRG is the? |
Dorsal respiratory group(inside medulla) |
|
|
DRG does what? |
•Receiveinput from thorax and abdomen regardingpO2 and pCO2 •Communicatewith pre-motor neurons connected to diaphragm •Integrate with the VRG Drives inhalation |
|
|
Who are the three primary controllers for respiration? |
medulla, apneustic center, and pnemotaxic |
|
|
VRG is the? |
Ventral Respiratory Group |
|
|
Functions of the VRG? |
inspiratoryand expiratory – largely quiescent during quiet breathing •powerfulexpiratory signals to abdominals during exercise •larynxand pharynx control/dilation •Integrationwith DRG (Botzinger complex) |
|
|
How is the VRG affected by the cerebral cortex? |
Fear, excitement, etc. |
|
|
VRG is located in the? |
Pre-Botzinger complex |
|
|
Features of Pre-Botzinger complex? |
Has a pacemaker activity This is easily overridden by conscious control and the DRG input. |
|
|
Pons is thought of as? |
Finishing off/inhibitory respiratory site.
|
|
|
Apneustic Center? |
Part of pons. Prolonged inspiratory gasps. |
|
|
Pnemotaxic Center? |
Part of pons. Turns off inspiration. Limits AP in phrenic nerve. |
|
|
Respiratory Control Center sensors? |
Central chemoreceptors: Hydrogen ions Peripheral chemoreceptors: Oxygen, carbon dioxide, and hydrogen ions. Pulmonary receptors: Stretch Going and muscle receptors: Stretch and tension |
|
|
Peripheral chemoreceptors are in the? |
arterial system |
|
|
Chemical chemoreceptors act upon the? |
diaphragm |
|
|
Peripheral chemoreceptors act upon the? |
Inspiration and external intercostal muscles. |
|
|
Pulmonary Receptors act upon the? |
Accessory muscles and Expiration. |
|
|
Joint and muscle receptors act upon the? |
Internal intercostal muscles and abs. |
|
|
Breathing is controlled by ____ and ___ response to the diaphragm. |
afferent and efferent |
|
|
MOST important sensory input is? |
PaO2, PaCO2, and Arterial pH |
|
|
CO2 and the chemoreceptors? |
CO2 diffuses easily across the vessel wall but H+ and HCO3 donot. CO2releasesHCO3 and protonswhich lower the pH of CSF and stimulatestheactivity of the chemoreceptors. |
|
|
CO2 is actually measured by the________. |
Number of protons it generates |
|
|
Peripheral receptors? |
primarily driven by oxygen levels |