![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
37 Cards in this Set
- Front
- Back
|
Squamous Papilloma |
verruca vulgaris/wart of nasal vestibule |
|
|
Sinonasal (Schneiderian) Papillomas *3 types* |
Uncommon, Benign neoplasms (but locally destructive) 1. Exophytic (septal,squamous) ~50-60% 2. Inverted (lateral,squamous) ~40-50% 3. Oncocytic (lateral,cylindrical/columnar) ~5-10% |
|
|
Exophytic Sinonasal Papilloma (Septal, Squamous, Fungiform) |
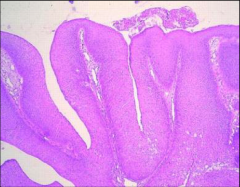
- Occurs on septal nasal wall - Rarely (almost never) develops into invasive carcinoma - Looks like fingers off the septum |
|
|
Inverted Sinonasal Papilloma |
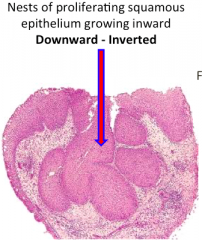
- Occurs on lateral nasal wall near middle turbinate - 5-10% develop invasive carcinoma within 5 years |
|
|
Oncocytic Sinonasal Papilloma (Cylindrical, Columnar) |
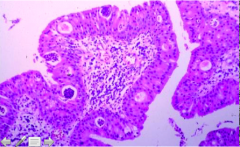
- Occur on Lateral nasal wall near middle turbinate - No assx w/ HPV - Oncocyte = abundant bright pink cytoplasm (from mitochondria in this tumor) |
|
|
Olfactory Neuroblastoma (Esthesioneuroblastoma) |
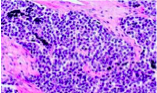
- Arises from neuroectodermal olfactory cells in olfactory mucosa - Average age onset bimodal- 15 and 50 y/o - 5-year Survival = 40-90% - obstructive - Superior nasal concha, upperseptum, roof of nose, cribriform plate, ethmoidsinus - "Small blue cell" tumor |
|
|
Three Major Divisions of the pharynx |
1. Nasopharynx (*NK) 2. Oropharynx 3. Laryngopharynx *NK = “non-keratinizing” (no cornified layer) |
|
|
Lymphoid structures in the Upper “Airway” |

- "Waldeyer'sring" (left) - which includes Palatine tonsils - Lymphocytes in the lamina propria (Submucosal dense lymphoid aggregates) |
|
|
What will obstruction of the internal auditory canal in the Nasopharynx cause? What about in the upper airway? |
Recurrent otitis media --> hypertrophicadenoidal tissue --> Obstruction ofthe internal auditory canal Obstruction inupper airway --> Sleep apnea |
|
|
Nasopharyngeal Angiofibroma (NA) |
- Epidemiology = rare - Occurs almost exclusively in young males (often redheads) - onset 10-20 years (rare>30); “Juvenile NA” - Sx = epistaxis - Clinical Behavior: Posterolateral wall fibromuscular stroma origin - Benign, but 10-20% are locally aggressive and 9% are fatal - Tx = surgery - Prognosis = Excellent after removal |
|
|
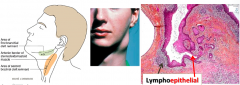
Nasopharyngeal Carcinoma *3 histo subtypes* |
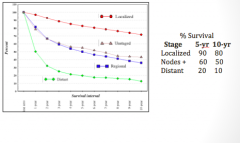
- Epidemiology = EBV-related - Africa: Common in children (not adults) - China: Common in adults (not children) - Rare in U.S. - Freq. unresectable at diagnosis, Five year survival (after Rx) 60% 1. Keratinizing - squamous cell carcinoma (SqCC) 2. Nonkeratinizing- squamous cell carcinoma3. Undifferentiated/basaloid carcinoma,with lymphoid component* |
|
|
What is "Pharynx –Oropharynx". What occurs here? |
Not really part of airway; represents posterior portion of oral cavity - this is where Acute Pharyngitis “Beefy Red” & Acute Tonsillitis hits . In either, think Adenovirus [ds-DNA]. Viral infections by far most common cause of AP |
|
|
Group A Streptococcus (GAS) |
- 10-20% of pharyngitis ages 5-15 yrs - Rare in adults - Incidence peaks winter-early spring - Sore throat + fever - Absence of cough, coryza, hoarseness, conjunctivitis •(these suggest a virus) - Tender anterior cervical lymph nodes - Tonsils are enlarged, erythematous and have patchy exudate (follicular tonsillitis) |
|
|
Fusobacterium necrophorum |
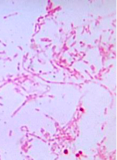
- ~10% of acute pharyngitis cases - >20% in recurring cases and in peritonsillarabscesses - Jugularvein with thrombophlebitis (Lemierre syndrome) |
|
|
Corynebacterium diphtheriae |

- Only strains carrying toxgenecausediphtheria - Gene encodedwithin a lysogenic bacteriophage - Diphtheria - Productionof pseudomembrane |
|
|
ViralPharyngitis |
- Rhinoviruses(~20%) - Indirectpharyngitis. - Adenoviruses - Cancause pharyngoconjunctivalfever (fever,sore throat, conjunctivitis). - EBV - Infectious mononucleosis mainlyin 15-25 yr-oldage group, Monospottest for heterophile antibodies. - HSV types I and 2- Gingivitis, stomatitis and pharyngitis, vesicles inpharyngeal mucosa - Influenza - Pharyngitis - Parainfluenza andcoronaviruses- pharyngitis aspart of common cold syndrome - Enteroviruses(certain coxsackieand echovirus)-pharyngitis secondaryto upper GI infection and then dissemination - CMV &HIV – Mononucleosis-typeillness |
|
|
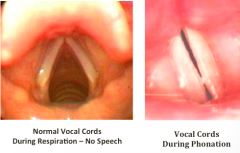
How to vocal cords move during phonation? |
|
|
|
Anatomy of the Laryngopharynx/Hypopharynx& Larynx |

|
|
|
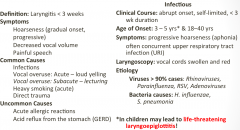
Discuss Acute Laryngitis |
|
|
|
Croup/ Laryngotracheitis / Laryngotracheobronchitis |
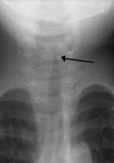
• MC cause of inspiratory stridor (laryngealor supraglottic obstruction)in children • Oftenassociated with seal-like barking • Cause - Mainlyparainfluenza (paramyxovirus) • Steeple sign – subglottic narrowing • Pathogenesis = Infx via aerosol into nasopharynxand spread to larynx and trachea•Edemaand inflammation in subglottic larynx and trachea around cricoid cartilage –airway narrowing. May haveendothelialdamage and loss of ciliaryfunction. Fibrinous exudate may beformed andaddto airway occlusion•Edemaof vocal cords can cause hoarseness • Treatment = Supportivewith short termsteroids to reduceinflammation. |
|
|
Reinke Edema (PolypoidCorditis) |
Middle-aged females who are heavy smokers --> Develop husky low-pitched weak voices |
|
|
Vocal Cord NodulesandPolyps |
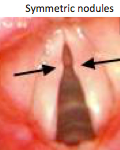
- Pathogenesis:Reaction to injury of vocal cord - Classic location at junctionanterior and middle third of cord - Occurs following sustainedinjury causedby Heavy smoking Heavy, recurrent voice strain (singer’snodules)“Theyvirtually never give rise to cancers” |
|
|
VocalCord Papilloma and Papillomatosis |
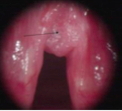
- Papillomas: Benignneoplasms locatedon true vocal cords - Usuallysinglein adults, but can be recurrent - Multiple in children (juvenile laryngeal papillomatosis) - Causedby HPVtypes 6/11 |
|
|
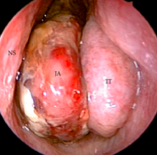
SquamousCell Carcinoma of Larynx |
- ClinicalFindingsProlongedhoarseness (>6 wks) earliest,most consistent Sx - Epidemiology= ~90%have a prolonged and significant history of Heavy smoking,>20 years (> 50 pack yrs) + Ethanol abuse/dependence |
|
|
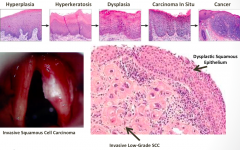
Squamous Cell Carcinoma of Larynx (Premalignant Changesand InvasiveCarcinoma) |
|
|
|
Location of Laryngeal Carcinoma |
Anatomic locations 1. Glotticcarcinoma:involvesthe true vocal folds 50-60%oflaryngeal carcinomas 2. Supraglotticcarcinoma: confinedto the supraglotticarea (free border of the laryngeal epiglottis, false vocal folds and laryngealventricles) 30-40%oflaryngeal carcinomas Discovered later– early tumors do not causehoarsenessHigher stage tumors at diagnosis- 2/3StageIIIor IV 3. Subglottic carcinoma:extendor arise more than 10mmbelow the free marginofthe true vocal fold up to the inferior border of the cricoid cartilage. <5%of laryngeal carcinomas 4. Transglotticcarcinoma:cross the ventricle from the supraglotticarea to involve the true and false vocal folds or involve the glottis andextend subglotticallymore than 10mm orboth. Glottictumors:5 yrsurvival ~65% Supraglottictumors:5 yrsurvival ~45% |
|
|
Squamous Cell Carcinoma Larynx - Survival by Stage |
|
|
|
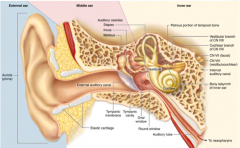
Anatomy of the Ear |
|
|
|
External Ear and Otic (Aural) Canal |
Otitis Externa •Marked tendernessafter gentletractionof pinna •Peak age between 7-12 •Physical Findings: erythema,swelling, moist debris +/-pus •Etiology: Traumatized ear canal• excessive use cotton-tip swabs• retained contaminated water“Swimmer’sEar” •Bacterial -90% • PseudomonasSp 38 - 50% • StaphylococcusSp • Gram-negativerods • Fungal 10% •Aspergillus • Candida Neoplasms = Simplyskin tumors; i.e. squamous and basal cell carcinoma |
|
|
Middle Ear Anatomy |
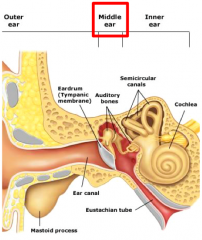
Middle ear is linedby thin “non-keratinizing” stratified squamous epithelium |
|
|
Middle Ear Inflammatory Disorders - Acute OtitisMedia |

Tympanic membraneopacity, bulging , erythema, effusion and decreased motility |
|
|
Middle Ear Inflammatory Disorders - Chronic Otitis Mediaand Cysts |
ChronicOtitis Media: when Eustachian tube becomesblocked repeatedlyCauses:Recurrent otitis media (> 3/6 mo; 4/yr) with adenoid hypertrophy Bacterialagents: Pseudomonasaeruginosa, S. aureusLong-termsequellae:Perforationtympanic membrane, scarring, mastoiditis and bone erosion, cysts; conductive hearing loss common Middle ear cysts (0.5 - 3 cm) Two types of cyst lining 1.Squamous epithelium (cholesteatoma):large amounts of keratin produced 2.Metaplastic columnar epithelium: mucin-secreting |
|
|
Cholesteatoma |
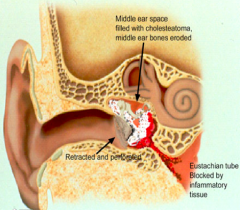
Squamous epitheliumtrappedwithin thetemporal bone(middle earor mastoid) |
|
|
Otosclerosis |
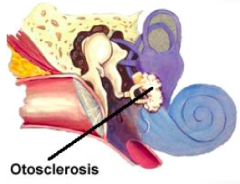
Bony overgrowth --> severe conductive hearingloss |
|
|
Neck- Branchial Cleft Defects |
|
|
|
Neck - ThyroglossalDuct Cysts |

Cystin midlinelocationAnyage (usually<40) |
|
|
Neck- Carotid Body Tumor |
- Prototypeof parasympathetictumor --> With↓pO2 carotid bodyreleasesneurotransmitters that↑ ventilatory rate - Bruit on auscultation duetoobstruction and turbulent flow |