![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
43 Cards in this Set
- Front
- Back
|
features of acute severe asthma |
PEF 33-50% best or predicted |
|
|
features of life threatening asthma |
PEF <33% best of predicted |
|
|
medical management of acute severe / life threatening asthma |
Oxygen to maintain SpO2 94-98% |
|
|
clinical features for PE on Wells' criteria |
Clinical signs and symptoms of DVT (minimum of leg swelling and pain with palpation of the deep veins) |
|
|
clinical probability score required for PE likely on Wells' criteria |
More than 4 points |
|
|
If PE likely (>4 Wells Score), what's the next line of investigation? |
CTPA and then treat if positive. If CTPA negative, consider leg USS for possible DVT |
|
|
If PE unlikely (≤ 4 Wells Score), what's the next line of investigation? |
1. D-dimer test |
|
|
Management of small (<2cm), simple pneumothorax |
observe in A&E for 4 to 6 hours with supplemental high-flow oxygen |
|
|
Management of large (≥2cm), simple pneumothorax |
Percutaneous aspiration using cannula and syringe |
|
|
Management of acute exacerbation of COPD |
Controlled oxygen therapy - aim for sats 88-92% |
|
|
Causes of interstitial lung disease - groups |
idiopathic, occupational, chronic allergy (EAA), autoimmune, iatrogenic |
|
|
occupational toxins associated with ILD |
hairdressing sprays, silica, asbestos, coal dust |
|
|
Causes of chronic Extrinsic Allergic Alveolitis |
pigeon breeding, mouldy foliage (farmers), wood dust |
|
|
Autoimmune conditions associated with ILD |
RA, SLE, scleroderma, dermatomyositis, sarcoidosis |
|
|
iatrogenic causes of ILD |
radiation, methotrexate, bleomycin, nitrofurantoin, amiodarone |
|
|
chest findings in idiopathic pulmonary fibrosis |
fine, end-inspiratory crackles reduced chest expansion bilaterally |
|
|
causes of transudative pleural effusion |
Cardiac failure |
|
|
causes of exudative pleural effusion |
Bacterial pneumonia |
|
|
diagnostic features of pleural tap for exudate |
protein >30 g/dL, LDH >200 u |
|
|
CURB-65 score |
confusion, urea >7, respiratory rate >30, BP <90/60, age > 65 years |
|
|
when to consider hospital treatment for pneumonia |
CURB-65 ≥ 2 |
|
|
commonest pathogen for pneumonia |
Streptococcus pneumoniae (60-75%) |
|
|
antibiotic management of moderate/severe pneumonia (CURB-65 2-5) |
Amoxicillin IV + clarithromycin PO for 3-5 days |
|
|
causes of localised bronchiectasis |
infective - severe pneumonia, TB |
|
|
causes of generalised bronchiectasis |
Cystic fibrosis Marfan's |
|
|
features of bronchiectasis on CT |
bronchial dilation The signet ring sign |
|
|
criteria for immediate (without CXR) lung cancer referral (2ww) |
chest X‑ray findings that suggest lung cancer OR aged 40 and over with unexplained haemoptysis |
|
|
criteria for urgent CXR to assess for lung cancer |
age >40 ≥2 unexplained symptoms ≥1 unexplained symptoms & (ex-)smoker symptoms: cough fatigue shortness of breath chest pain weight loss appetite loss |
|
|
test used to assist in diagnosis of asthma |
Bronchial challenge test with methacholine Asthmatics will react to lower doses of drug |
|
|
Indications for long-term oxygen therapy in patients with COPD |
1. PaO2< 7.3 kPa when stable OR 2. PaO2 7.3-8 kPa when stable and one of: secondary polycythaemia nocturnal hypoxaemia peripheral oedema pulmonary hypertension |
|
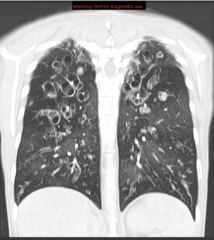
CT thorax |
bronchiectasis |
|
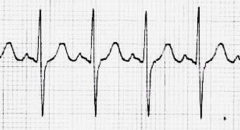
Which lung condition? |
Pulmonary hypertension - RVH, right axis deviation, p-pulmonale (peaked p waves), tall R waves in V1, right ventricular strain |
|
|
causes of pulmonary hypertension |
Left heart failure COPD Chronic pulmonary emboli Sickle cell disease Pulmonary fibrosis |
|
|
causes of type I respiratory failure |
pneumonia pneumothorax pulmonary oedema pleural effusion PE |
|
|
causes of type II respiratory failure |
Acute: asthma, foreign body, Guillan-Barre, opioid toxicity Chronic: COPD, MND, pulmonary fibrosis |
|
|
type II respiratory failure on ABG |
respiratory acidosis low PaO2 Raised PaCO2 |
|
|
causes of respiratory alkalosis |
hyperventilation (anxiety, excess mechanical ventilation, compensatory ventilation in acidosis) |
|
|
Stepwise treatment for asthma |
1. SABA 2. SABA + ICS (400 mcg/day) 3. SABA + ICS + LABA 3b. if LABA fails, add leukotriene receptor antagonist or theophylline 4. increase ICS up to 2000 mcg/day, consider addition of 4th drug 5. oral steroid + refer |
|
|
definition of COPD in lung function tests
|
FEV1/FVC < 0.7 |
|
|
COPD severity according to FEV1 |
Mild: FEV1 >80% Moderate:FEV1 50-80% Severe:FEV1 30-50% Very severe:FEV1 <31% or respiratory or right heart failure |
|
|
treatment of COPD according to severity |
Mild: SABA/SAMA as required Moderate (FEV1>50%): LABA Severe (FEV1<50%): LABA + ICS Very severe (FEV1<31%): LABA + ICS + LAMA |
|
|
SAMA |
ipratropium, tiotropium |
|
|
LABA |
formeterol, salmeterol |