![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
46 Cards in this Set
- Front
- Back
|
Alveoli |
-Delicate -Type 1 pneumocytes most susceptible to injury |
|
|
Type 2 pneumocytes: |
Make the surfactant, and make Type 1 and 2 pneumocyte |
|
|
Alveoli damage |
AS long as BM is intact, Type 2 pneumocyte division can proceed with repair. |
|
|
Alveolar epithelialisation |
Diffuse forms of alveolar injury can take on the appearance of a gland. |
|
|
Hyaline Membranes |
Microscopic eosinophilic bands formed by a combination of pulmonary surfactant and plasma proteins which can leak into the alveoli following injury to Type 1 pneumocytes and alterations in BBB. |
|
|
Pneumonia |
Inflammation in alveoli and alveolar walls. |
|
|
Classifications of Pneumonia |
1. Bronchopneumonia: suppurative 2. Bronchopneumonia: fibrinous 3. Bronchointerstitial 4. Interstitial 5. Granulomatous 6. Embolic |
|
|
Bronchopneumonia |
Inflammation on bronchi bronchioles adjacent alveoli lumens *Originates from terminal bronchioles. |
|
|
Bronchopneumonia Common Causes |
Bacterial Mycoplasma infections Aspiration of foreign material |
|
|
Suppurative Bronchopneumonia |
Neutrophils Cellular debris Macrophages *in airway and alveolar lumen |
|
|
Bronchopneumonia Consequences |
1. Resolution 2 Progression to Chronic Suppurative BP |
|
|
Chronic Suppurative Bronchopneumonia |
1. Bronchioectasis 2. Pulmonary abcessation 3. Plueritis and adhesions 4. Atelectasis or overinflation 5. BALT hyperplasia |
|
|
Fibrinous Bronchopneumonia |
More severe, sudden death, associated toxemia. aka Lobular Pneumonia: involvement of entire lobes and pleural surface. *Less likely to resole--> fibrosis and adhesions. |
|
|
Interstitial Pneumonia |
Inflammation in ALVEOLAR WALLS, not spaces. From blood borne insult or direct aerogenous injury. Diffuse damage. Protein and fluid exudation--> hyaline membrane formation. EXUDATIVE PHASE--> PROLIFERATIVE PHASE (lots of Type 2pn) |
|
|
2 types of Interstitial Pneumonia |
1. Acute Interstitial Pneumonia 2. Chronic Interstitial Pneumonia |
|
|
Acute Interstitial Pneumonia |
1. Transient (viral) 2. Severe and associated with life threatening pulmonary oedema |
|
|
Chronic Interstitial Pneumonia |
Dominated by fibrosis of alveolar walls. Proliferation of Type 2 Pn. |
|
|
Interstitial Pneumonia: Fog fever/ Bovine pulmonary emphysema and oedema |
Adult beef cattle in autumn Change in pasture L-typtophan ingestion Metabolised to 3 methylindole --> bloodsteam ---> lungs |
|
|
Interstitial Pneumonia: Paraquat Poisoning |
Lesions range from acute lesions to chronic. NECROSIS OF THE ADRENAL ZONA GLOMERULOSA AND RENAL TUBULAR EPITHELIUM. |
|
|
Embolic Pneumonia |
Haematogenous spread of infections into the lung. No orientation around airways. Mostly in caudal region. Inflammation mainly around pulmonary arterioles or alveolar capillaries. |
|
|
Granulomatous Pneumonia |
Dominated by macrophages +/- giant cells Lymphocytes Neutrophils |
|
|
Pulmonary abcesses can be a consequence of |
1. Septic emboli in pulmonary vessls 2. Extension from severe focal supurative bronchopneumonia 3. Aspiration of foreign material 4. Direct penetration |
|
|
Species specific aspects |
See pp. 85-87 |
|
|
Equine influenza |
Mild bronchointerstitial pneumonia |
|
|
Equine viral rhinopneumonitis |
Milk bronchointersitial pneumonia |
|
|
Rhodococcus equi. |
Foals or immunosuppressed adults. Cause SEVERE BRONCHOPNEUMONIA. *It is taken up by macrophages and survives in them. *Becomes suppurative bronchopneumonia and abcess formation *Leads to necrosis |
|
|
Bovine Shipping/Transit Fever |
Pasteurellosis. Nasopharyngeal and oral regions. Due to stress/virus. |
|
|
Bovine Enzootic Pneumonia |
Due to viruses/mycoplams. Bacterial involvement makes it worse. Clinically mild, lesions of bronchointerstitial pneumonia. |
|
|
Bovine TB |
M. tuberculosis or M. bovis Granulomatous where bacteria survive in macrophages. |
|
|
TB events that follow... |
1. Primary complex - primary infection of lungs - involvement of regional lymph nodes. -Starts as small tubercles in dorsocaudal subpleural areas which progress to larger confluent areas of caseous necrosis. 2. Mycobacteria can disseminate via lymphatics... MILIARY TB. |
|
|
Bovine respiratory syncitial virus (RSV) |
Associated with winter housing. Cranioventral atelectasis and consolidation. Interstitial emphysema in caudal lung lobes. Bronchoconstriction due to mast cell degranulation and histamine release. |
|
|
Canine parainfluenza |
Paramyxovirus. Acute. Actions: Replicates in airway epithelial cells.. Bronchitis bronchiolitis Alveoli infection |
|
|
Canine distempter virus CDV |
Catarrhal oculonasal discharge Pharyngitis Bronchitis Targets lymphoid tissue. Resultant immunosuppression. Predisopsed to secondary bacterial infection. |
|
|
Ovine Maedi visna virus/ aka Lymphoid Interstitial Pneumonia |
Pulmonary lesions develop very slowly. Uncommon. Lungs are large, mottled, grey. Enlarged lymph nodes. Histologically: extensive lymphoid proliferation and smooth muscle hyperplasia. |
|
|
Sheep Pasteurellosis |
Lambs Late spring, early summer. Same as shipping fever for cattle. |
|
|
Porcine Respiratory and Reproductive syndrome PRRS |
Respiratory and reproductive failure. Transient loss of appetite. Slight hyperthermia. Respiratory distress. |
|
|
Porcine Enzootic Pneumonia |
Lesions of bronchopneumonia: suppurative or catharral. Confluent consolidation of cranioventral lung lobes. Economically highly significant. |
|
|
Pasteurellosis in pigs |
Severe acute fibrinous pneumonia Chronic suppurative bronchopneumonia with abcessation and pleuritis. |
|
|
Aspergillus fumigatus |
Cause of aspergollosis. Significant in BIRDS. Due to inhalation of mouldy feed/bedding. Immunodeficiency. Grossly: multiple discrete grey/white nodules. Blood vessels can become involved in lesions. Invasion, hemorrhage, thrombosis. |
|
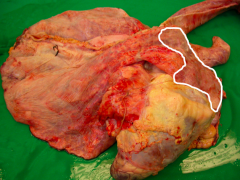
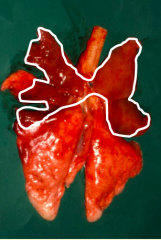
What pattern is this? |
Suppurative bronchopneumonia. |
|
Most common causes? |
Bacteria, mycoplasma. |
|
What cells characterise this? |
neutrophils, cell debris, macrophages. |
|
|
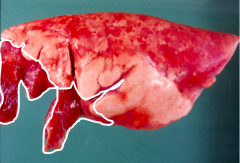
What are the consequences of bronchopneumonia? |
1. Resolution 2. Progress to a more chronic suppurative bronchopneumonia |
|
|
What are the features of a chronic suppurative bronchopneumonia? |
Bronchiectasis Pulmonary abcess Pleuritis Adhesions Atelectasis |
|
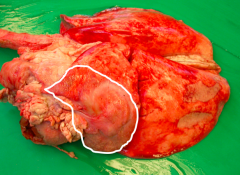
What is this? |
Fibrinous bronchopneumonia More severe, sudden death Involve entire lobes and pleural surface. Fibrosis and adhesions, less likely to resolve quickly. |
|
|
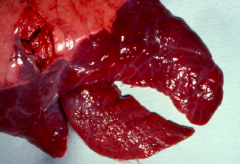
Aerogenous. Hard. |