Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
122 Cards in this Set
- Front
- Back
|
Microscopic appearance of alveoli in pulmonary edema
|
Pink fluid in normally clear alveolar spaces, hyperemia. Septal edema can involve widening of the alveolar septum.
|
|
|
General (3) causes of pulmonary thromboemboli
|
1. Stasis
2. Immobility 3. Hypercoagulable states |
|
|
Sources of pulmonary thromboemboli
|
Deep leg veins, then pelvic veins
|
|
|
Appearance of a thrombus with Lines of Zahn
|
|
|
|
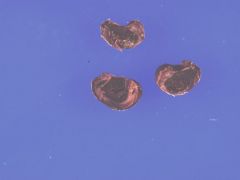
Gross appearance of a hemorrhagic infarct and pulmonary arterial thromboembolism
|

|
|
|
Etiology of pulmonary hypertension
|
Primary: lung vascular disease, chronic hypoxia, bad genes, abnormal mediators inflammation, unknown.
Secondary: cardiac, IV drug abusers, autoimmune diseases, herbs |
|
|
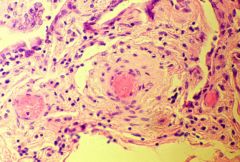
Appearance of a highly constricted arteriole in pulmonary hypertension showing MARKED MEDIAL HYPERTROPHY.
|
|
|
|
Pulmonary alveolar proteinosis
|
Heavy edema due to either a congenital lack of surfactant or an acquired state due to silicosis, immunodeficiency, or cancer. PAS positive
|
|
|
Histologic appearance of pulm. alveolar proteinosis
|
The alveoli will be chock-a-block full of a protein-lipid-granular precipitate.
|
|
|
Angiofibroma
|
Benign tumor of sinonasal area -- a testosterone dependent highly vascularized tumor that can kill you if it expands into the cranial cavity. BLEEDS LIKE CRAZY.
|
|
|
Histologic appearance of an allergic inflammatory polyp
|
What you'd expect -- eosinophils red and mast cells blue.
|
|
|
Names and classifications for benign nasal papillomas
|
Schneiderian, transitional, squamous
1. Exophytic: septal 2. Endophytic: lateral |
|
|
What virii are nasal papillomas associated with?
|
HPV 6,11.
|
|
|
Path lab list of malignant sinonasal tumors
|
SCC, TCC, adenocarcinoma, undiff carcinoma, neuroblastoma and neuroendocrine (characteristics are in Robbins, and probably later in these notecards)
|
|
|
Race and age distribution of nasopharyngeal carcinomas
|
Asians, either 15-25 or 60-69. The survival rates at 5 years are good but the tumors are recurrent
|
|
|
Can nasopharyngeal cancers lack lymphocytic infiltrates?
|
Yes.
|
|
|
Common viral and genetic associations with nasopharyngeal cancers.
|
EBV-DNA, HLA-2, HLA-BW46
|
|
|
Histologic appearance: small tumor cells in a sea of lymphocytes
|
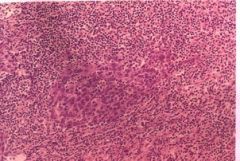
Undifferentiated nasopharyngeal carcinoma
|
|
|
Children have many and adults, few. Benign are associated with HPV 6,11 ... and malignant 16,18. Are they cancerous?
|
Squamous papillomas of the sinonasal tract. Potential carcinoma development in 15 years because they are difficult to get rid of.
|
|
|
General precursors to SCC in respiratory system.
|
Like other squamous cancers...either keratoses or squamous dysplasia.
|
|
|
Predominant carcinoma of the larynx?
|
Squamous
|
|
|
Clinical presentation of laryngeal carcinoma
|
Hoarseness, pain, dysphagia, hemoptysis, stridor . . . etc.
|
|
|
What determines survival rates in laryngeal carcinoma?
|
Where the cancer is and whether it hits the local lymph node. The common locations are supraglottic, glottic and subglottic. . .
|
|
|
The rule of 95%.
|
95% of lung neoplasms are malignant cancer. 95% of those metastasize. BAD NEWS.
|
|
|
Accrding to the ancient chart in our notes . . .
|
People develop lung cancer most frequently in their 7th decade of life, men more than women.
|
|
|
Major characteristics of squamous cell carcinoma of the lung
|
1. Smokers
2. Central bronchi 3. Very low 5-yr survival rate 4. Met to peribronchial lymph nodes and liver. |
|
|
Gross appearance of lung leukoplakia
|

|
|
|
Gross appearance of Lung SCC
|

|
|
|
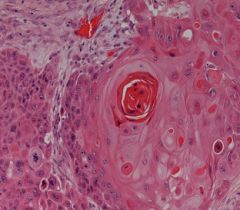
Keratin pearl appearance in keratinizing invasive SCC.
|
|
|
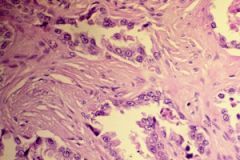
Characteristics of adenocarcinoma
|
1. Still mostly smokers
2. Glandular neoplastic elements with destructive fibrosis. KEY. 3. Early metastasis. |
|
|
Glands glands glands of adenocarcinoma
|
|
|
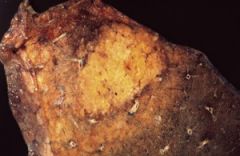
Characteristics of bronchioalveolar carcinoma
|
1. 71% smokers
2. Peripheral, pneumonia-like appearance 3. Lepidic growth (crawls along the walls, not into them) with NO DESTRUCTIVE FIBROSIS |
|
|
Bronchioalveolar carcinoma -- note the consolidated, pneumonia-like appearance. Will also appear on x-rays as hazy consolidation near periphery of lung.
|
|
|
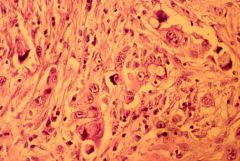
Characteristics of large cell undifferentiated carcinoma
|
Like all undiff cancers, VERY HIGH STAGE AND BAD PROGNOSIS
1. Peripheral 2. Epitheloid, spindle, clear 3. Mets wherever the hell it wants to. |
|
|
Undiff large cell carcinoma - note pleomorphic cells are no organization.
|
|
|
General characteristics of carcinoid tumors
|
More atypical cells, mitoses, necrosis.
|
|
|
How do you tell the difference between a large-cell undiff carcinoma and large-cell neuroendocrine carcinoma
|
Endocrine will palisade and be positive for neuroendocrine markers
|
|
|
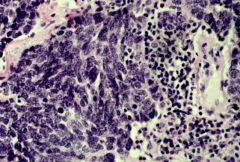
Characteristics of small-cell lung carcinoma
|
1. Aggressive and metastatic
2. SMOKERS 3. Non-surgical 4. TTF-1, CD56, synaptophysin |
|
|
Small cell lung carcinoma, ewww....
|
|
|
Characteristics of solitary fibrous tumor of the pleura.
|
1. Hyaline fibrosis, spindle cells
2. Unrelated to asbestosis |
|
|
Characteristics of malignant mesothelioma
|
1. More men than women, 6th-9th decade of life.
2. Non-pleuritic chest pain 3. Paraneoplastic hypoglycemia, ADH. |
|
|
Gross appearance of malignant mesothelioma
|
1. Occasionally hemorrhagic pleural effusions
2. Multiple pleural nodules that coalesce over time. |
|
|
Microscopic indicators of malignant mesothelioma
|
1. Mucin neg
2. WT-1, calretinin, CK 5/6 positive 3. BER EP4, CEA, TTF-1 negative |
|
|
Two morphological appearances of mesothelioma
|
1. Epitheloid
2. Spindle (Sarcamoid) |
|
|
General risk factors for lung cancer (Markus lecture)
|
Smoking, obstructive lung disease, passive smoke, relative, pulmonary fibrosis, air pollutants, radon
|
|
|
When does risk for lung ca decrease? When does it return to 80-90% nonsmoking level?
|
5 yrs. 15 yrs. It will never return to normal.
|
|
|
Do you increase your risk of mesothelioma with asbestos and smoking? What about lung ca?
|
No. The combination does not carry increased risk over asbestos exposure alone. For lung ca, the two are independent risk factors.
|
|
|
Frequency of non small cell carcinomas
|
Adeno - 30%
SCC - 25% LCC - 15% Bronchoalveolar - 5% (although technically this is an adeno carcinoma) |
|
|
Frequency of small cell carcinoma
|
25%
|
|
|
Peripheral involvement, early mets, DIC, hypertrophic pulmonary osteoarthropathy
|
Adenocarcinoma
|
|
|
Central involvement, common hilar complications, obstructive, cavitation, late mets, superior sulcus, hypercalcemia (from PTH), clubbing
|
SCC
|
|
|
Hylar mass, widened mediastinum, early and terrible mets, SIADH (hyponatremia, fluid overload), Eaton-Lambert
|
Small cell carcinoma
|
|
|
Peripheral, ill-defined mass, common hilar complications, rapid growth, early mets, clubbing
|
Large cell carcinoma (remember that ALL large cell cancers grow quickly, because they don't differentiate or organize)
|
|
|
Multicentric, consolidatory, lepidic growth and pneumonic features
|
Bronchoalveolar cancer
|
|
|
Do adenocarcinomas respond well to chemo/radiation?
|
No, it's better to catch them before met and surgically excise them, if possible. If you have symptoms, it's too late.
|
|
|
Solitary nodule vs. diffuse
|
Adenocarcinoma general vs. bronchoalveolar adenocarcinoma
|
|
|
Best prognosis of all lung cancer if a solitary nodule
|
Bronchoalveolar carcinoma
|
|
|
1-yr survival rates of bronchoalveolar carcinoma
|
80% if resected.
|
|
|
Bronchorrhea
|
Copious sputum production, a characteristic of bronchoalveolar (which is growing along the alveolar walls anyway)
|
|
|
Tx for SCC
|
Resect if at all possible, responds better to chemo/radiation than adenocarcinomas
|
|
|
Cancers that show cavitations and necrosis
|
SCC, Large Cell Carcinoma
|
|
|
Where are you most likely to find small cell carcinomas?
|
Perihilum/hilum (80%)
|
|
|
Can you surgically resect small cell carcinoma?
|
No.
|
|
|
Paraneoplastic syndromes of small cell carcinoma
|
SIADH, ACTH overproduction (Cushing's), and Eaton-Lambert
|
|
|
Do small cell carcinomas respond to chemotherapy?
|
Yes! But they recur, hence the worse prognosis.
|
|
|
Symptoms of mesothelioma
|
Dyspnea, chest wall pain, bloody effusion, spontaneous pneumothorax
|
|
|
Thrombocytosis, clubbing
|
Paraneoplastic findings of mesothelioma
|
|
|
Tx of mesothelioma
|
Pleurodectomy, with talc pleurodesis and the usual chemo/rad. You will still die within the year.
|
|
|
Presents most commonly in adults < 40 yrs of age.
|
Carcinoid tumor
|
|
|
Sx of carcinoid tumor
|
Hemoptysis and cough.
|
|
|
Cushing's, HTN (due to incr. ACTH), hypercalcemia
|
Carcinoid
|
|
|
Can secrete neurotransmitters like serotonin and has other NE markers
|
Carcinoid. (small cell carcinomas also frequently have secretory granules and systemic paraneoplastic effects)
|
|
|
Palisading histology
|
Carcinoid
|
|
|
Octrotide scan, serum chromgranin A2 blood test
|
Carcinoid
|
|
|
Percentage symptoms at time of diagnosis:
1. Local 2. Regional 3. Systemic mets 4. Paraneoplastic and constitutional |
1. 70%
2. 15% 3. 10% 4. 10%, but 40% will have either weight loss or chest pain. |
|
|
Number 1 symptom of lung cancer, followed by several other prominent ones
|
#1: Cough
-Hemoptysis, Dyspnea, pneumonia, lymphangitic dissemination, wheezing |
|
|
Regional effects of lung CA
|
Pleural/pericardial effusions, hoarseness, SVC syndrome (small cell), brachial plexus involvement (Horner's syndrome, Pancoast tumor)
|
|
|
Sx of Pancoast tumor
|
Supraclavicular mass, shoulder pain, ulnar distribution pain, rib involvement and of course Horner's syndrome
|
|
|
Horner's syndrome
|
Miosis, Ptosis, Anhydrosis.
|
|
|
SVC Syndrome Sx
|
Facial edema, JVD, huge central mass on X-ray, emergent intervention
|
|
|
SIADH, Increased ACTH leading to hypokalemia, calcitonin excess
|
Small cell carcinoma (adenocarcinoma will also present with calcitonin excess)
|
|
|
Hypercalcemia (due to PTH)
|
SCC, carcinoid
|
|
|
Gynecomastia (increased FSH)
|
large cell, adenocarcinoma
|
|
|
Anti-calcium channel antibody
|
Eaton-Lambert: associate with small cell
|
|
|
Cerebellar ataxia
|
squamous
|
|
|
Focal neurologic signs -- are they paraneoplastic or metastatic?
|
Mets!
|
|
|
When is a coin lesion benign?
|
Young, no growth or only grows every 16 months, (popcorn, laminated, central, diffuse) calcifications, well-marginated, smaller than 2 cm
|
|
|
When is a coin lesion malignant?
|
Older, doubles in 6 mos, (eccentric, stippled) calcfication, irregular margins, larger than 3cm
|
|
|
What is the TNM system? Who doesn't follow this rubric?
|
(Tumor, Nodes, Metastases) -- T is size and location, N is location, M is either yes or no. Small cell carcinomas have a different system
|
|
|
Small cell staging
|
Is either limited or extensive.
|
|
|
How do you stage a tumor?
|
CT, or MRI for superior sulcus. Can tell you T and N
|
|
|
How do you stage T, N, and M all at once?
|
A PET scan. The accuracy is very high, but you can't see the brain or kidney (already high metabolic activity)
|
|
|
How do you evaluate performance status?
|
Karnofsky score: you can look this up on Wikipedia.
|
|
|
Why would you want a head CT?
|
10% of small cell tumors present with cranial mets
|
|
|
Examples of surgical diagnostic techniques
|
MEDIASTINOSCOPY, T Biopsy, bronchoscopy, transthoracic needle aspiration, thoracentesis
|
|
|
Bronchoscopy sensitivity in endobronchial disease vs. peripheral
|
88% vs. 69% with all procedures, and it helps the sensitivity if the tumor is larger than 2 cm.
|
|
|
Sensitivity of Transthoracic Needle Aspiration
|
90%, but not needed for single lesion, straight to surgery
|
|
|
Satisfactory Pre-Op FEV. Questionable? Bad?
|
> 2L! from 1-2 L requires a perfusion scan. < 1L is unacceptable.
|
|
|
Other pre-op pulmonary measurements to consider
|
CO2, DLCO, O2 saturation, exercise performance.
|
|
|
General trend of Tx and TNM staging
|
Early stages -- mix of surgery if possible with chemo and radiation. As the stages rise, surgery will not be possible, and radiation will no longer be effective.
|
|
|
Tx for limited stage small cell carcinoma
|
Chemo and XRT
|
|
|
Tx for extensive stage small carcinoma
|
Chemo
|
|
|
Is screening useful for lung CA?
|
Apparently not. Both a bias in screening and the lack of accurate met detection contribute to no apparent drop in mortality.
|
|
|
Top met to lung
|
Breast. Followed by other lung, renal cell, malignant melanoma
|
|
|
Main head and neck cancer. Others?
|
Squamous cell carcinoma. Adenocarcinoma of salivary glands, undiff muconasal carcinoma.
|
|
|
5 basic areas of head and neck region.
|
oral cavity, pharynx, larynx, tongue and paranasal sinuses, major salivary glands
|
|
|
Risk factors for head and neck cancer
|
Alcohol (dose dependent) and of course smoking/smokeless tobacco. Combined effect is multiplicative. Also, viral infections via interfering with tumor suppressor gene fxn.
|
|
|
EBV
|
Endemic nasopharyngeal cancer
|
|
|
Virii associated with head and neck cancers
|
EBV, HPV, HIV, HSV
|
|
|
Early Sx for head and neck cancer
|
Epistaxis, non-healing ulcers, nasal obstruction, jaw swelling, lymphadenopathy, dysphagia, hoarseness
|
|
|
Staging criteria for head and neck cancer
|
TNM
|
|
|
Indications for postop radiation HNC therapy
|
Involved surgical margins, perineural involvement, bone/cartilagenous invasion, advanced disease, extracap lymph node extension.
|
|
|
Dominant oncogenes involved in lung CA
|
c-MYC, K-RAS, EGFR, and HER-2/neu
|
|
|
Inactivated tumor suppressor genes involved in lung ca
|
p53, RB, p16INK4a, and multiple loci on chromosome 3p
|
|
|
Different genetic alterations in small cell vs. non-small cell
|
small cell cancers harbor more frequent alterations in c-MYC and RB, whereas non-small cell tumors are associated with mutations in RAS and p16INK4a
|
|
|
highest frequency of p53 mutations of all histologic types of lung carcinoma
|
SCC
|
|
|
2 types of bronchoalveolar carcinoma
|
Mucinous and nonmucinous. They do not usually manifest glandular elements.
|
|
|
Why do small cell carcinomas appear angry?
|
Basophilic staining of vascular walls due to encrustation by DNA from necrotic tumor cells
|
|
|
Do small cell carcinomas evidence neuroendocrine features
|
Yes! 2/3rds of presenting cases will have neurosecretory granules . . . and if you think about the paraneoplastic (SIADH and ACTH) of small cell, you can imagine this would be true.
|
|
|
Neuroendocrine markers tested for in lung CA
|
chromogranin, synaptophysin, and Leu-7
|
|
|
What is a DNES tumor smaller than a carcinoid?
|
Tumorlet.
|
|
|
Typical carcinoids
|
No p53 mutations or BCL2/BAX imbalance
|